
Abstract
Background:
Depth of anesthesia may be insufficient in pediatric cardiac anesthesia if a total intravenous anesthetic regimen with opioids and midazolam is used during cardiopulmonary bypass. The advantages of sevoflurane-based balanced anesthesia may be (1) a more graduated regulation of the depth of anesthesia during cardiopulmonary bypass and (2) a reduction in postoperative ventilation time for children in comparison with total intravenous anesthesia.
Aim:
To evaluate a possibly positive effect of sevoflurane-based balanced anesthesia in children undergoing cardiac surgery we analyzed whether this anesthetic regimen had a significant effect related to (1) depth of anesthesia, (2) the need for opioids during cardiopulmonary bypass as well as on postoperative characteristics such as (3) time of postoperative ventilation, and (4) duration of stay in the intensive care unit in comparison with total intravenous anesthesia.
Methods:
In a retrospective analysis, data from heart-lung machine protocols from 2013 to 2016 were compared according to anesthetic regimen (sevoflurane-balanced anesthesia, n = 70 vs. total intravenous anesthesia, n = 65). Children (age: 8 weeks to 14 years) undergoing cardiac surgery with cardiopulmonary bypass were included. As a primary outcome measure, we compared Narcotrend® system–extracted data to detect insufficient phases of anesthetic depth during extracorporeal circulation under moderate hypothermia. Postoperatively, we measured the postoperative ventilation time and the number of days in the intensive care unit. Furthermore, we analyzed patients’ specific characteristics such as opioid consumption during cardiopulmonary bypass. Regression analysis relating primary objectives was done using the following variables: anesthetic regimen, age, severity of illness/surgery, and cumulative dosage of opiates during cardiopulmonary bypass.
Results:
No significant differences were observed in descriptive patient characteristics (age, body weight, height, and body temperature) between the two groups. Further, no significant differences were found in depth of anesthesia by analyzing phases of superficial B1-C2-electroencephalography Narcotrend® data. No marked difference between the groups was observed for the duration of postoperative intensive care unit stay. However, the postoperative ventilation time (median (95% CI, hours)) was significantly lower in the sevoflurane-based balanced anesthesia group (6.0 (2.0-15.0)) than in the total intravenous anesthesia group (13.5 (7.0-25)). A higher dosage of opioids and midazolam was required in the total intravenous anesthesia group to maintain adequate anesthesia during cardiopulmonary bypass. Regression analysis showed an additional, significant impact of the following factors: severity of illness and severity grade of cardiac surgery (according to Aristotle) on the primary endpoint.
Conclusion:
In children undergoing cardiac surgery in our department, the use of sevoflurane-balanced anesthesia during cardiopulmonary bypass showed no superiority of inhalational agents over total intravenous anesthesia with opioids and benzodiazepines preventing phases of superficial anesthesia, but a marked advantage for the postoperative ventilation time compared with total intravenous anesthesia.
Keywords
Introduction
Intraoperative awareness is rare but possible during anesthesia. The most common risk factors for intraoperative awareness are (1) young age, (2) anesthesia during cardiac surgery, and (3) an insufficient depth of anesthesia. 1 Therefore, children undergoing cardiac surgery represent a group of patients at increased risk for insufficient depth of anesthesia and thus possibly intraoperative awareness. During cardiopulmonary bypass (CPB), when ventilation is stopped, a balanced anesthesia with inhalational agents is not readily possible and even in phases of ventilation during CPB, the level of lung perfusion is restricted; consequently, the concentration of inhalational anesthetic in patients’ blood would be reduced. Thus, the use of inhalation anesthesia was limited during CPB in the past, for technical reasons, and many medical centers in Germany preferred a high-dose opioid anesthetic regimen supplemented with flunitrazepam or midazolam (total intravenous anesthesia, TIVA). For this reason, until 2015, our department also used TIVA with fentanyl and midazolam during CPB.
According to modern surgical techniques, a deep hypothermia, which per se reduces the need for anesthetics, is no longer necessary. Today, many operations can be performed under moderate hypothermia or normothermia. However, under these conditions maintaining a sufficient level of anesthesia may not be guaranteed exclusively with high-dose opioids, benzodiazepines, and alpha-receptor-agonists, thus also fulfilling point (3) as a risk factor for intraoperative awareness. 2
Consequently, questions concerning the need and the adequate use of anesthesia under the aforementioned conditions still need to be addressed.
As a consequence and in our opinion, balanced anesthesia supplemented with opioids and a modern inhalational anesthetic, for example, sevoflurane, would constitute a better anesthetic regimen for most children undergoing cardiac surgery under CPB. Sevoflurane can be added via the oxygenator of the heart-lung machine during CPB and guarantees adequate hemodynamic stability and a good controllability.3,4
Whether the balanced anesthesia regimen with sevoflurane in children undergoing cardiac surgery during CPB under hypothermia is associated with an adequate depth of anesthesia, measured by an age-related algorithm of Narcotrend® data, compared with TIVA has to our knowledge not yet been investigated and therefore represents the aim of this study.
Methods and measurements
Study population: inclusion and exclusion criteria
The retrospective study was conducted after receiving permission from the Ethical Committee of Heidelberg University (S-498/2015).
All patients aged from 8 weeks to 14 years of age undergoing cardiac surgery with CPB at our institution between October 2013 and November 2016 were included in this study. The administration of sevoflurane during CPB became available in May 2015 and was used exclusively thereafter. Because we included n = 65 children in the TIVA group from October 2013 to May 2015, in the sevoflurane group we included a comparable number of children (n = 70) with the same inclusion criteria for the time period from May 2015 to November 2016.
Those children aged <8 weeks alone were not included in the data analysis. The age-related limit of 8 weeks was defined relating to the manufacturers’ instructions for electroencephalography (EEG)-monitor description. In children with age <8 weeks, the reliable measurement of adequate anesthetic depth with Narcotrend® is not possible. In total, 135 patients were included in this retrospective study.
Narcotrend®
As a reliable assessment of the depth of hypnosis during sedation and general anesthesia, EEG is currently a subject of interest. One possibility for detecting brain activity during anesthesia is the EEG-Narcotrend® system (Monitor Technik, Bad Bramstedt, Germany). The Narcotrend® algorithm is based on a pattern recognition of the raw EEG and classifies the EEG epochs in different stages—from A (awake) to F (very deep depression, increasing burst suppression down to electrical silence). A superficial anesthesia is defined as phase B1-C2 (corresponding to 89-65). Using the actual Narcotrend® index, the newest version 1.8 was implemented in the EEG monitor.
However, for this study we used retrospectively recorded Narcotrend® data for achieving the aims of this study.
Objectives
We used the EEG-Narcotrend® monitor to define phases of insufficient anesthesia such as Narcotrend® phases B1-C2 (superficial anesthesia) as our main objective.
During the period of extracorporeal circulation we measured:
The cumulative time of Narcotrend® superficial anesthesia (B1-C2 phases) and
The number of Narcotrend® superficial anesthesia (B1-C2 phases).
In addition, we calculated the percentage of cumulative time of Narcotrend® A-B0 (awake) and B1-C2 (superficial anesthesia) phases in relation to the duration of extracorporeal circulation.
Further, we recorded patient-related data such as age, body weight, height, American Society of Anesthe-siologists (ASA) Physical Status Classification, main diagnosis, kind and severity of cardiac surgery, the medication dosage (midazolam, opioids), the duration of the extracorporeal circulation period, and patients’ body temperature during this phase. From intensive care unit protocols we listed the mortality, the time of postoperative ventilation, and duration of the stay in the intensive care unit. Under the assumptions such as mortality, ventilation time over 168 hours, and prolonged stay in intensive care unit over 336 hours were not primarily related to the cardiac surgery or the type of anesthesia but rather to perioperative conditions and postoperative complications, we analyzed these objectives in intensive care unit only up to a maximum of 7 and 14 days, respectively.
Anesthesia and monitoring
Children aged more than 6 months received premedication orally with midazolam 0.5 mg/kg half an hour before they were transferred to the operation area.
After attaching the standard monitoring regimen, anesthesia was induced with midazolam 0.1 mg/kg, fentanyl 5-10 µg/kg, propofol 2 mg/kg, or etomidate 0.2 mg/kg, depending on the nature of the heart defect and cisatracurium 0.2 mg/kg. To some patients, however, sufentanil or remifentanil and piritramide, instead of fentanyl, was administered after discretion by the anesthesiologist. After nasotracheal or orotracheal intubation, the patient’s lungs were ventilated to achieve normocarbia and an arterial oxygenation according to the nature of the heart defect. Anesthesia was maintained age-adapted 5 with sevoflurane (Baxter Inc., Deerfield, IL, USA) 0.5-1 minimal alveolar concentration and repetitive doses of fentanyl. Neuromuscular blockade was maintained with cisatracurium 0.2 mg/kg/hour.
An arterial cannula was inserted into the radial or femoral artery and a central venous catheter via the right internal jugular vein or, in single ventricle pathology, via the femoral vein.
Three blue sensor electrodes (Ambu® GmbH, Bad Nauheim, Germany) were attached to the skin of the face, one above the root of the nose and two besides the eyes. Name and date of birth of the patient were inserted into the Narcotrend® monitor and the cables of the monitor were attached to the electrodes. After testing for appropriate skin resistance, the measurement was started. In addition, two near-infrared spectroscopy optodes (INVOS®) were attached to the skin of the forehead for bilateral near-infrared spectroscopy monitoring during the operation.
Anesthesia during CPB
Group “sevoflurane”
Anesthesia was maintained with sevoflurane via the oxygenator of the heart-lung machine at a concentration to maintain the Narcotrend® stage D0. During the phases on extracorporeal circulation with ventilation of the lungs (partial bypass), sevoflurane was given at the same inspiratory concentration as via the oxygenator of the heart-lung machine. Sevoflurane administration was stopped when the anesthetic level reached Narcotrend® E2 or below. Analgesia was performed with repetitive doses of fentanyl (3-5 µg/kg) and neuromuscular blockade with cisatracurium 0.2 mg/kg/hour.
Group “TIVA”
Anesthesia was maintained with repetitive doses of midazolam (0.1 mg/kg) and fentanyl (5-10 µg/kg), with the aim to sustain Narcotrend® level at D0. Neuromuscular blockade was performed with cisatracurium 0.2 mg/kg/hour.
Criteria for extubation conformed to the German guidelines for artificial ventilation. 6
Statistics
This retrospective study was designed as a hypothesis-generating pilot study.
Patient characteristics and outcomes are presented in tables as or median with first and third quartiles with 95% CI for continuous parameters; absolute and relative frequencies are reported for categorical variables. Outcome parameters were compared between the TIVA and sevoflurane groups using a Mann–Whitney U test as the data were not normally distributed.
In addition, regression analyses were conducted to adjust patients’ age, ASA classification, amount of applied opiates, and severity grade. The grade of severity of surgery (1: low, 2: moderate, and 3: severe) was defined as shown in Appendix Table 5. To better understand the assumption of linear regression analysis (normally distributed residuals), the logarithm of the outcome variables is considered except for the cumulative time of Narcotrend® A-B0 and B1-C2 phases/extracorporeal circulation time, which was not logarithmized. Data were analyzed using SPSS (IBM, Version 21.0) and R (Version 3.5.0). 7
Results
Study collective
Children aged <8 weeks were excluded in the data analysis (n = 12). Because of incomplete data set, we excluded four patients. In total, 135 patients were included in this retrospective study. Thus, we analyzed 70 data sets of sevoflurane-based anesthesia and 65 data sets of TIVA.
In the sevoflurane group, the time on extracorporeal circulation was 1 hour and 47 ± 46 minutes (mean ± SD, 00:29:39-5:09:04, 95% CI). Two children died after surgery: one child at 7 days after surgery and the other child 89 days after surgery, both without a relationship of anesthesia during surgery. In the TIVA group, the time on extracorporeal circulation was 1 hour and 42 ± 36 minutes (mean ± SD, 00:36:55-05:36:43, 95% CI). None of these children died. Patient characteristics are given in Table 1. The proportion of low, moderate, and severe severity grades were similarly distributed. In both groups, no prolonged phases (>1 minute) of Narcotrend® A-B0-defined awareness (awake) were obtained.
Patient characteristics.
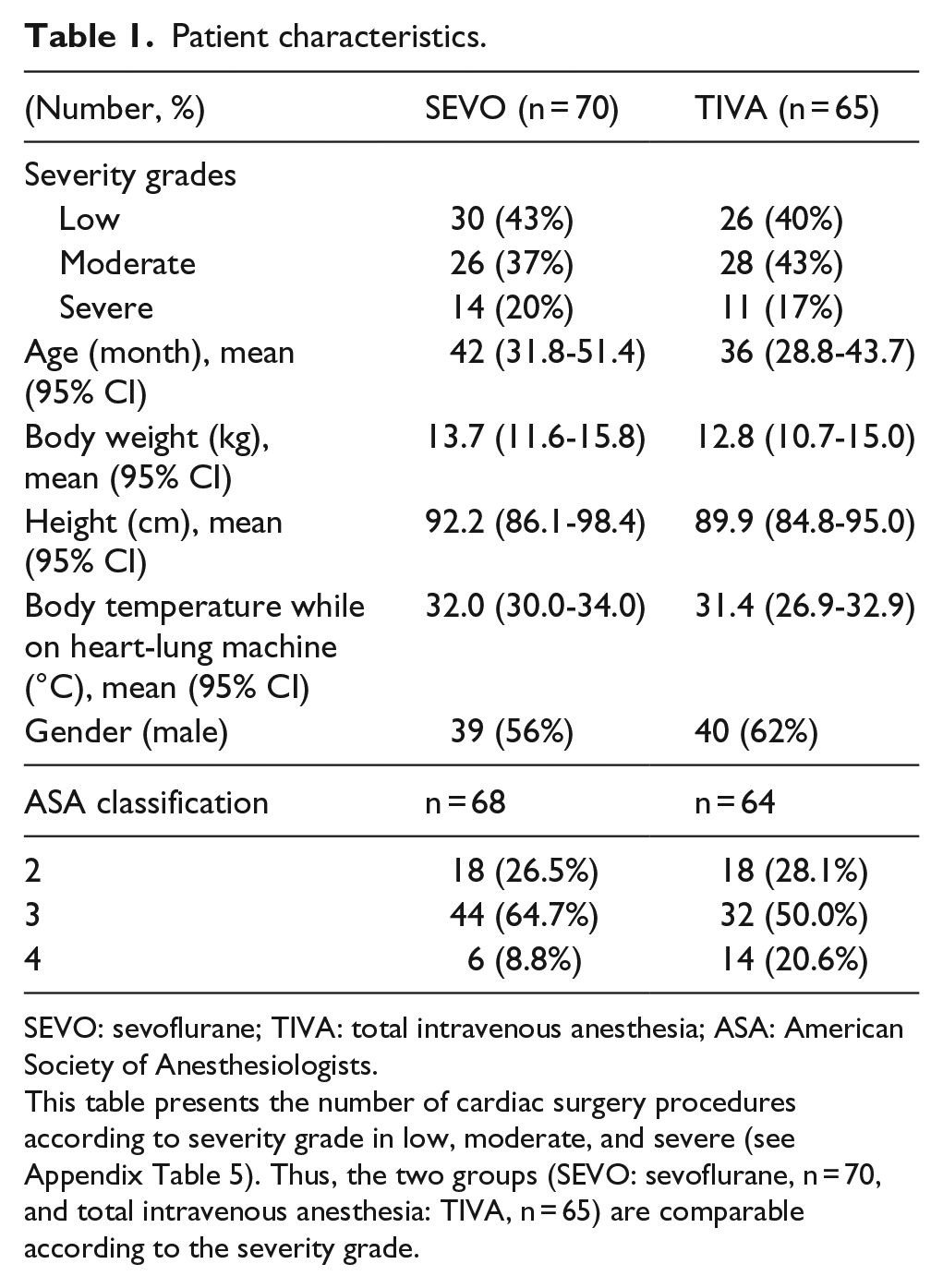
SEVO: sevoflurane; TIVA: total intravenous anesthesia; ASA: American Society of Anesthesiologists.
Study group analysis
We studied patients with age ranging from 8 weeks to 14 years. Descriptive patient characteristics (age, body weight, height, and body temperature) were very similar between the two groups (Table 1).
Further, in relation to the objectives, no significant differences were found in depth of anesthesia by analyzing phases of B1-C2-EEG-Narcotrend®-data (superficial anesthesia). Thus, the time and the number of superficial phases of anesthesia were not significantly different between the two groups (Table 2).
Narcotrend® analysis.
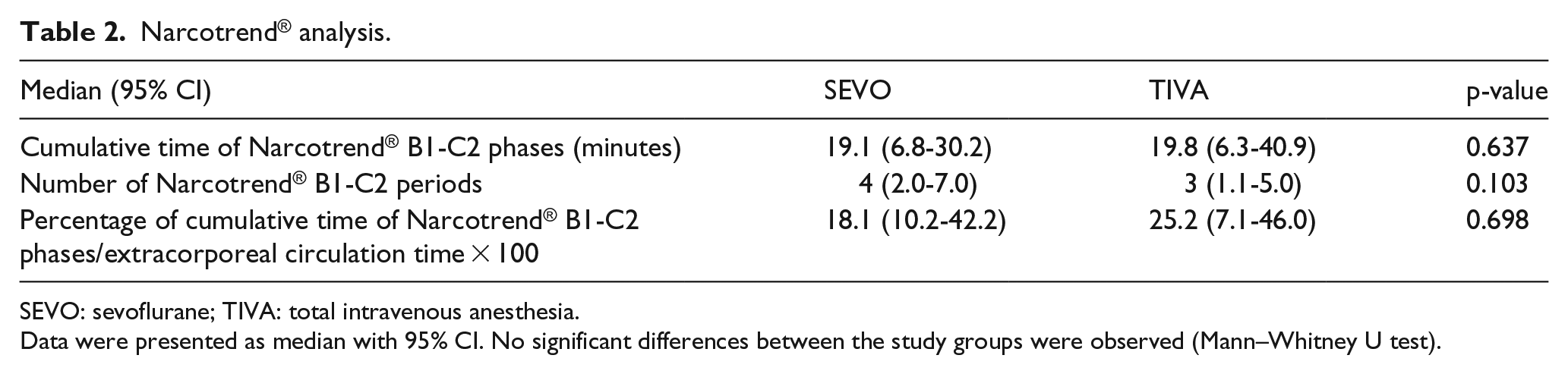
SEVO: sevoflurane; TIVA: total intravenous anesthesia.
Data were presented as median with 95% CI. No significant differences between the study groups were observed (Mann–Whitney U test).
We also compared the need for opioids and midazolam during the extracorporeal circulation period. The results showed that a higher dosage of opioids and midazolam was necessary in the TIVA group to maintain an adequate anesthesia (Table 3).
Need for opioids and midazolam during CPB.
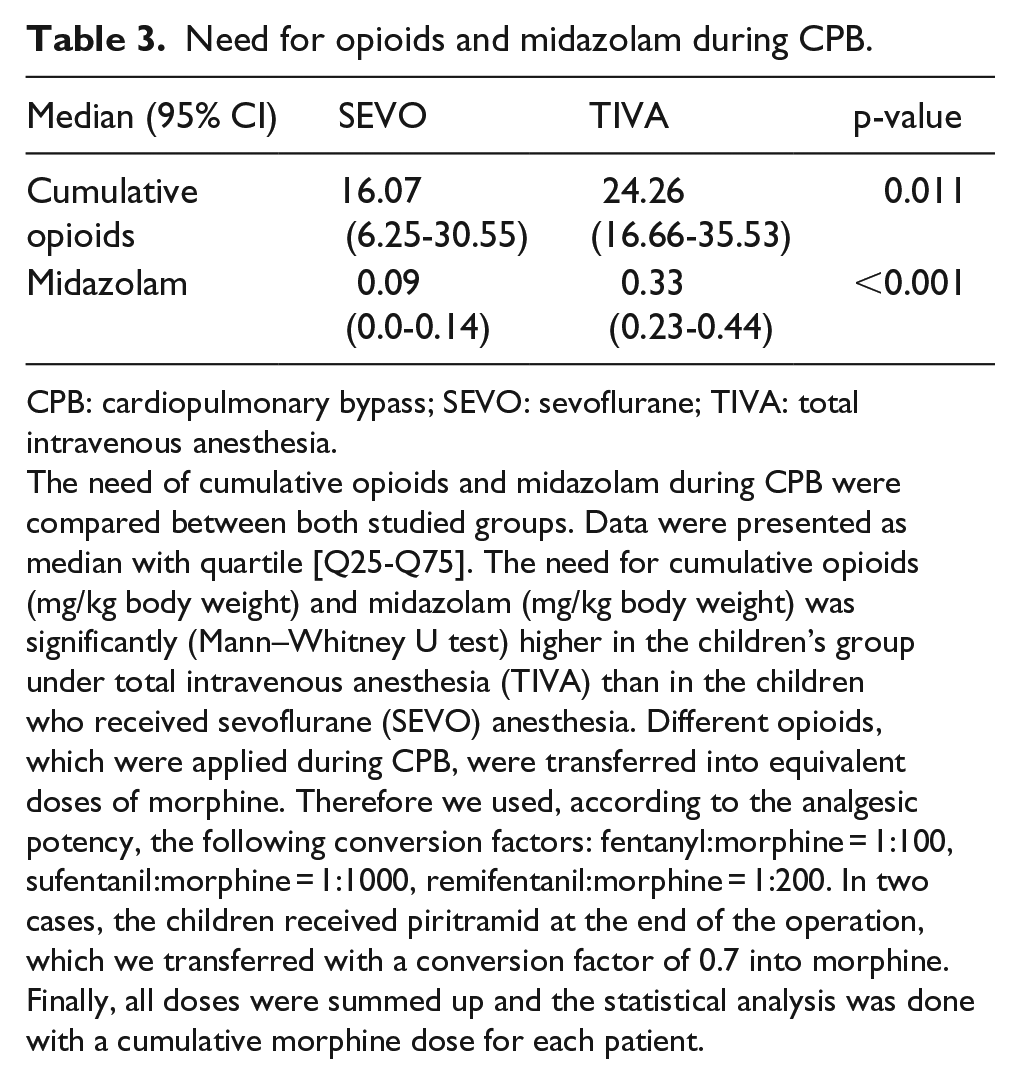
CPB: cardiopulmonary bypass; SEVO: sevoflurane; TIVA: total intravenous anesthesia.
The need of cumulative opioids and midazolam during CPB were compared between both studied groups. Data were presented as median with quartile [Q25-Q75]. The need for cumulative opioids (mg/kg body weight) and midazolam (mg/kg body weight) was significantly (Mann–Whitney U test) higher in the children’s group under total intravenous anesthesia (TIVA) than in the children who received sevoflurane (SEVO) anesthesia. Different opioids, which were applied during CPB, were transferred into equivalent doses of morphine. Therefore we used, according to the analgesic potency, the following conversion factors: fentanyl:morphine = 1:100, sufentanil:morphine = 1:1000, remifentanil:morphine = 1:200. In two cases, the children received piritramid at the end of the operation, which we transferred with a conversion factor of 0.7 into morphine. Finally, all doses were summed up and the statistical analysis was done with a cumulative morphine dose for each patient.
No marked difference between the groups was obtained in the number of postoperative days in the intensive care unit. However, the postoperative ventilation time (median (95% CI)) was significantly lower in the sevoflurane-based balanced anesthesia group (6.0 (2.0-15.0)) than in the TIVA group (13.5 (7.0-25), Figures 1 and 2).
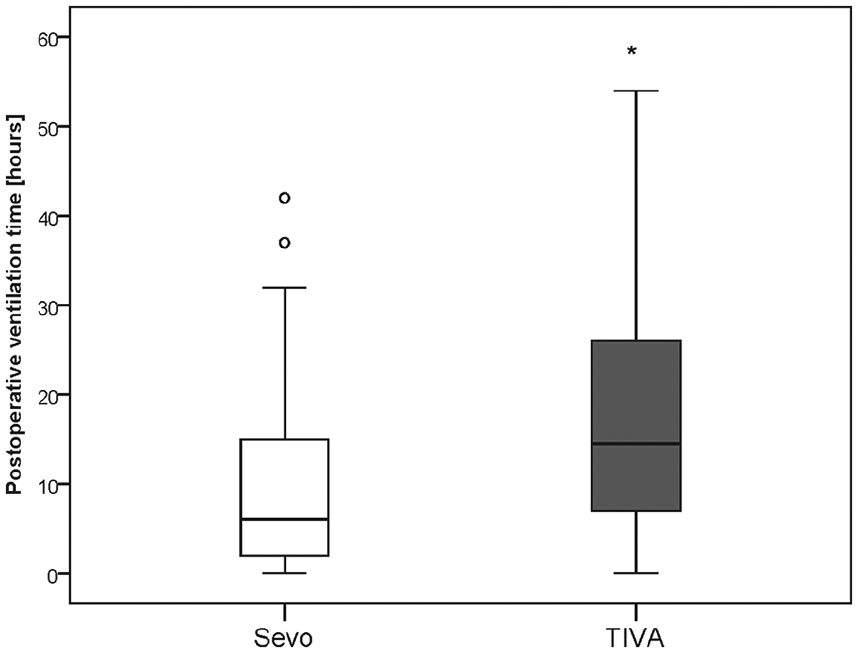
Effect of anesthetic regimen on postoperative ventilation time.
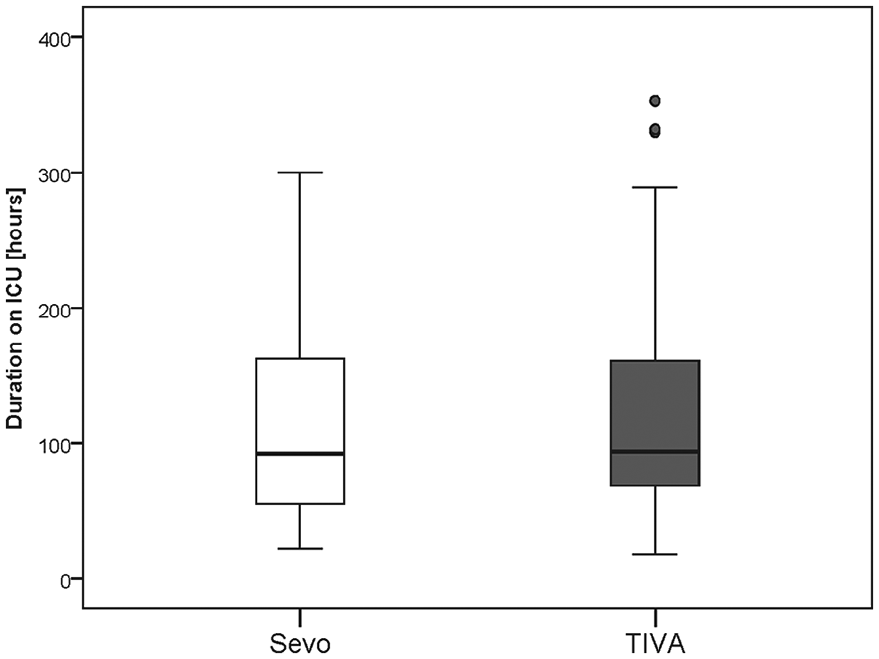
Effect of anesthetic regimen on duration of stay in the intensive care unit (ICU).
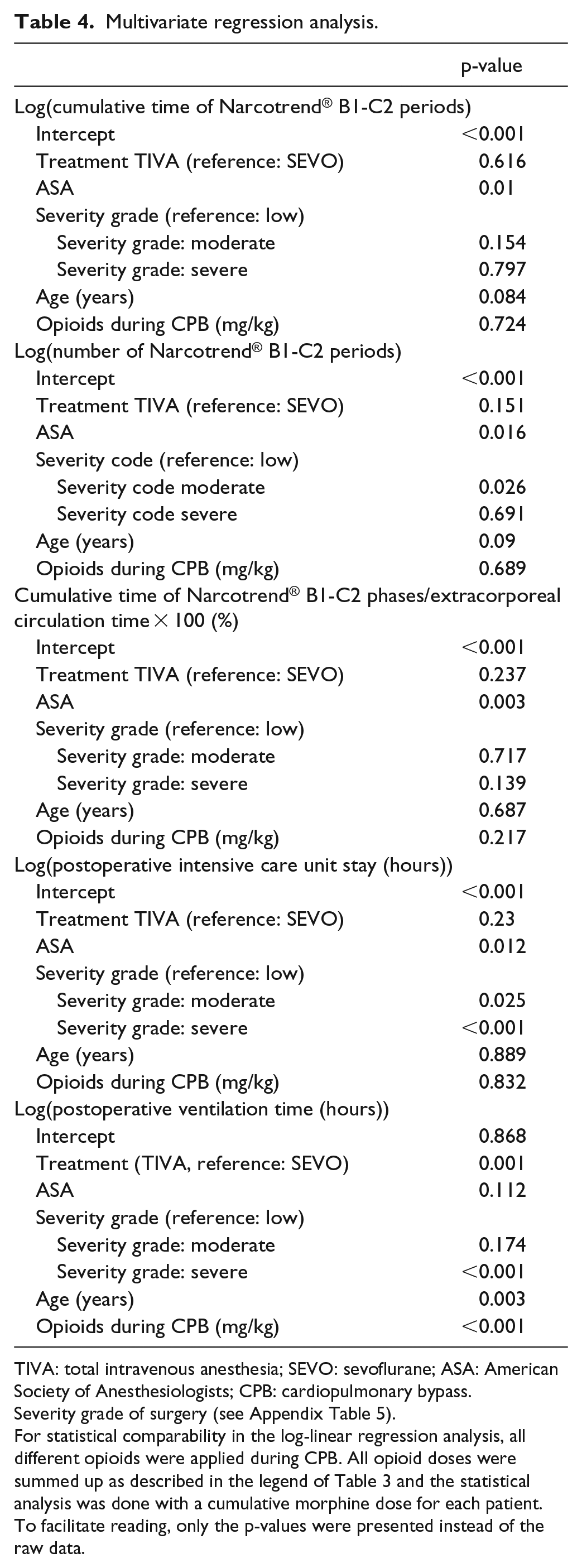
When additionally adjusting for ASA, severity grade of surgery (according to Appendix Table 5), age, and opioids during CPB in regression analyses (Table 4), a significant difference was also observed between the treatment groups regarding the time of postoperative ventilation, where longer times were observed in the TIVA group than in the sevoflurane group. In addition, regression models showed that higher ASA was associated with shorter time of Narcotrend® B1-C2 periods, lower number of Narcotrend® B1-C2 periods, and shorter cumulative time of B1-C2 phases/extracorporeal circulation. Duration of postoperative intensive care unit stay was estimated to be longer for patients with a higher ASA and a higher severity grade of surgery. A longer postoperative ventilation time was associated (additionally to TIVA treatment) with severity Grade 3 (in comparison with Grade 1), younger age, and higher opioids during extracorporeal circulation.
Multivariate regression analysis.
TIVA: total intravenous anesthesia; SEVO: sevoflurane; ASA: American Society of Anesthesiologists; CPB: cardiopulmonary bypass.
For statistical comparability in the log-linear regression analysis, all different opioids were applied during CPB. All opioid doses were summed up as described in the legend of Table 3 and the statistical analysis was done with a cumulative morphine dose for each patient. To facilitate reading, only the p-values were presented instead of the raw data.
Discussion
As a main result of this retrospective study, we showed in children undergoing cardiac surgery under extracorporeal circulation that the use of sevoflurane-balanced anesthesia during CPB showed no difference regarding phases of “superficial” anesthesia, measured by an age-related Narcotrend® algorithm compared with TIVA, but reduced the need for opioids and showed a marked advantage in the postoperative ventilation time.
Due to technical reasons we did not supply sevoflurane over the pump circuit in our institution until 2015.
In Germany, no systems are commercially available that can directly supply an inhalational anesthetic into the heart-lung machine. Therefore, the heart-lung machine had to be reconfigured by the perfusionists with separate components that are accredited and certified by the National Supervision Agency. 8 Thus, we reconfigured the heart-lung machine together with cardiotechnical specialists and thereafter received permission to use this system in 2015 in pediatric patients. Thus, from 2015 onwards we have been using in almost all cases—if there are no contraindications—extracorporeal circulation with sevoflurane-based balanced anesthesia for cardiac surgery in patients >8 weeks of age. Consequently, this study aimed to compare the TIVA regimen before 2015 with the sevoflurane-based regimen after 2015.
Balanced anesthesia can only be continued during extracorporeal circulation if the inhalational anesthetic is administered directly via the oxygenator of the heart-lung machine. The blood concentration of the inhalational anesthetic does not correlate with the concentration of volatile anesthetics on the output of the oxygenator; therefore, it is necessary to measure both the concentration of volatile anesthetics in the input of the oxygenator of the heart-lung machine as well as the depth of anesthesia to guarantee an adequate and safe anesthesia. The technical precondition for monitoring the depth of anesthesia provides the possibility to individually regulate the concentration of inhalational anesthetic and reduces the need for vasopressors.
Furthermore, the newest algorithm for electroencephalography (EEG)-based measurement of the depth of anesthesia with the Narcotrend® system has now enabled us to investigate and to measure the depth of anesthesia in even very young children of >8 weeks of age, and has been documented in pediatric patients undergoing cardiac surgery. 9
In addition, data from Schultz et al. 10 showed that the Narcotrend® index had the highest average correlation with the propofol effect-site concentration and the smallest variability in individual correlation values. Moreover, the Narcotrend® index was the only parameter which showed a monophasic trend over the entire period of investigation. Therefore, the Narcotrend® monitor can make a significant contribution in improving the quality of anesthesia by adjusting the dosage of hypnotics to individual patient needs, also in children.11–15 Although a critical assessment of EEG-based systems including the Narcotrend® system still exists, 16 we used the Narcotrend® system for testing the hypotheses of this study.
Although we observed a tendency for reduction in the percentage of time of superficial phases of anesthesia in relation to the whole time of the extracorporeal circulation (about 28%, Table 2) in the sevoflurane group, the appearance (number) and duration of Narcotrend® B1-C2 periods of superficial anesthesia were not significantly different between the sevoflurane-based balanced anesthesia and TIVA groups.
Laussen et al. 2 demonstrated in their study, using isoflurane in children undergoing cardiac surgery, a significant increase in the bispectral index (BIS™) during the rewarming phase after extracorporeal circulation. Under the presumption that Narcotrend® and BIS™ monitors are principle comparable systems, 17 it is still not clear whether this increase in EEG activity is related to temperature-dependent changes in solubility of the anesthetics in blood or rather to an increased demand for anesthetic concentration during rewarming of the brain. Dennhardt et al. used the processed EEG of the Narcotrend® monitor in children undergoing hypothermic CPB and found a decrease of the Narcotrend® index, when cooling the patient, and an increase, when rewarming the patient. In addition to the partial pressure, these authors also found, that this was related primarily to the interaction of minimal alveolar concentration and temperature. 11 On one hand, partial pressure is known to be relevant to depth of anesthesia. Otherwise, the group of Nitzschke et al. 18 showed a reduction in sevoflurane levels in the blood plasma with increasing temperature in adult patients undergoing cardiac surgery using a bypass system. Thus, two factors probably underlie the transient, more superficial anesthesia during the rewarming period after extracorporeal circulation: an increasing cerebral demand for anesthetics together with a temperature-associated reduction in plasma concentrations of sevoflurane. This might explain the existence of some superficial anesthetic periods (B1-C2) in the sevoflurane group presented here.
The anesthetic regimen was not standardized in this study. Not surprisingly, we demonstrated a significant difference in the cumulative dosage of midazolam and opioids to reach comparable anesthetic levels in the two groups. Thus, in the TIVA group we showed a higher cumulative dosage of midazolam and opioids which was associated with a prolonged time in postoperative ventilation in this group compared with the sevoflurane group.
The duration of postoperative ventilation after cardiac surgery is closely related to an early extubation process. Therefore, Harris et al. 19 investigated whether early extubation after cardiac surgery might possibly have a positive effect. In this retrospective study on 613 pediatric patients including 97 neonates, the authors demonstrated that an early extubation (<24 hours after cardiac surgery) showed a positive effect on mortality. However, owing to their study design, it cannot be excluded that this effect depends on several factors, such as preoperative ventilation, patient age, duration and severity of the surgery, neurotoxicity of medication, 19 and so on. Other studies discussing this question, for example, using a randomized prospective design, are not available so far. Thus, one limitation of the study design used in this study is that the respective data were extracted retrospectively.
In this study, we showed a very low mortality. Therefore, no statistical evaluation regarding early extubation and mortality was performed and we cannot help resolve this still open question.
It was shown that sevoflurane can reduce myocardial tissue damage via the mechanism of ischemic preconditioning,20–22 leading to reduced perioperative mortality 23 in an experimental design. Thus, it could be speculated that a sevoflurane-based balanced anesthesia compared with TIVA might be a protective effect on the myocardium. In a pediatric population, however, this protective effect was only confirmed in part of the cardiac study group,24–26 and we did not observe any marked difference in the perioperative mortality between the sevoflurane and TIVA groups either.
TIVA with propofol and opioids might represent an alternative technique for achieving an adequate anesthesia with early extubation like the one achieved with balanced anesthesia with sevoflurane. However, many concerns exist over the incidence of propofol infusion syndrome (PRIS) associated with administering propofol in infants and children over a longer period. However, there are also numerous reports of PRIS and aberrant forms of PRIS with shorter administration periods in children and adults, also in pediatric cardiac surgery.27,28 Therefore, in our opinion, sevoflurane-based anesthesia is a more suitable method to anesthetize patients in pediatric cardiac surgery as compared with TIVA including propofol anesthesia. In the future, however, alternative anesthesia for CPB might be a TIVA with opioids and dexmedetomidine.
Summary
Our findings did not show a significant difference in the occurrence of periods of superficial anesthesia in children undergoing cardiac surgery on the heart-lung machine in sevoflurane-based balanced anesthesia as compared with TIVA. Not surprisingly, a higher dosage of opioids and midazolam was necessary in the TIVA group to maintain an adequate anesthesia. Thus, the postoperative ventilation time was significantly prolonged in the TIVA group. Because our two groups were not studied contemporaneously, we cannot totally exclude the possibility that the institutional norm for postoperative ventilation would have decreased over this time period independent of anesthetic agent, following an international trend to earlier extubation.
Taken together, we show here that sevoflurane-based anesthesia during CPB is associated with an advantage in postoperative ventilation time and a reduction in opioid use as compared with TIVA in the pediatric population undergoing cardiac surgery.
Footnotes
Appendix 1
Severity grading for surgical procedures.
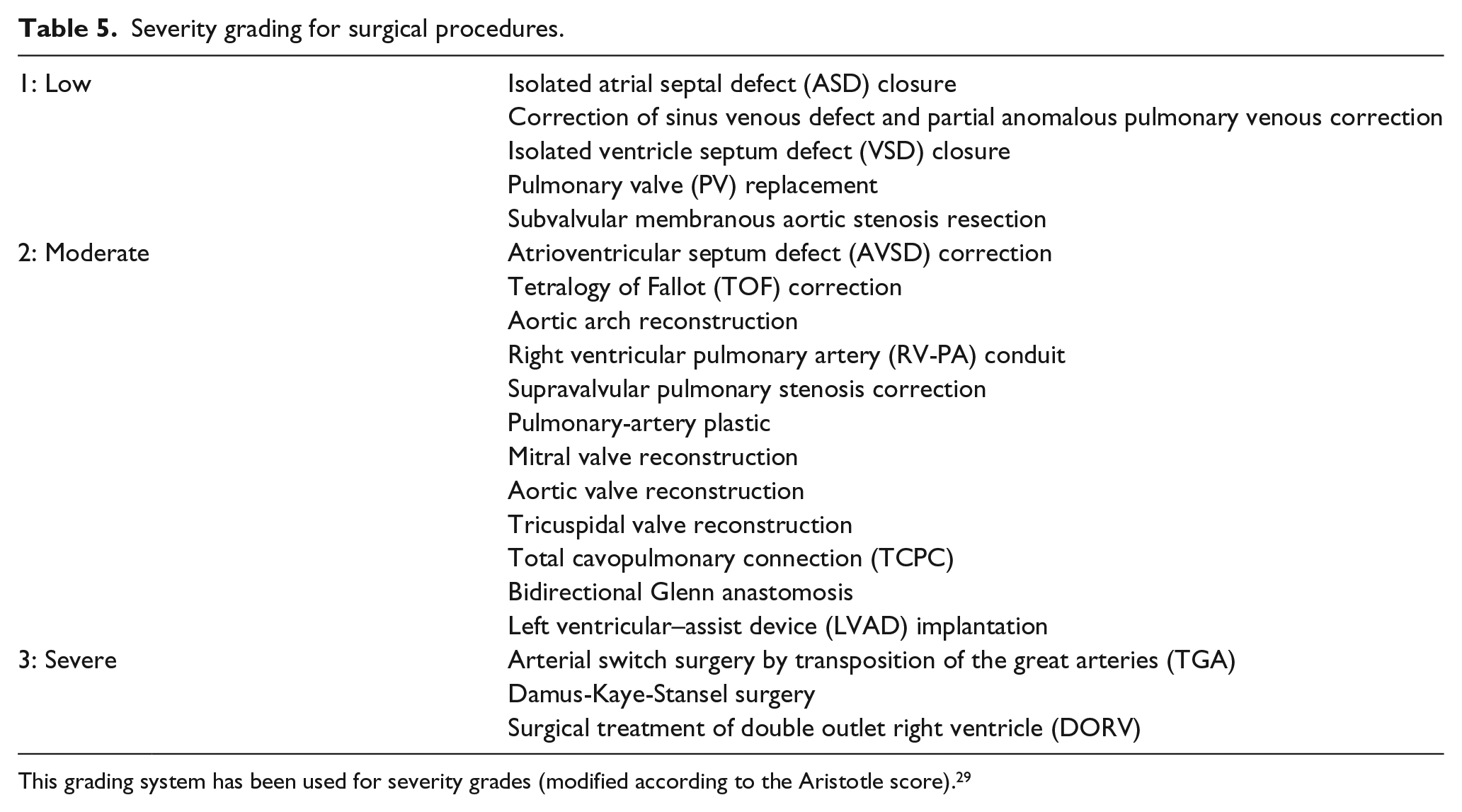
| 1: Low | Isolated atrial septal defect (ASD) closure |
| Correction of sinus venous defect and partial anomalous pulmonary venous correction | |
| Isolated ventricle septum defect (VSD) closure | |
| Pulmonary valve (PV) replacement | |
| Subvalvular membranous aortic stenosis resection | |
| 2: Moderate | Atrioventricular septum defect (AVSD) correction |
| Tetralogy of Fallot (TOF) correction | |
| Aortic arch reconstruction | |
| Right ventricular pulmonary artery (RV-PA) conduit | |
| Supravalvular pulmonary stenosis correction | |
| Pulmonary-artery plastic | |
| Mitral valve reconstruction | |
| Aortic valve reconstruction | |
| Tricuspidal valve reconstruction | |
| Total cavopulmonary connection (TCPC) | |
| Bidirectional Glenn anastomosis | |
| Left ventricular–assist device (LVAD) implantation | |
| 3: Severe | Arterial switch surgery by transposition of the great arteries (TGA) |
| Damus-Kaye-Stansel surgery | |
| Surgical treatment of double outlet right ventricle (DORV) |
This grading system has been used for severity grades (modified according to the Aristotle score). 29
Declaration of Conflicting Interests
M.G. received lecture fees from Actelion, Bayer, and MSD. Furthermore, he is a member of Advisory Board of Actelion, Bayer, and Abbott. All other authors have nothing to declare.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Departmental resources.
Ethics
This trial was approved by the Ethics Committee of the Medical Faculty of the University of Heidelberg, Germany (IRB number S-498/2015, date 25/09/2015) and performed in accordance with the ethical standards outlined in the current version of the Declaration of Helsinki.
Author contributions
B.K., T.L, M.G., H.R., and M.A.W. designed the study and together with K.P. and A.W. planned the concept of the study. B.K., T.L, M.G., K.P., H.R., and M.A.W. were responsible for conception and design. A.W. collected the data. L.B. and K.P. analyzed the data. All authors participated in interpreting the data. K.P. drafted the manuscript together with H.R, A.W., and L.B. All authors revised the manuscript.