
Abstract
Background:
Recently extracorporeal membrane oxygenation is becoming the commonly used mechanical assist device for the treatment of severe cardiogenic shock in postcardiotomy patients. Evaluation of risk factors of negative outcome would be beneficial in decision-making in the elderly patient population.
Methods:
This was a retrospective single-centre analysis of elderly patients who underwent extracorporeal membrane oxygenation treatment for refractory cardiogenic shock in a tertiary care centre. Demographic data, comorbidities and perioperative parameters were collected to evaluate their impact on the outcome of extracorporeal membrane oxygenation treatment in this patient group. Logistic regression analysis of the variables was performed to identify factors predicting an adverse outcome.
Results:
Forty consecutive elderly patients underwent extracorporeal membrane oxygenation treatment during the study period. The mean age was 76.7 ± 3.8 years, 27 (68%) were male. The mean Survival after Veno–Arterial extracorporeal membrane oxygenation score before initiating extracorporeal membrane oxygenation support was − 11 ± 6. Intra-aortic counterpulsation was used as the first-line mechanical support in 31 (77%) patients. The mean duration of extracorporeal membrane oxygenation support was 172 ± 128 hours. Twenty-four patients (56%) were successfully weaned from extracorporeal membrane oxygenation, and 8 (20%) survived to hospital discharge. Lactate level before extracorporeal membrane oxygenation initiation was the only predictor of unfavourable outcome in multivariate analysis (p < 0.05).
Conclusion:
High lactate level before initiation of extracorporeal membrane oxygenation was the most important prognostic values of an unfavourable outcome.
Keywords
Introduction
Postcardiotomy shock occurs in 2-6% of all adult patients undergoing cardiac surgery and is associated with high mortality rates. 1 For many years intra-aortic balloon counterpulsation was the most frequently used mechanical assist device for the treatment of cardiogenic shock; however, its efficacy in the treatment of cardiogenic shock has been debated. Recent IABP-SHOCK II trial failed to demonstrate the effect of intra-aortic balloon pump (IABP) on long-term follow-up.2,3 Extracorporeal membrane oxygenation (ECMO) has been successfully used as a support strategy in the treatment of cardiogenic shock refractory to conventional care. 4 The use of this technology has increased dramatically over the last decade, 5 making it perhaps the second-most utilized therapy after IABP for cardiogenic shock treatment.
Patients undergoing cardiac surgery tend to be elderly, representing over 50% of all cardiac surgical patient population. 6 According to the guidelines of the Extracorporeal Life Support Organization, advanced age is a relative contraindication for the use of ECMO in the treatment of a life-threatening cardiac or respiratory failure. 7 Some local hospital guidelines do not recommend the use of any type of ECMO in patients older than 70 years. 8 However, data are showing that ECMO can be successfully used in the elderly cardiogenic shock patients. The outcomes may not be as favourable as those seen in younger patients but are deemed acceptable in this high mortality risk patient group.9,10
Our study aimed to identify the risk factors that would be associated with increased risk of mortality in the elderly patient population supported with ECMO due to cardiogenic shock following cardiac surgery and help identify a sub-group of the elderly population that would most benefit from ECMO support.
Methods
This was a retrospective analysis of 40 consecutive elderly patients in whom ECMO was initiated due to postcardiotomy heart failure in a single tertiary care institution from 1 January 2009 to 31 December 2018. The study was approved by Vilnius Regional Bioethics Committee (Lithuania), reference number 158200-16-850-259. Information on patient’s demographic variables, comorbidities, pre-existing medical conditions and perioperative data were collected retrospectively from medical records.
The study sample of this analysis included only V-A ECMO cases due to cardiogenic shock, which occurred during or after cardiac surgery. One patient was started on ECMO support for cardiogenic shock due to ventricular septal defect associated with acute myocardial infarction and subsequently bridged to cardiac surgery was excluded from the analysis.
All patients underwent a cardiac surgical procedure with a median sternotomy and cardiopulmonary bypass. Minimally diluted tepid blood cardioplegia, slightly modified from the originally described by Calafiore, 11 was used in the majority of patients. Custodial solution (HTK – Bretschneider, Dr Franz Kohler Chemie, Alsbach – Hanhlein, Germany) was used for myocardial protection. Cardioplegia was usually delivered in antegrade fashion at induction, followed by retrograde delivery through coronary sinus cannulation or completed vein graft during coronary revascularization.
ECMO was considered in cases when patients were unable to be weaned from cardiopulmonary bypass. Following the first unsuccessful attempt, the patient was left on bypass for another 45-60 minutes of reperfusion, and insertion of IABP was performed (if appropriate). If second attempt failed (after optimization of preload) and vasoactive-inotropic score (VAS) exceeded 50 (dopamine (mcg/kg/min) + dobutamine (mcg/kg/min) + 100 × epinephrine dose (mcg/kg/min) + 10 × milrinone dose (mcg/kg/min) + 100 × norepinephrine dose (mcg/kg/min), on the team decision basis ECMO was initiated. The same VAS was applied for patients in the intensive care unit.
In our study, we evaluated the ability of European System for Cardiac Operative Risk Evaluation (EuroSCORE II), Simplified Acute Physiology Score (SAPS II), Sequential Organ Failure Assessment (SOFA) and Survival after Veno–Arterial ECMO (SAVE) scores to predict adverse outcome in ECMO-supported elderly postcardiotomy patients. EuroSCORE is a risk model that allows the calculation of risk of death after cardiac surgery based on 18 preoperative parameters. 12 The SAPS II is a mortality estimation tool which is made of 15 physiological and disease-related variables. 13 The SOFA is built of six parameters, each representing an organ system. 14 In SAPS II and SOFA scores, the worst physiological variables are collected within 24 hours of a patient’s intensive care unit (ICU) admission. The SAVE is designed to assist the prediction of survival for adult patients undergoing ECMO for refractory cardiogenic shock. Patient’s diagnosis, age, weight and organ systems variables are used to predict the outcome. SAVE score ranges from −15 to 15 points, where 0 equates to a 50% chance of survival. 15 Clinical Frailty scale (CFS) was used to define the level of frailty in our population. The CFS ranges from 1 (very fit) to 9 (terminally ill) based on descriptors of activity and functional status. 16
ECMO management
In 16 (40%) cases, ECMO was initiated intra-operatively, another 24 (60%) were initiated in intensive care, according to the same inotropic requirement criteria. In 33 (82.5%) cases, intra-thoracic cannulation was used, and only 7 (17.5%) patients underwent peripheral cannulation. If intra-thoracic cannulation was used, cannulas were placed through stab wounds and tunnelled, secured with two pledgeted purse-string sutures with tourniquets, brought through the skin of the anterior abdominal wall in the subcostal region. The chest was closed using standard surgical techniques. If peripheral cannulation was used, a percutaneous approach was utilized using Seldinger technique or direct surgical cut down of the corresponding femoral artery. A distal perfusion catheter placed in the femoral artery (8 Fr) or posterior tibial artery (4-5 Fr) for retrograde perfusion was used if optimization of distal leg perfusion was required. In all cases of peripheral cannulation near-infrared spectroscopy (INVOS5100 cerebral/somatic oximeter, Medtronic Inc, Minneapolis, MN, USA) monitor was used to access the adequacy of distal extremity perfusion.
Typically, 5000 units of heparin were given during cannulation if the patient was not on cardiopulmonary bypass. Heparin infusion was started when patients showed no signs of increased bleeding but not before the next postoperative morning. Anticoagulation targeted ACT levels of 180-220 seconds. Resternotomy for bleeding in patients on ECMO and stable hemodynamics was performed in cases when coagulopathy was not present or was adequately corrected, and drainage per 8 hours was ⩾1500 mL. In patients with unstable hemodynamics and the presence of continuous blood loss, threshold for resternotomy is reduced.
ECMO flows were maintained to keep mixed venous oxygen saturation greater than 60%. The target level of haemoglobin during ECMO procedure was 90-100 g/L. Platelet count was maintained 40,000-60,000 cells/mm3 for non-bleeding patients and >100,000 cells/mm3 in case of active blood loss. If coagulopathy and signs of bleeding occurred, fresh frozen plasma, clotting factor concentrates and cryoprecipitate transfusion was performed to support the INR <1.5 and fibrinogen level >200 mg/dL.
Weaning from ECMO support was initiated following at minimum of 48 hours of treatment, after evidence of recovery of cardiac function based on cardiac ultrasound and hemodynamic evaluation. Echocardiographic evaluation was performed by attending cardiologist. Aortic velocity time integral (VTI) ⩾10 cm and left ventricle ejection fraction (LVEF) of more than 20-25% at an ECMO flow of 2 L/min were considered as signs of myocardial recovery.
After successful weaning, trial decannulation was usually performed in the operative room. In 31 (77.5%) patients, intra-aortic counterpulsation was used before ECMO implantation, in another 3 (7.5%) IABP was inserted to facilitate weaning from extracorporeal life support.
Statistical analysis
Statistical analysis was performed using the data acquisition and analysis software package SPSS 23.0 (IBM Corp., Armonk, NY, USA). The quantitative normality of continuous data was evaluated using the criteria of histograms, rectangular diagrams and the Shapiro–Wilk test (p > 0.05). The quantitative continuous data distributed outside the normal distribution presented as the median and quartiles intervals. The categorical data expressed as a percentage. Categorical variables (between patients who survived to hospital discharge versus those who did not) were compared using the χ2 or Fisher criterion. The Mann–Whitney–Wilcoxon test was used to compare quantitative continuous data. Univariate logistic regression analysis of risk factors was performed, and variables with the p value of less than 0.1 were included in multivariate regression analysis. P-value < 0.05 considered as statistically significant.
Results
Between 2009 and 2018, 119 salvage VA ECMO procedures were performed in 8554 consecutive cardiac surgical patients (1.4% of all operated patients). Forty patients were older than 70 years and were included in the final analysis as ‘elderly group’. The preoperative demographics and perioperative data of the study group are shown in Table 1. The median age in the study group was 76 years (72-78). Twenty four patients (56%) in the elderly group were successfully weaned from ECMO, eight (20%) survived to hospital discharge. Preoperatively median left ventricular ejection fraction for the study group was 47.5% and the overall median frailty score was 5. Perioperative variables were compared in between survivors (n = 8) and non-survivors (n = 32) group (Table 2). There was no significant difference in the majority of hemodynamic variables, except from levels of pre-ECMO lactate, which were significantly higher in non-survivors group (5.7 (4.5-7.4) vs 11.5 (8.2-716.8) mmol/L). There was a borderline significant difference of aortic cross-clamp time and significantly higher use of inotropes (39 (21.5-40.5) vs 60 (54.3-73.5). The median duration of ECMO was 118 (89-154) hours. Distribution of variables included in univariate analysis is presented in Table 3. None of the non-modifiable preoperative demographic variables showed significant differences between groups, except composite risk stratification scores. Elderly non-survivors had significantly higher SOFA and SAVE scores (9 (8-11.3) vs 6.5 (5.8-7) and −11.5 (−15 to −9) vs −6 (−6.6 to −4.8)). Receiver operating characteristic (ROC) curve analysis of risk prediction scores revealed that SOFA score was the most accurate in prediction of elderly ECMO patient mortality with highest area under the curve in comparison with SAVE, SAPS and EuroSCORE (0.88 (95% CI = 0.7-1.0) vs 0.79 (95% CI = 0.6-0.9) vs 0.62 (95% CI = 0.4-0.8) vs 0.4 (95% CI = 0.2-0.6) (Figure 1).
Baseline clinical characteristics of study population.
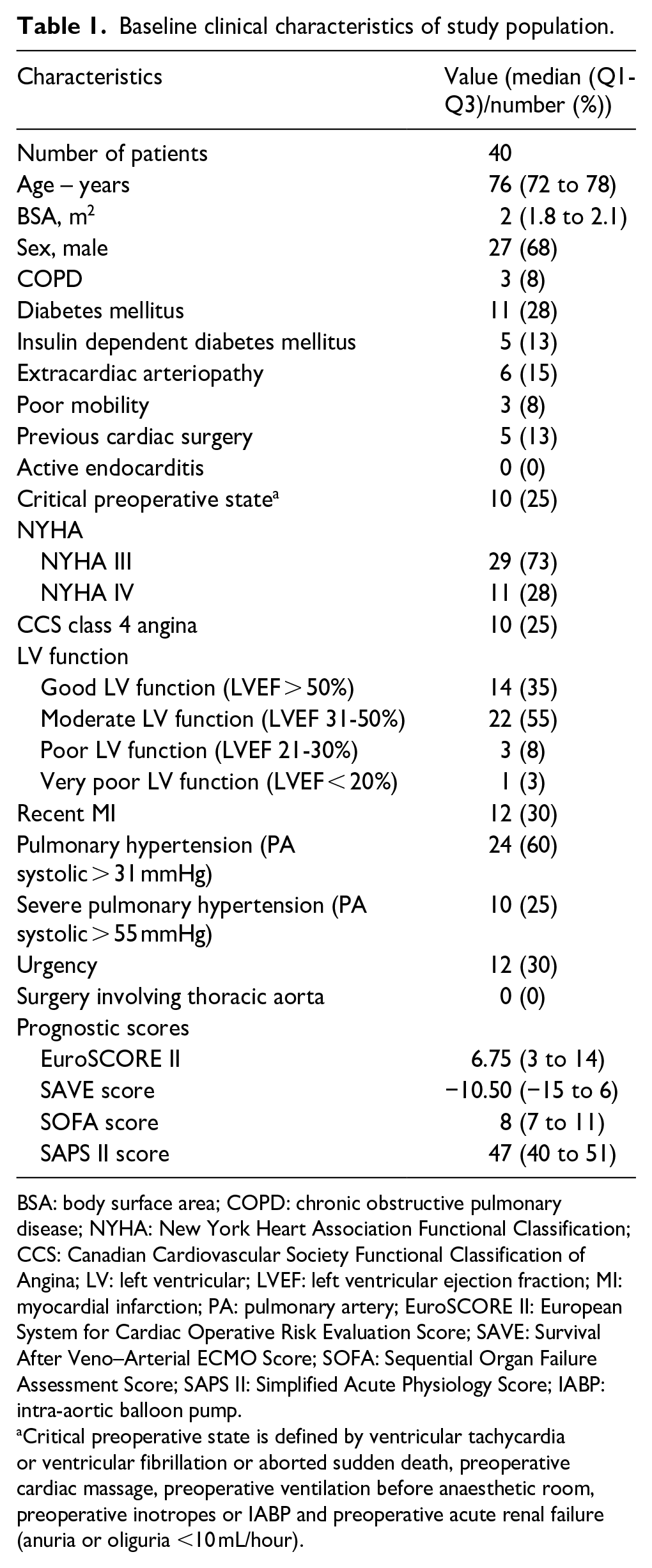
BSA: body surface area; COPD: chronic obstructive pulmonary disease; NYHA: New York Heart Association Functional Classification; CCS: Canadian Cardiovascular Society Functional Classification of Angina; LV: left ventricular; LVEF: left ventricular ejection fraction; MI: myocardial infarction; PA: pulmonary artery; EuroSCORE II: European System for Cardiac Operative Risk Evaluation Score; SAVE: Survival After Veno–Arterial ECMO Score; SOFA: Sequential Organ Failure Assessment Score; SAPS II: Simplified Acute Physiology Score; IABP: intra-aortic balloon pump.
Critical preoperative state is defined by ventricular tachycardia or ventricular fibrillation or aborted sudden death, preoperative cardiac massage, preoperative ventilation before anaesthetic room, preoperative inotropes or IABP and preoperative acute renal failure (anuria or oliguria <10 mL/hour).
Comparison of intraoperative variables for elderly ECMO survivors and non-survivors groups.
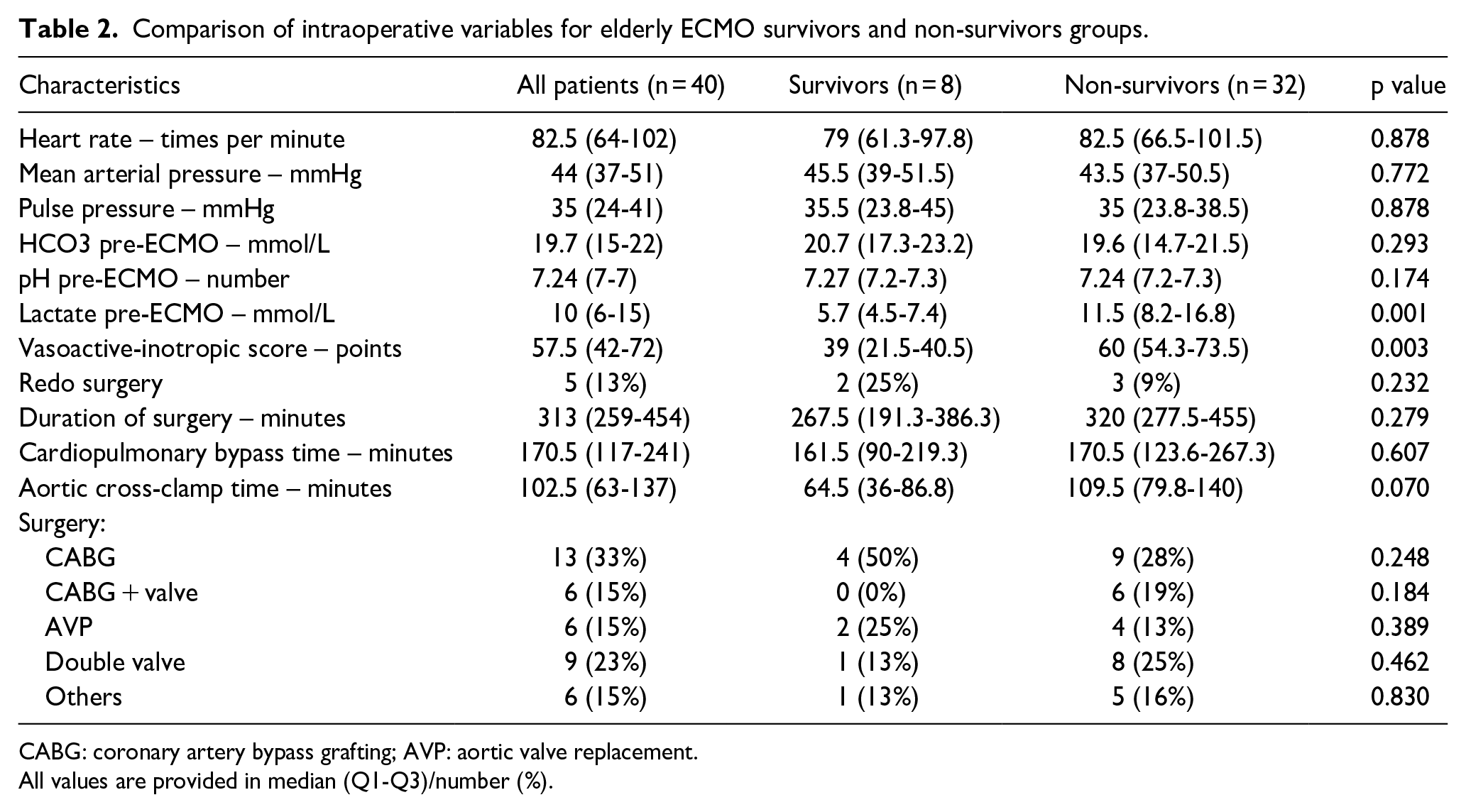
CABG: coronary artery bypass grafting; AVP: aortic valve replacement.
All values are provided in median (Q1-Q3)/number (%).
Univariate analysis of risk factors for mortality in elderly postcardiotomy ECMO patients (all values are provided in median (Q1-Q3)/number (%)).
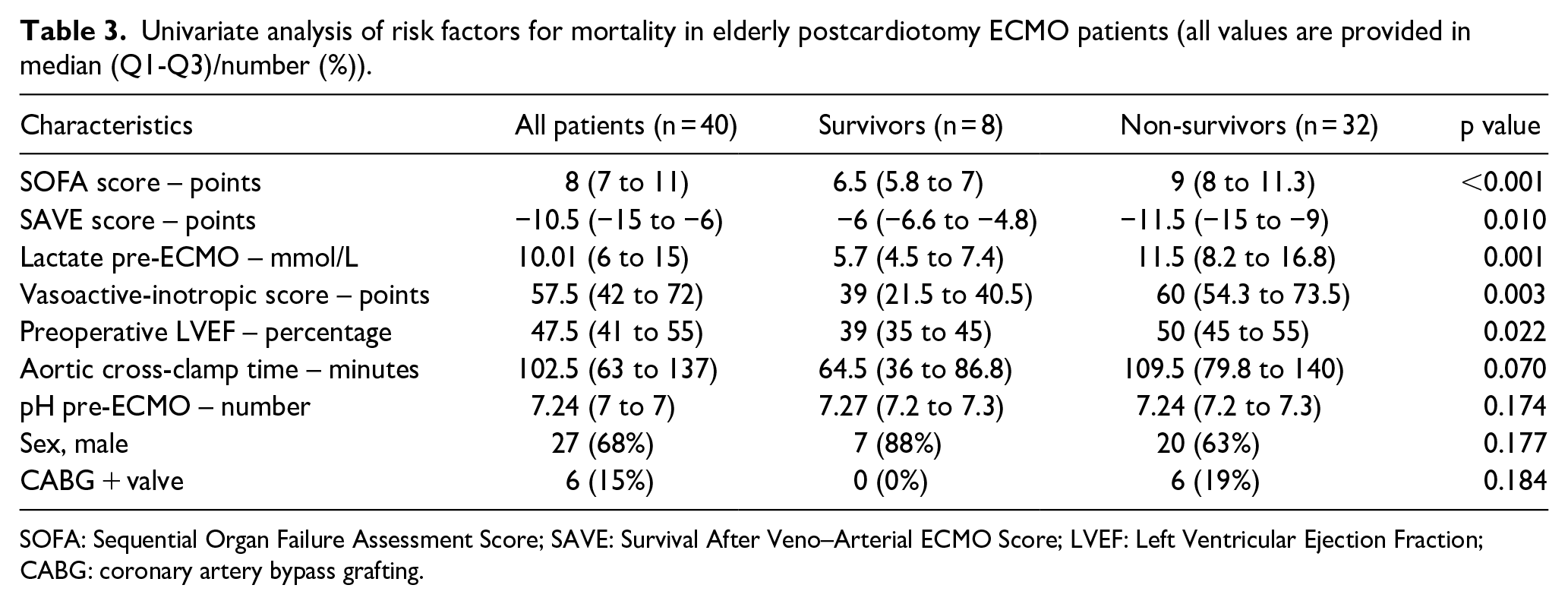
SOFA: Sequential Organ Failure Assessment Score; SAVE: Survival After Veno–Arterial ECMO Score; LVEF: Left Ventricular Ejection Fraction; CABG: coronary artery bypass grafting.
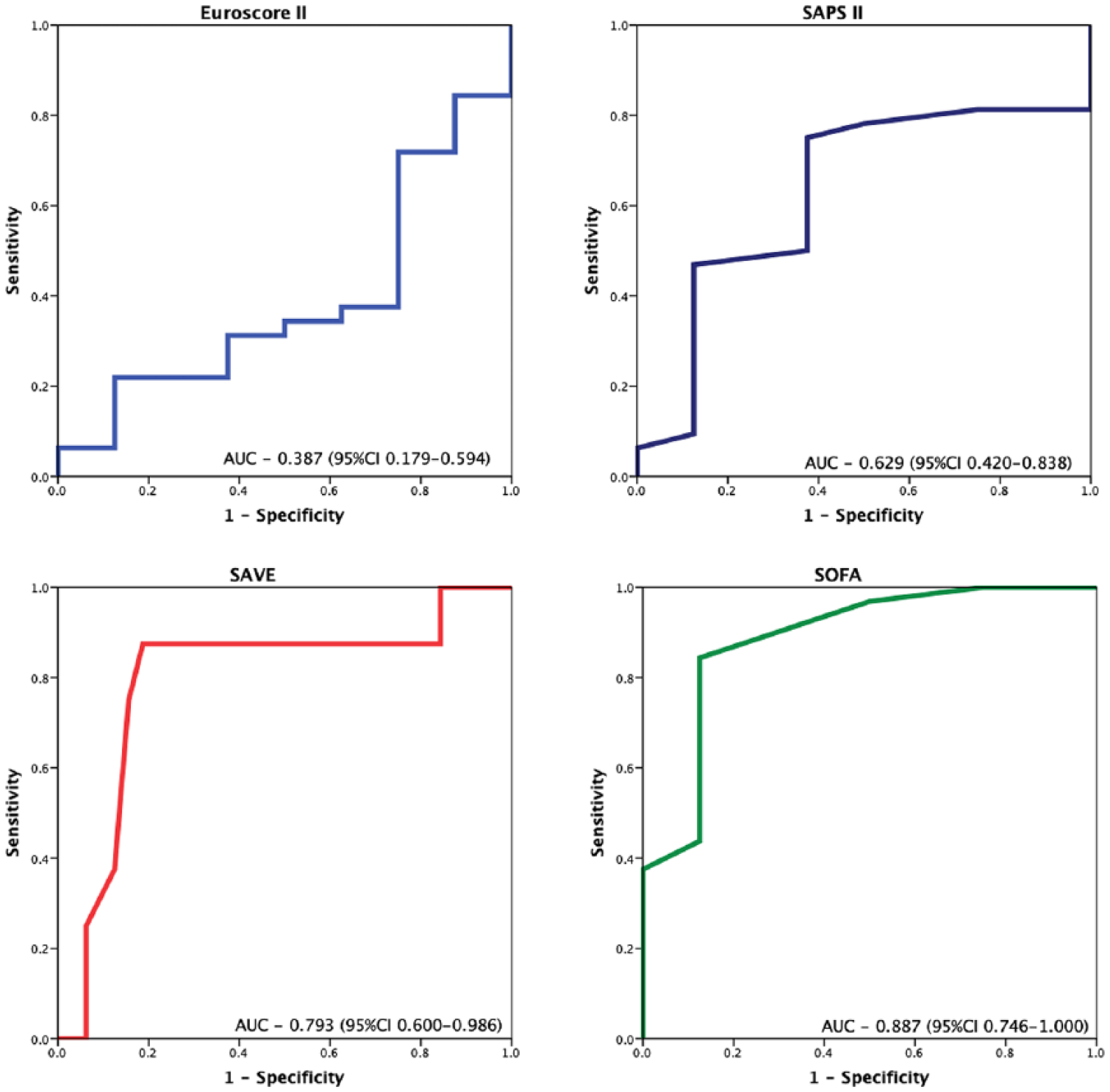
ROC curves for predicting of mortality in elderly patients including EuroSCORE II, SAFE, SOFA and SAPS II scores.
Logistic regression confirmed the association between pre-ECMO lactate and mortality of elderly ECMO patients (p = 0.027, 95% CI = 1.0-1.7).
Discussion
Aging population, advances in cardiac surgical techniques and increased expectations of patients and their relatives have led to a change of profile of patients accepted for cardiac surgery. Given the trend of our ageing population, one might expect that the proportion of the elderly undergoing cardiac surgical procedures will continue to rise. Extracorporeal life support is a widely established therapy for younger patients with refractory cardiogenic shock. However, the efficacy of its use in the elderly remains debated. Survival to hospital discharge of elderly patients who were treated with ECMO for postcardiotomy heart failure was 20%, which is comparable with other studies with hospital survival rates of less than 25%.9,17 Although older age itself is associated with a greater number of comorbidities and lower survival rates, age itself should not preclude patients from ECMO support following cardiac surgery. A recent study has shown that lower hospital survival rates were among the elderly postcardiotomy patients supported with ECMO; however, 100% of patients surviving to discharge were alive beyond 1 year. 9 In a large prospective cohort study including 1225 acute myocardial infarction patients, authors found that elderly patients without left ventricular failure had subsequently better survival the first year after the myocardial infarction than much younger patients with left ventricular failure. 18 Identification of patients with the best chances for survival might play a pivotal role in decision-making for using extracorporeal technology in elderly cardiac surgical patients.
Pre-ECMO lactate levels, inotropic score, SOFA and SAVE scores were among the most powerful predictors of unfavourable outcomes in univariate analysis in our study. After multivariate analysis, pre-ECMO lactate levels remained the only significant predictor of hospital mortality. The same results were found in a recent study, 17 where authors found lactate levels greater than 6 mmol/L before starting VA ECMO to be the only predictor of in-hospital mortality. Multiorgan failure before ECMO implantation is a well-described phenomena related to adverse outcomes in younger patient population. 19 SOFA score in our study patients, as an indicator of multiorgan failure, was more accurate than the SAVE score in predicting outcomes (area under the ROC curve 0.89 vs 0.79). This difference might be due to a delay in initiating treatment which might be associated with adverse outcomes. Elderly patients with multiple comorbidities and suboptimal organ function might be more sensitive to the negative consequences of cardiogenic shock. Early decision to proceed with ECMO implantation in this vulnerable patient population might be associated with increased survival. Out 24 weaned from ECMO patient, only 8 (33%) were discharged from hospital. This finding suggests that the elderly population is frail and due to various complications following ECMO treatment may have an undesirable outcome. In patients who survived to discharge, we found that SOFA score and lactate levels were lower compared to those who did not. This finding supports that to reduce morbidity and mortality in elderly patients after cardiac surgery with refractory cardiogenic shock, ECMO treatment should be considered and initiated without a delay.
It has been shown by several studies that frail patients have a higher likelihood of mortality, morbidity and major adverse cardiovascular and cerebral events following cardiac surgery.16,20,21 We could not confirm these data in the ECMO-treated patient group, as not all postcardiotomy elderly patients with cardiogenic shock were supported with ECMO. Although frailty score was not used for decision-making, the frailest patients were treated with less-invasive techniques than ECMO. Further research is needed to determine whether patients determined as frail could benefit from the use of ECMO in the treatment of postcardiotomy shock.
Our study has several limitations. The design of the study was a retrospective investigation. The relatively small number of patients involved limited its statistical power. It was a single-centre study, representing our centre experience in providing ECMO therapy in elderly cardiac surgery patients.
In conclusion, ECMO can be used in elderly patients. The decision to use ECMO should be taken earlier and take into account the degree of metabolic derangement and the comorbidities. Further multicenter prospective studies with a larger number of patients involved are needed to single out a group of elderly patients who would benefit from ECMO treatment in case of developing cardiogenic shock, refractory to medical treatment in a perioperative period.
Supplemental Material
Supp_Mat_907746_-_Evaluation_of_risk_factors_for_adverse_outcome_in_ECMO_supported_elderly_postcardiotomy_patients_ – Supplemental material for Evaluation of risk factors for adverse outcome in extracorporeal membrane oxygenation–supported elderly postcardiotomy patients
Supplemental material, Supp_Mat_907746_-_Evaluation_of_risk_factors_for_adverse_outcome_in_ECMO_supported_elderly_postcardiotomy_patients_ for Evaluation of risk factors for adverse outcome in extracorporeal membrane oxygenation–supported elderly postcardiotomy patients by Robertas Samalavicius, Ieva Norkiene, Nadezda Scupakova, Jurij Sabliauskas, Karolis Urbonas, Povilas Andrijauskas, Agne Jankuviene, Lina Puodziukaite, Aleksejus Zorinas, Vilius Janusauskas, Kestutis Rucinskas, Kestutis Laurusonis and Pranas Serpytis in Perfusion
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.