
Abstract
Background:
Cerebral complications in veno-arterial extracorporeal membrane oxygenation are known to have a strong impact on mortality and morbidity. Aim of this study is to investigate the early incidence, risk factors and in-hospital mortality of intra-cranial ischaemia and haemorrhage in adults undergoing veno-arterial extracorporeal membrane oxygenation treatment.
Methods:
This study is a single-centre retrospective analysis on adult patients undergoing veno-arterial extracorporeal membrane oxygenation for different indications. The inclusion criterion included patients with early routine cerebral computed tomography imaging during extracorporeal membrane oxygenation, with no clinical evidence of cerebral pathology prior to cannulation. Cerebral complications were grouped by aetiology and the territories of the brain’s supplying arteries.
Results:
One hundred eighty-seven adult patients with a total of 190 veno-arterial extracorporeal membrane oxygenation treatments were included. A total of 16.3% (n = 31) had evidence of either cerebral ischaemia (11.1%) or haemorrhage (5.8%); one patient suffered from both. Cerebral computed tomography scans were performed early in median on the first day after extracorporeal membrane oxygenation cannulation; in-hospital mortality of intra-cranial ischaemia and haemorrhage was 71.4% and 45.5%, respectively. Associated with an increased risk for ischaemic lesions were cannulation of the ascending aorta, higher age, presence of an autoimmune disease and cardiac surgery prior to veno-arterial extracorporeal membrane oxygenation. An association with haemorrhagic lesions was found for a lower blood PaCO2 at 2 hours, lower blood flow through the extracorporeal membrane oxygenation device at 2 hours, higher international normalized ratio and constantly higher activated partial thromboplastin time values as well as higher mean arterial pressures until haemorrhagic lesions were evident.
Conclusion:
Cerebral complications are frequent in patients on veno-arterial extracorporeal membrane oxygenation and may be clinically silent events. Careful monitoring with routine neuroimaging seems to be the most appropriate diagnostic approach at present. Intra-cranial ischaemia occurs more frequent than haemorrhage and is associated with cannulation of the aorta ascendens.
Keywords
Background
Veno-arterial extracorporeal membrane oxygenation (V-A ECMO) is used to support patients with cardiac failure outside the operating room for limited periods of time. Common indications include refractory cardiogenic shock due to acute coronary syndrome (ACS), myocarditis, low cardiac output syndrome (LCOS), extracorporeal cardiopulmonary resuscitation (ECPR), septic shock and organ failure after heart or lung transplantation 1 . In Germany, the utilization of V-A ECMO has increased 35-fold from 2007 to 2014 2 , which may be attributed to an improved risk–benefit ratio associated with technological improvements in ECMO devices 3 . In general intra-cranial bleeding and thromboembolic events remain common,4,5 with severe implications for both survival,6,7 long-term cognitive functions and quality of life.8,9 According to the Extracorporeal Life Support Organization (ELSO; Ann Arbor, MI, USA) Registry, ischaemic and haemorrhagic stroke occurred in 2.2-6.3% and 1.2-2.5% of patients, respectively.10,11 When analysing autopsy results, higher rates are seen, with ischaemic or haemorrhagic brain lesions found as the predominant pathology in 9 of 10 patients, 12 indicating a significant underreporting. In addition, with recent improvements in ECMO technology, patient management, anticoagulation and cannulas, 13 there is a need for updated epidemiological data.2,14
The aim of this study was to investigate the early incidence of brain lesions in adult patients treated with V-A ECMO, and to characterize these by type (ischaemic vs. haemorrhagic) and location in the brain. Furthermore, potential risk factors for brain lesions were analysed.
Methods
Patients
For this retrospective analysis, the ECMO database of the University Hospital Regensburg (UKR), which is recorded in a prospective fashion, was used. The database records important clinical information on all ECMO patients (patient-related data, ECMO characteristics, ventilation settings, medication, haemodynamic data, laboratory values and complications).
All V-A ECMO treatments between March 2011 and August 2016 were checked against the following inclusion criteria: 1. patient age ⩾18 years, 2. availability of at least one cerebral computed tomography (cCT) scan obtained during ECMO support and 3. no evidence of cerebral bleeding prior to arrival at UKR. All calculations in this article relate to the total number of treatments (n = 190).
ECMO management and early cerebral CT performances at our institution
The standard of care at UKR is to provide a bolus dose of 2,000-5,000 IU unfractionated heparin (UFH) during peripheral ECMO cannulation, except in ECPR cases post-cardiotomy and when active bleeding is suspected. No heparin is used in the priming solution of the ECMO circuit. After cannulation, a continuous intravenous infusion of UFH is used for systemic anticoagulation, aiming for a 1.5- to 2-fold increase (respectively, 50-80 seconds) of the activated partial thromboplastin time (aPTT). The aPTT and dose of UFH are monitored once daily, more often only if adjustment is necessary. When bleeding occurs, UFH is stopped and restarted once the bleeding is controlled. All patients undergo arterial blood gas (ABG) analysis before ECMO cannulation (pre-ECMO values) and 2 hours after. During ECMO support, ABG, haematological, biochemical and coagulative blood markers are recorded each morning. In our institution, a first CT scan is performed deliberately soon after ECMO cannulation (on the first or second day). This CT scan includes cerebral (cCT), chest, abdominal and thigh imaging to verify correct positions of the cannulas, to screen for a focus of infection, unrecognized haemorrhage or malignancies, and to identify early signs of cerebral ischaemia/haemorrhage that may not yet be clinically evident. The early CT scan (within 48 hours) is deferred only when patients are too unstable for transportation or if the reason for V-A ECMO is clear and the patient improves rapidly. Further cCT scans are only performed when patients exhibit new neurologic abnormalities or if patients have persistent neurological disabilities after CPR.
Analysis of cerebral CT images
Formal radiologist’s reports of cCT images were screened to identify evidence of cerebral pathology, namely, hypoxic brain injury, ischaemia, intraparenchymal haemorrhage (IPH), subarachnoid haemorrhage (SAH), subdural haemorrhage (SDH) or epidural haemorrhage (EDH). Where present, the largest extent (length and width) of these lesions was recorded and they were allocated to the corresponding arterial territory: anterior cerebral artery (ACA), middle cerebral artery (MCA), posterior cerebral artery (PCA) or brainstem/cerebellar territory. Controversial reports were reviewed and reevaluated in collaboration with a radiologist. Only the primary manifestation of a cerebral complication was categorized, while a secondary haemorrhagic transformation was classified as primary ischaemic.
If there was evidence of hypoxic brain injury, patients were classified in two groups: moderate hypoxic injury (basal ganglia definable, with reduced corticomedullary differentiation) and generalized severe hypoxic injury (basal ganglia undefinable, no corticomedullary differentiation, generalized cerebral oedema or early brainstem incarceration).
Where available, follow-up data were obtained for patients after discharge and categorized into three of the five groups of the Glasgow Outcome Scale (GOS): 15 good recovery (GOS 5), moderate disability (GOS 4) and severe disability (GOS 3).
Statistical analysis
Descriptive statistics are presented with the number and percentage for categorical variables and with median (25th-75th percentile interquartile range (IQR)) for continuous variables, as the broad majority was, according to the Kolmogorov–Smirnov test, not normally distributed. Between-group comparisons of categorical and metric variables were performed using Fisher’s exact test or Mann–Whitney U test. All odds ratios (ORs) and 95% confidence intervals (CIs) were calculated by binary logistic regression to identify risk factors for cerebral ischaemia and haemorrhage.
A p value of <0.05 was considered statistically significant. The analyses were performed using IBM SPSS Statistic software version 24.0 (SPSS Inc. Chicago, IL, USA).
Results
Patients
Among 320 patients who underwent V-A ECMO during the study period (324 ECMO treatments), 134 treatments did not meet the inclusion criteria because 1. patient age <18 years (6 treatments), 2. no cCT scan obtained during ECMO support (125 treatments) and 3. cerebral bleeding diagnosed prior to arrival at UKR (3 treatments). By absolute numbers, this led to the inclusion of 187 patients (190 V-A ECMO treatments; Figure 1).
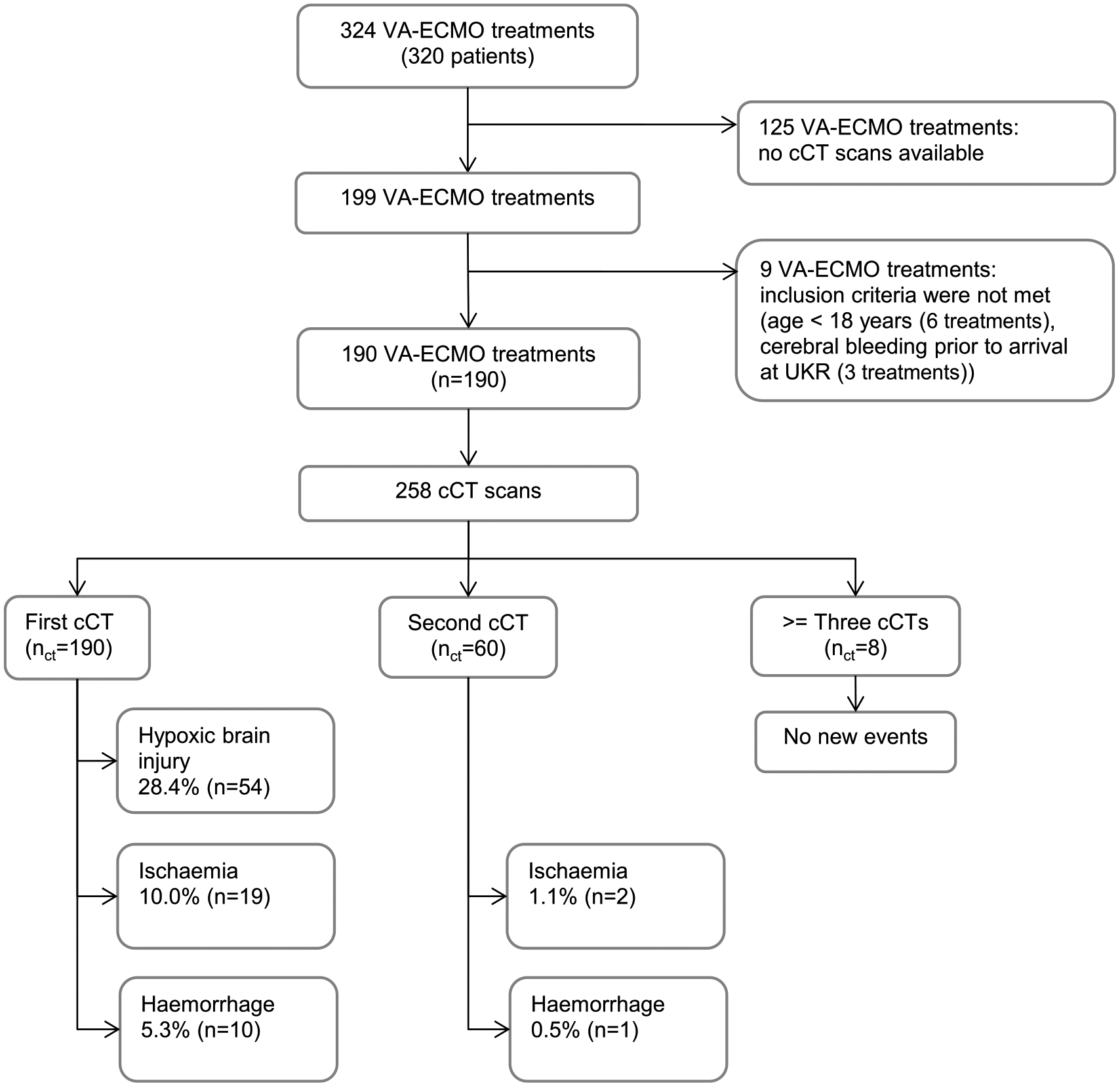
Flow chart of the study.
Patient’s median age in all included ECMO treatments was 58.5 (IQR: 49-65) years, 67.4% (n = 128) were male. The most common reason for initiation of V-A ECMO was ECPR (54.7%), followed by LCOS (36.8%) and failure to wean from cardiopulmonary bypass (8.4%). In total, 80.0% (n = 152) had suffered a cardiac arrest prior to initiation of ECMO. The group of ECPR cases included 19 out-of-hospital cannulations. Univariate comparisons of baseline characteristics of patients and their co-morbidities are presented in Table 1. Intake of antiplatelet medication was only documented in two patients.
Patient demographics, patient factors and ECMO factors in patients with ischaemic lesions or haemorrhagic lesions.
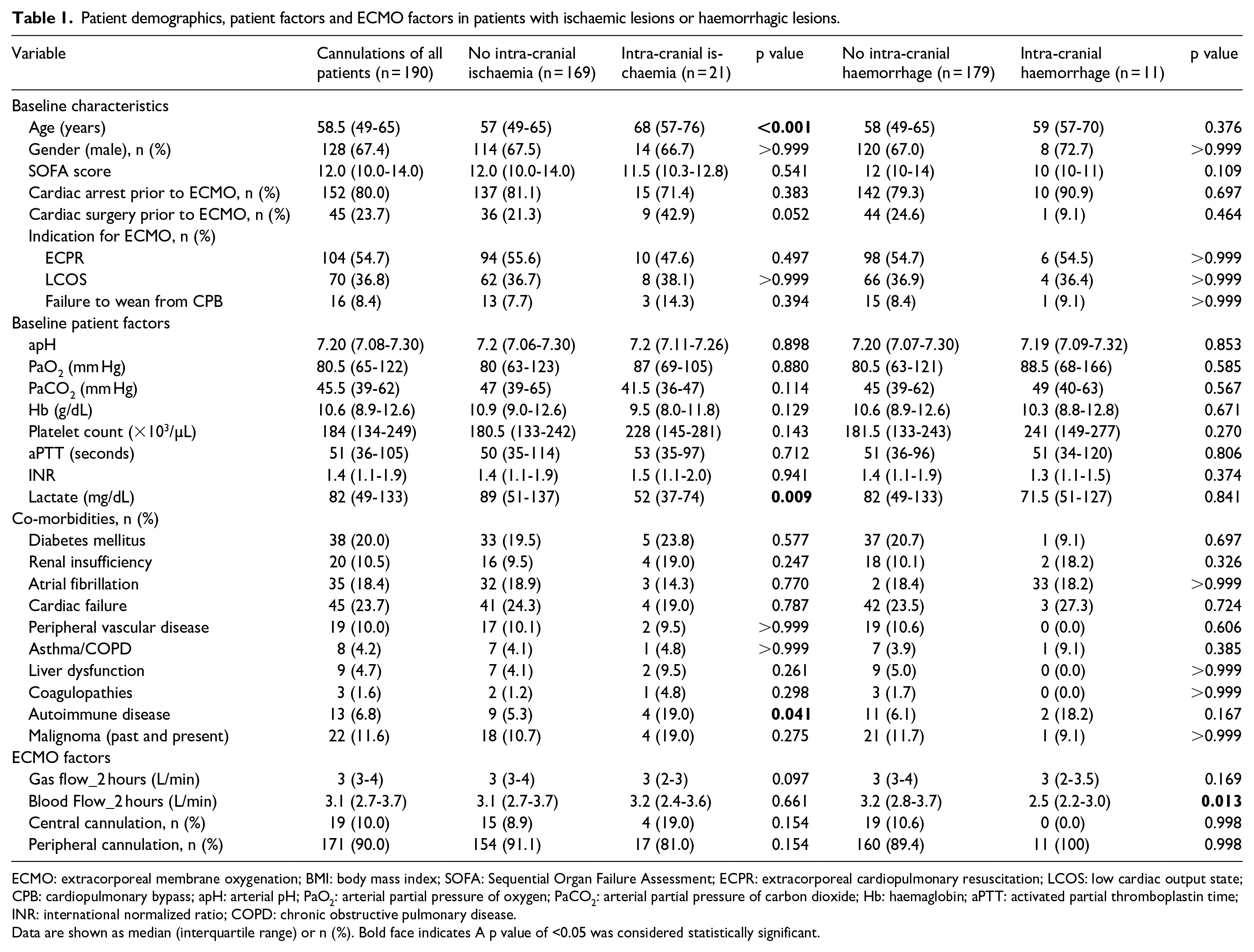
ECMO: extracorporeal membrane oxygenation; BMI: body mass index; SOFA: Sequential Organ Failure Assessment; ECPR: extracorporeal cardiopulmonary resuscitation; LCOS: low cardiac output state; CPB: cardiopulmonary bypass; apH: arterial pH; PaO2: arterial partial pressure of oxygen; PaCO2: arterial partial pressure of carbon dioxide; Hb: haemaglobin; aPTT: activated partial thromboplastin time; INR: international normalized ratio; COPD: chronic obstructive pulmonary disease.
Data are shown as median (interquartile range) or n (%). Bold face indicates A p value of <0.05 was considered statistically significant.
The in-hospital mortality was 65.2% (n = 122). After hospital discharge, follow-up data were available for 39 (59.1%) of 66 survivors. 20.5% (n = 8) had a good recovery (GOS 5), while 59.0% (n = 23) had moderate disabilities (GOS 4), and 20.5% (n = 8) had severe disabilities (GOS 3).
ECMO characteristics
Most cannulations were performed peripherally via the femoral artery (90.0%), while the remainder were cannulated centrally (ascending aorta (6.8%), subclavian artery (3.2%)). The median length of ECMO support was 4 (IQR: 2-8) days. Univariate comparisons of ECMO factors are presented in Table 1. An overview of ECMO pumps and oxygenators is given in the Supplemental Material (S1).
Analysis of cerebral CT images
Overall, 258 cCT scans were evaluated; all patients included in the analysis had at least one early, within 48 hours of cannulation, cCT for each individual ECMO treatment (n = 190), which was performed in median during Day 1 (IQR: 0-2). In 46.8% (n = 89) of cases, this first cCT scan was obtained on the day of cannulation. Those who had a second cCT scan (n = 60) underwent imaging in median on Day 3 (IQR: 2.0-6.8). For ECMO treatments in which a third (n = 6) or fourth cCT (n = 2) scan was obtained, no new cerebral lesions were identified.
Of all included patients, 16.3% (n = 31) had evidence of cerebral lesions on cCT (first or second cCT); ischaemic lesions in 11.1% (n = 21) and haemorrhagic lesions in 5.8% (n = 11) (Figure 1). In one case, there was both an ischaemic and haemorrhagic lesion identified in the first cCT scan. The distribution of brain lesions is illustrated in Figure 2. In-hospital mortality of patients with cerebral ischaemia and haemorrhage was 71.4% and 45.5%, respectively. This was not significantly different from patients without lesions (p = 0.630 for ischaemia and p = 0.205 for haemorrhage).
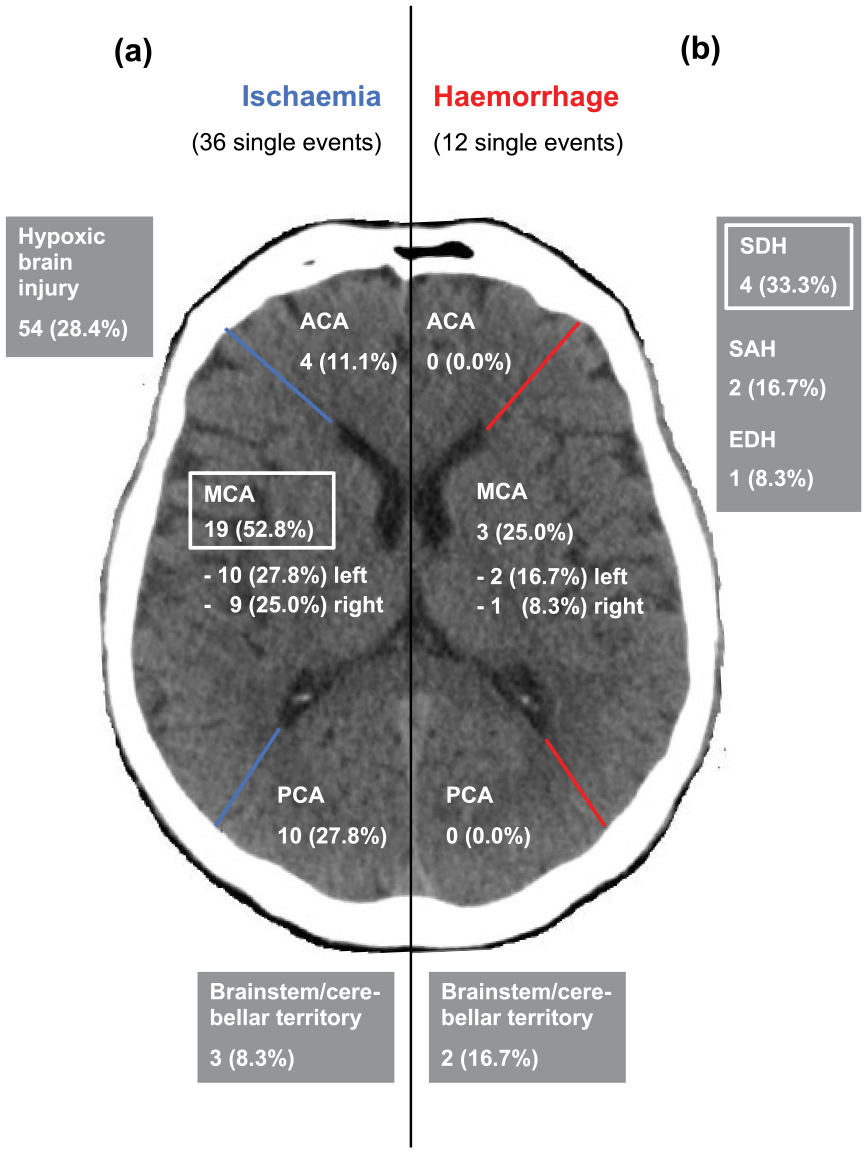
Distribution of (a) ischaemic and (b) haemorrhagic events in the cerebral vascular territories, the brain stem and cerebellum. Events are given in absolute numbers and percentage (%).
During V-A ECMO, hypoxic brain injury, already visible in the first cCT scan, was present in 28.4% (n = 54). In these patients, in-hospital mortality was 96%. 20.4% (n = 11) of hypoxic brain injuries were graded as moderate and 79.6% (n = 43) as generalized. Prior to ECMO, 81.8% of cases with moderate hypoxic brain injury, and 97.7% of the cases with generalized hypoxic injury, suffered cardiac arrest.
The median size of ischaemic lesions was 2.0 (IQR: 1.0-3.6) cm in length and 1.1 (IQR: 0.6-2.9) cm in width. IPH had a median length of 2.1 (IQR: 0.9-5.0) cm and a width of 0.8 (IQR: 0.8-3.0) cm. Multifocal ischaemic events were recorded in 3.2% (n = 6). There were no multifocal haemorrhagic events.
Variables associated with cerebral complications during V-A ECMO
Ischaemic lesions
Of all patients, 11.1% (n = 21) had an ischaemic lesion diagnosed on a cCT scan. Multiple variables from baseline and during V-A ECMO treatment were analysed for univariate risk association of ischaemic lesions; the results are presented in Tables 1 and 2. Variables associated with a risk of ischaemic lesions were the following: higher age, presence of an autoimmune disease, cardiac surgery prior to V-A ECMO and a higher increase in sweep gas flow within the first 24 hours of treatment (Table 2).
Risk factors for intra-cranial ischaemia during V-A ECMO.
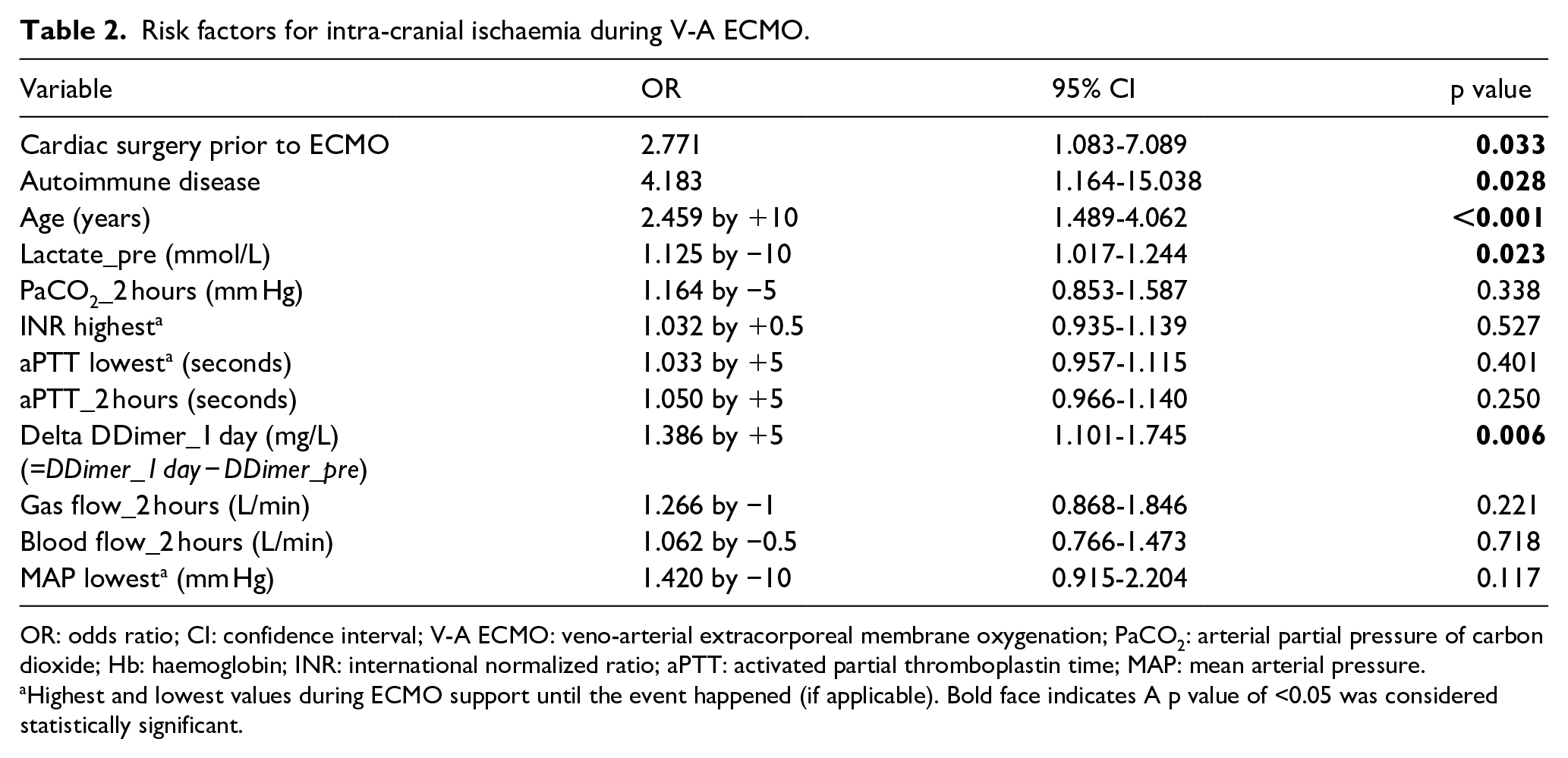
OR: odds ratio; CI: confidence interval; V-A ECMO: veno-arterial extracorporeal membrane oxygenation; PaCO2: arterial partial pressure of carbon dioxide; Hb: haemoglobin; INR: international normalized ratio; aPTT: activated partial thromboplastin time; MAP: mean arterial pressure.
Highest and lowest values during ECMO support until the event happened (if applicable).
Bold face indicates A p value of <0.05 was considered statistically significant.
Regarding the site of cannulation, the risk of intra-cranial ischaemia was significantly higher when the ascending aorta (n = 13) was used for return (OR = 4.0 (1.1-14.3), p = 0.033). Subclavian artery cannulation (n = 6) was not associated with ischaemic complications (p = 0.999). Overall, cannulation of the femoral artery (n = 171) has shown to be protective, although not significant, as the occurrence of cerebral ischaemia was higher, when the cannula was not in the femoral artery (OR = 2.4 (0.7-8.1), p = 0.154). Atrial fibrillation, hypocapnia, lower aPTT, INR values or lower heparin doses at any time during ECMO support were not associated with the incidence of cerebral ischaemia.
Haemorrhagic lesions
Haemorrhagic lesions occurred in 5.8% (n = 11) of patients. The variables analysed for univariate risk association are shown in Tables 1 and 3. An association was found for a lower PaCO2 at 2 hours (31 vs. 35 mm Hg), lower blood flow through the ECMO device at 2 hours, higher INR values and constantly higher aPTT values as well as higher mean arterial pressures (MAP) until haemorrhagic lesions were identified. Higher heparin dosages at any time during ECMO support were not associated with cerebral haemorrhage.
Risk factors for intra-cranial haemorrhage during V-A ECMO.
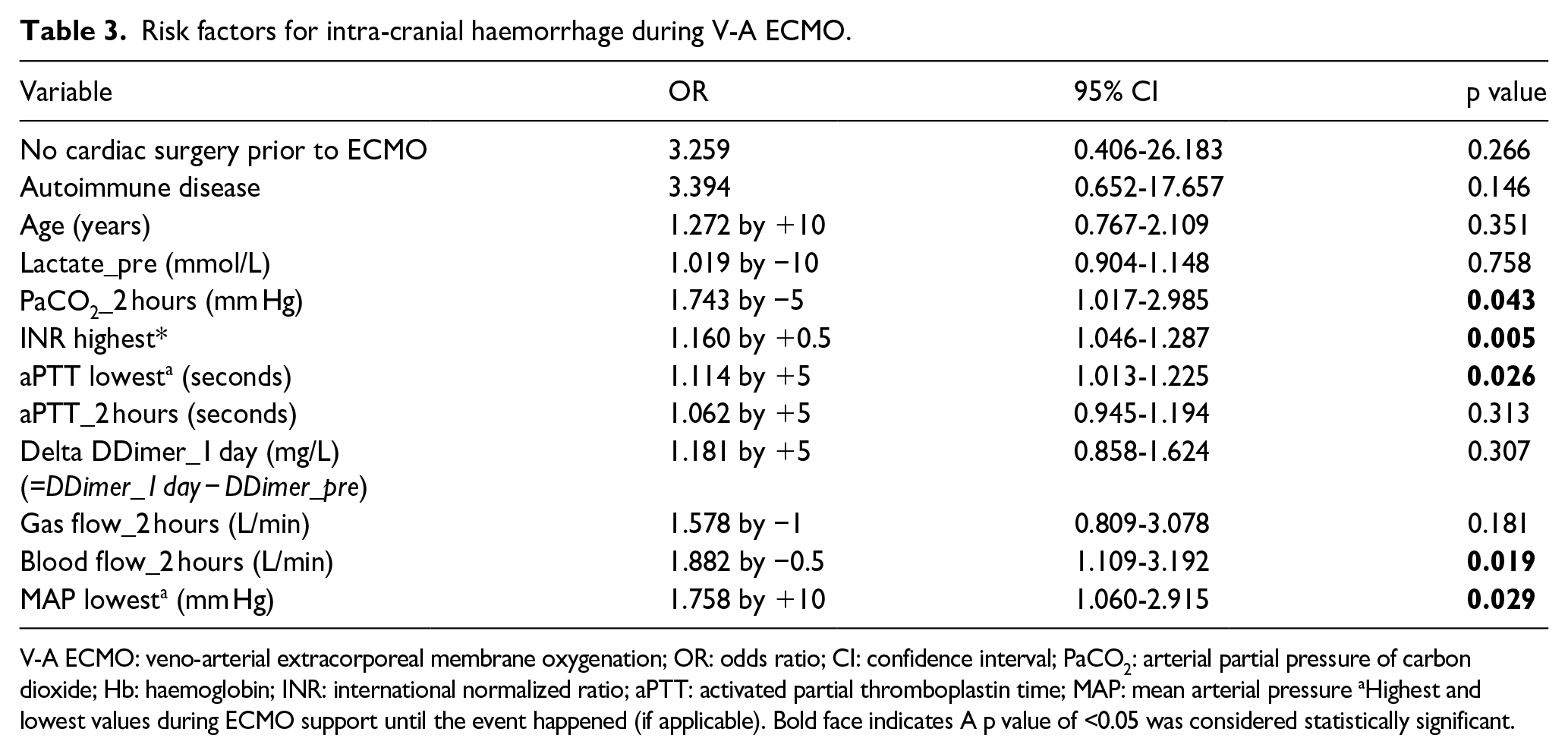
V-A ECMO: veno-arterial extracorporeal membrane oxygenation; OR: odds ratio; CI: confidence interval; PaCO2: arterial partial pressure of carbon dioxide; Hb: haemoglobin; INR: international normalized ratio; aPTT: activated partial thromboplastin time; MAP: mean arterial pressure aHighest and lowest values during ECMO support until the event happened (if applicable).
Bold face indicates A p value of <0.05 was considered statistically significant.
Discussion
With thrombotic and haemorrhagic events still being the major complications of modern ECMO therapy, their occurrence within the central nervous system is one of the most feared ECMO complications. 16 We performed this analysis to add information on the appearance of cerebral complications in V-A ECMO patients and to gain further insight into associated risk factors. To our knowledge, this is the largest study to date in this area with 187 adult patients (n = 190 V-A ECMO treatments) with early CT scans of the brain after initiation of V-A ECMO.
Our most relevant points are the early appearances of brain lesions in V-A ECMO patients and a high incidence of 16.3%; ischaemic lesions were associated with cannulation of the ascending aorta and haemorrhagic lesions with higher INR values and higher minimum aPTT values.
In recent literature, several studies have reported on cerebral complications in the ECMO populations.9,17,18 However, in our experience, it is important to distinguish between cardiac V-A ECMO and respiratory veno-venous extracorporeal membrane oxygenation (V-V ECMO) patients as the underlying conditions of the patients are very different and also treatment modalities are handled differently in regard to blood flows, cannulas and anticoagulation.
Incidences of ischaemic and haemorrhagic lesions in our study were 11.1% and 5.8%, respectively. In the published literature, the incidence of intra-cranial ischaemia and haemorrhage in adult V-A ECMO patients varied between 2.2% and 6.3%, and 1.2% and 6.4%, respectively.4,11,19,20 Data from the ELSO Registry reported an incidence of 7.9% for ischaemia and 1.8% for haemorrhage in a total of 4,522 adult patients supported with V-A ECMO. These data, however, underly limitations of a registry with voluntary reporting, missing data and high probability of an underestimation. Notably, there are three single-centre V-A ECMO studies exceeding the incidence of 6.4% for intra-cranial haemorrhage. In 1999, Kasirajan et al. 21 reported an incidence of 18.9%, and based on more recent data in 2016, Omar et al. 22 found 7.8%. Fletcher Sandersjöö et al. 18 reported even 27% for adult V-A ECMO patients receiving neuroimaging. The rate of haemorrhagic lesions (5.8%) in our study falls within the most common range found in the literature (1.2-6.4%) but ranks unexpectedly high considering that first cCT scans were performed in median on Day 1. It has been suggested that neurological complications associated with ECMO are poorly understood, 14 and due to a lack of routine neuroimaging in many studies, cerebral complications might have been underestimated.18,23,24 Lidegran et al. 24 also found higher incidences of ischaemic stroke (9%) and intracerebral haemorrhage (ICH; 15%), when cCT scans during ECMO were available; however, this study included V-V and V-A ECMO in paediatric and adult patients. The relatively high appearance of ischaemic events in our study is probably due to more incidental findings as discussed above and a higher number of patients with CPR.
In-hospital mortality in patients with ischaemic lesions was 71.4% and 45.5% for patients with haemorrhagic lesions. Patients with hypoxic brain injury had an in-hospital mortality of 96.3% in our study population. The mortality associated with ischaemic lesions accords with previous estimates, where it ranged from 60% to 82%. 11 The mortality associated with haemorrhagic brain lesions during ECMO has previously been estimated between 80% and 96%.11,21,22 The difference to our better survival rates may be explained by the fact that also clinically silent, minor bleeding events have been recorded with routine cCT scans. When taking all lesions independent of size into account, we could not identify an association between intra-cranial ischaemia or haemorrhage and mortality, as it has been reported previously in literature.6,7 Regarding mortality of intra-cranial lesions, our patient outcome was good, despite their early appearances, so it may be beneficial to use early cCT imaging to adjust anticoagulation in time. This may indicate that early diagnosis of brain lesions is important to adjust therapy and, thus, improve patient anticoagulation management that may influence outcome.
Regarding variables associated with an elevated risk for intra-cranial ischaemia, we found patient characteristics including higher age, pre-existing autoimmune disease and cardiac surgery prior to ECMO to be independent risk factors; those are all parameters that have also been associated with ischaemic stroke in patient populations other than ECMO.25,26 An ECMO-specific variable that has shown to be statistically significant is change to higher sweep gas flows within the first 24 hours of treatment.
While sweep gas flow and CO2 levels have been previously identified as being associated with cerebral complications,27,28 reduced ECMO blood flow was not. 29 If ECMO settings are responsible for increased cerebral complications, this still has to be shown. Variables like oxygenator surface, pre- and post-oxygenator pressure as well as coating of the system are also likely to play a crucial role.
Interestingly, lower ECMO blood flow is also associated with intra-cranial haemorrhage in our study. Other variables to indicate a higher risk were a lower PaCO2 at 2 hours (31 vs. 35 mm Hg), a higher INR value, constantly higher aPTT values and a higher MAP until haemorrhagic lesions were evident. Pathophysiologic considerations regarding lower blood flow could be that low blood flow within the ECMO system favours clot formation. Consecutively, these clots could either cause thrombotic emboli or induce haemolysis with higher bleeding risks. If these hypotheses are relevant, then need to been shown in further research.21,22 As fast reduction of PaCO2 levels was mentioned as a risk factor for neurologic complications before,27,28 our centre policy is to increase the sweep gas flow step by step; however, we do not follow a strict protocol yet.
Our data give further insight into the appearance of cerebral complications in V-A ECMO patients. The high appearance indicates the need for better monitoring in our patients. Neuroimaging gives only a snapshot, and the best timing is not known at present. However, most of the events seem to occur early in/before ECMO treatment; therefore, we would suggest to perform a cCT scan on the first day of ECMO treatment. Current state of alternative brain monitoring options has recently been reviewed by Lorusso et al. 16 If continuous electroencephalography monitoring or near infrared spectroscopy can have a positive impact on patient outcome has yet to be shown.30,31,32
Other points to start from are changes in ECMO management strategies like sweep gas flow, blood flow, cannulation sites or optimization of coagulation. A recent report by Kalbhenn et al. 33 showed a reduced incidence of intra-cranial haemorrhage in V-V ECMO with target-controlled coagulation factor substitution. Generation of prospective data would be very valuable to take steps towards better prevention strategies for cerebral complications, especially as case numbers of patients receiving V-A ECMO are still rising in Germany and other countries. Reasons for this increase are technological improvement, encouraging reports and probably also a good reimbursement situation. Therefore, it is important to carefully consider possible complications.
Our study has several limitations. A main limitation is its retrospective design. And besides being the largest study on cerebral complications in V-A ECMO patients, the sample size is still a limitation. The low number of pathologic findings does not allow a multivariate analysis. Further, not all patients in the study period underwent a cCT scan, which can be considered a selection bias. A limitation of the cCT scans is that ischaemic strokes only show up 6-8 hours after stroke symptoms appear. In almost 55% of our patients, the ECMO was used for ECPR, which implies that many cerebral pathologies might have been caused by the reanimation.
The intention to perform an early cCT scan soon after ECMO cannulation is what distinguishes the presented data from other reports, where patients who died early on ECMO were not considered to have suffered cerebral lesions 27 or neuroimaging was only performed when neurologic symptoms have been noticed.17,27 This is why our results might add incidental findings and give a better estimate of cerebral complications in V-A ECMO patients.
Conclusion
Cerebral complications are frequent in patients on V-A ECMO and may be clinically silent events both for cardiac support and ECPR. Careful monitoring with liberal indication for neuroimaging is advisable.
Intra-cranial ischaemia occurred more frequent than haemorrhage in our patients and was in the presented study associated with cannulation of the ascending aorta. This aspect should be considered when the cannulation site is chosen, although further research is needed to confirm this point. The precise roles of initial setting of PaCO2 levels and management of coagulation parameters have to be evaluated carefully, to possibly improve patient care in the future.
Supplemental Material
supplementary_material_907438 – Supplemental material for Incidence of early intra-cranial bleeding and ischaemia in adult veno-arterial extracorporeal membrane oxygenation and extracorporeal cardiopulmonary resuscitation patients: a retrospective analysis of risk factors
Supplemental material, supplementary_material_907438 for Incidence of early intra-cranial bleeding and ischaemia in adult veno-arterial extracorporeal membrane oxygenation and extracorporeal cardiopulmonary resuscitation patients: a retrospective analysis of risk factors by Maximilian Valentin Malfertheiner, Andrea Koch, Christoph Fisser, Jonathan Edward Millar, Lars Sigfried Maier, Florian Zeman, Florian Poschenrieder, Matthias Lubnow, Alois Philipp and Thomas Müller in Perfusion
Footnotes
Acknowledgements
We would like to thank the nursing staff of the intensive care units and the perfusionists of the University Medical Center Regensburg, Regensburg, Germany, for their excellent work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Consent for Publication
Consent for publication was waived by the local ethics committee as all data are retrospectively collected from routine care. And no information in the manuscript allows a connection to a single patient.
Ethical Approval and Consent to Participate
The requirement of individual patient consent and necessity of approval for the data report were waived by the local ethics committee because of the study’s design and data collection from routine care. A letter from the local ethics committee is on file.
Author Contributions
All the authors read and approved the final manuscript for submission. M.V.M. and A.K. were responsible for drafting the article and were involved in the acquisition of data, analysis and interpretation of this information. L.S.M., F.P., A.P., T.M. and M.L. were involved in the conception, hypotheses delineation and the design of the study and its revision prior to submission. C.F., J.E.M. and F.Z. were involved in the analysis and interpretation of this information, and the critical revision of the article prior to submission.
Availability of Data and Material
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.