
Abstract
Preventing the introduction of air while a mechanical circulatory support device is being implanted is critical for successful outcomes. A substantial amount of air may be introduced into the circulation during the pump-to-outflow and/or pump-to-inflow port connection, which can be detrimental to optimal pump function and long-term survival. We have developed a novel connecting sleeve that enables an airless connection of the continuous-flow total artificial heart to the conduits. Herein, we describe the device design and surgical techniques evaluated in vivo.
Introduction
Air introduction inevitably occurs during the attachment of mechanical circulatory support (MCS) pumps to vascular and atrial conduits. The atmospheric air present enters into the space available within chambers and remains entrapped unless removed properly. The negative effects of air deposition into the circulatory system such as multi-organ functional deterioration have been previously reported in the literature.1,2 The current techniques of de-airing and prevention of air entrapment are limited to basic attempts of careful device-to-conduit connection, priming of connection lines, and proper device manipulation to avoid excessive air engagement into circulation during connection. These techniques are imperfect, and the risk of air embolism remains since the access to atmospheric air is never fully limited during the actual device-to-conduit connection process. The process is further complicated by devices that have a unique design architecture, which imposes additional demands for a quick and effective connection technique during surgical implantation. 3 At the time of connection, all connection ports of the Cleveland Clinic continuous flow total artificial heart (CFTAH) are oriented downward, which makes visualization and therefore direct control during device connection even more cumbersome. Limited access inside the chest further complicates the attempts to prevent air entrapment during connection.
In order to address this issue and to enable measured and controlled air removal, we have developed and evaluated a novel connecting sleeve that allows an airless connection of the CFTAH to the vascular conduits. Our technique and early experience with an improved connection device design performed in acute in vivo implantations is reported herein.
Methods
The Cleveland Clinic total artificial heart (CFTAH) is a double-ended centrifugal pump intended for total cardiac replacement. 4 The device has two inflow and two outflow ports (Figure 1(a)). The unique architecture features a single motor that performs through two independent impellers (left and right) mounted on the same rotor and running at the same speed (Figure 1(b)).
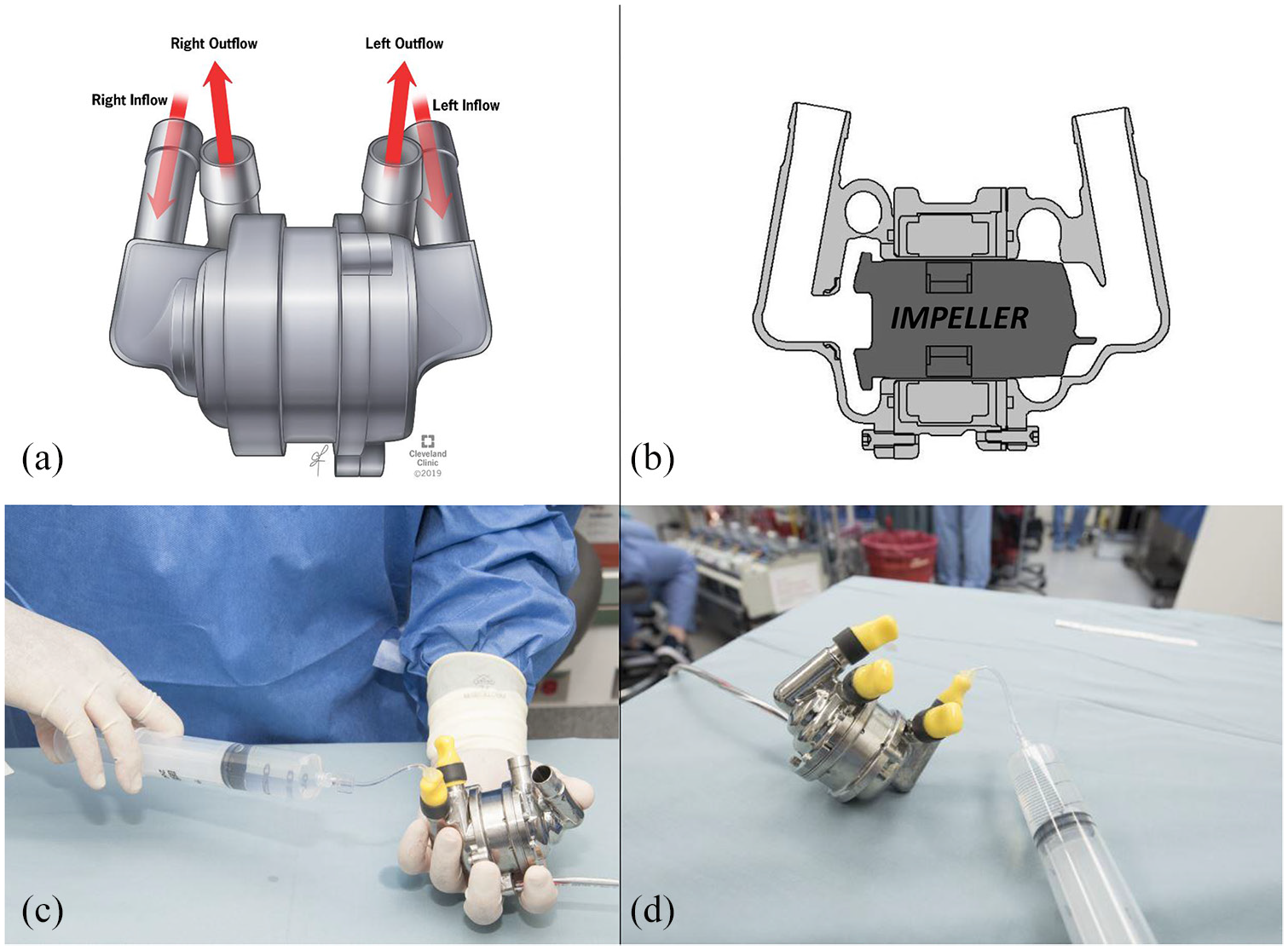
(a, b) Double-ended continuous flow total artificial heart, (c) device priming procedure, and (d) sealed device after complete de-airing.
The study protocol was approved by Cleveland Clinic’s Institutional Animal Care and Use Committee (study protocol number: 2019-2106), and all animals received humane care in compliance with the Guide for the Care and Use of Laboratory Animals. The device testing has been performed in acute in vivo (n = 2) CFTAH implants (Jersey calves, weight: 77.8 and 80.8 kg).
Procedures consisted of pump priming with normal saline and heparin (1 mL in 60 mL of saline) (Figure 1(c) and (d)) and application of a specifically designed, flexible connection sleeve (Figure 2(a)). The silicone sleeve (0.3-0.5 mm thick) was prototyped using a multilayer dip-coating technique over a 3D-printed mandrel (Material: MED-6,606, NuSil™ Carpinteria, CA) and made entirely of a single material. A peel-off suture line was added along the long axis to enable easy removal. The peel-off feature was designed to disrupt the integrity of the de-airing sleeve when mechanical force (by manual pulling) is applied to the body of the sleeve. De-airing sleeve was placed on each outflow port (conduit) and proximal port (port) ends (Figure 2(b)). Existing air was drawn out upward from an open pressure port (de-airing port). The conduit and pump ports were connected within the sleeve (Figure 2(c)) (with the air fully excluded from the circuit) and secured (Figure 2(d)). The CFTAH was started at the minimum speed (2,200 r/min) after connection.
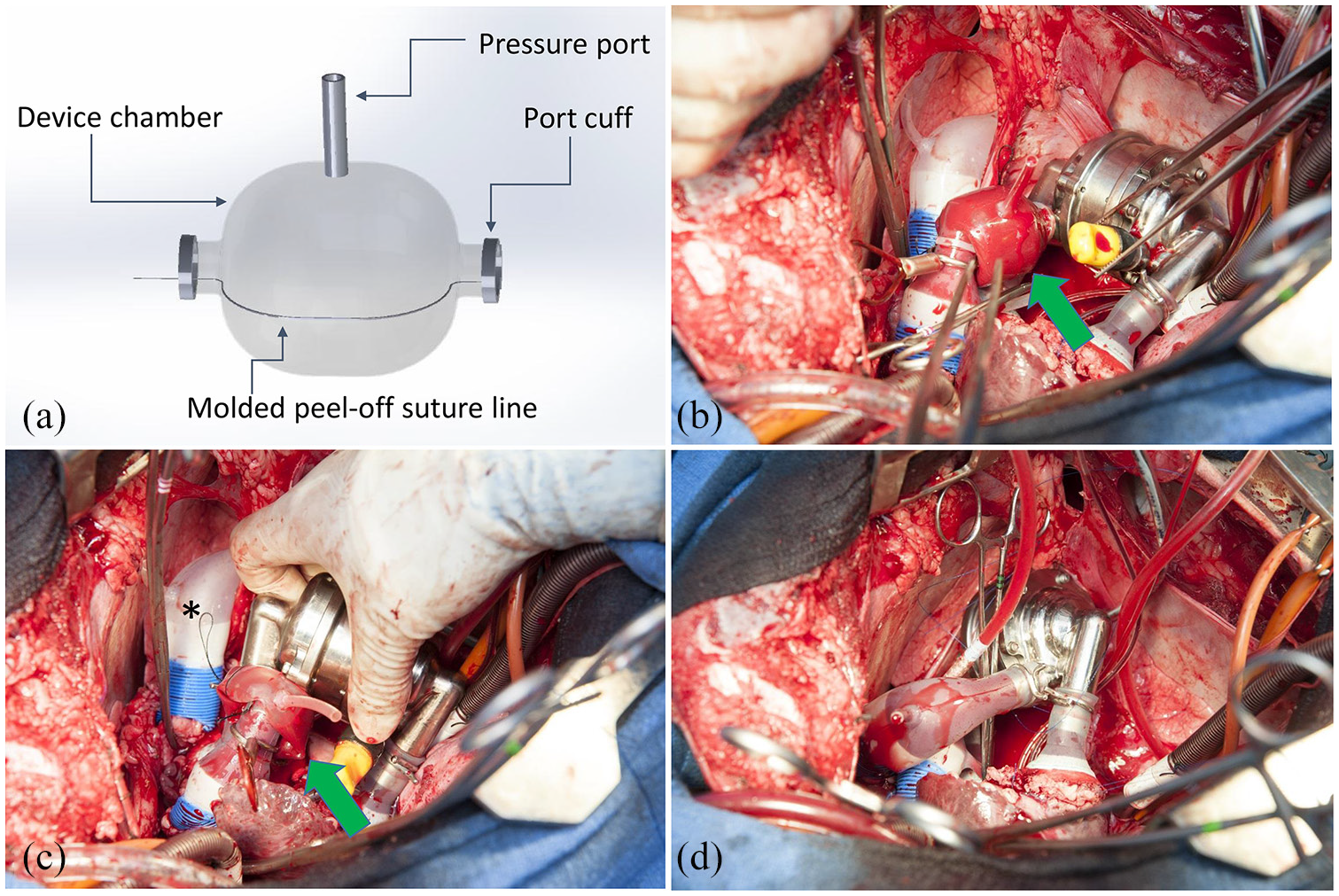
(a) Connecting sleeve; (b) pump inflow is connected with aortic prosthesis (arrow); (c) the aortic conduit and metallic pump inflow port are connected within the connecting sleeve (asterisk—the peel-off suture end intended for sleeve removal); and (d) device connection is complete, the peel-off suture has been removed along the long axis of the sleeve, and the sleeve is fully removed from the surgical field. The metallic clamps are then placed around each pump port to prevent disconnection of the conduit from the pump after implantation.
Results
The prototype de-airing sleeve was successfully applied in CFTAH acute implantation cases (n = 2). In both cases, each outflow port of the pump was successfully connected to the ascending aorta and the pulmonary artery using the de-airing sleeve. In all cases, after the devices were connected to the respective outflow ports using this sleeve and technique, the residual air was identified and evacuated through the pressure line at the side wall of the de-airing sleeve. The air deposition was noticeable at the top wall of the sleeve in all attempts. The priming of the sleeve was not required. The devices were fully expanded by blood and saline present within the circuit. After successful air removal, the pump and vascular conduits were connected and secured within the sleeve. After the connection was ensured, the peel-off suture of the sleeve was pulled off from two sides, along the device’s long axis. The sleeve was opened up along the long axis and was subsequently removed fully without leaving any residual parts in the surgical field. After sleeve removal, the vascular conduits were clamped using a dedicated circular fixating clamp to prevent any disconnection. No alterations were made in the surgical procedure before or after sleeve application.
Discussion
MCS device implantation is a well-established procedure, but complexities remain in trying to remove entrained air from the device and its circuit before use.1,5 Air embolism remains a significant complication of the total artificial heart, caused by ineffectual de-airing of the blood pump, which allows embolization of the retained air. 2 The entrained air may cause immediate issues, such as a drop in pump pressure rise, flow rate, and power, especially if more air than the impeller can handle is entrapped. This may cause air cavitation and impeller rubbing that in turn may damage the impeller surface and make pump biocompatibility a concern. The prime fluid can be lost during the connecting process and be quickly replaced by air under the effects of atmospheric pressure.
One important aspect of the MCS implantation procedure involves proper air removal and assurance of no residual or pooled air in the native vascular conduits or inside the mechanical device chambers. Several improvements have been made to optimize the device and to improve the cardiac surgical technique related to cardiac de-airing that affects the surgical outcomes.6–8
The most important limitation of the seamless device connections we performed in the past 7 was the difficulty of removing the sleeve after connection, which required tight fixation of metallic pump ports and vascular conduits. That has been found to be a limiting factor, since removing sleeve material with scissors or a surgical blade could potentially disrupt the continuity of the vascular grafts. Also, the placement of the metallic clips used for securing the connection sites (to prevent disconnection) was cumbersome. The de-airing process has been additionally aggravated, since the metallic body of the pump impedes visualization and makes the air identification procedure completely blind. In this early experience, the removal procedure per se was found to be easy in all cases. Moderate force has been required for successful removal. No need for scissors or surgical blade was deemed necessary with this optimized design with a peel-off feature.
The peel-off feature of the current connecting sleeve has been enabled by molding a suture line for quick removal that doesn’t alter the port-to-vessel connection. The connecting sleeve allows air visualization through its wall and tolerates device handling (position adjustment before fixation) during the de-airing and connection procedure. The described technique shortens the intraoperative time by enabling careful monitoring of air removal and visual metrics during the implantation procedure.
Development of new MCS device implantation techniques should be continued and improved, along with the engineering and development of the device technology itself. Proper strategies for de-airing, reliable device-to-vascular conduit connection, and effective use and reduction of cardiopulmonary bypass and cross-clamp times will continue to affect subsequent outcomes of these complex procedures.
Footnotes
Acknowledgements
The authors thank our Cleveland Clinic colleagues Jianzhong Cang for prototyping and Perfusion Service personnel for their technical support during these studies.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially supported with funding from the National Institutes of Health/National Heart, Lung and Blood Institute (NHLBI R01HL096619).
Study approval
The study protocol was approved by Cleveland Clinic’s Institutional Animal Care and Use Committee (study protocol number: 2019-2106).