
Abstract
Introduction:
Air in extracorporeal membrane oxygenation circuit may lead to deleterious consequence.
Case report:
Three cases of air in extracorporeal membrane oxygenation were presented. Air was introduced from right jugular venous sheath during percutaneous septal repair, pulmonary artery catheter during intensive care unit, and sewing holes on atrial wall during surgery respectively. Accidents in Case 2 and Case 3 were successfully managed, while Case 1 was suspected of cerebral air embolism through transseptal right-to-left shunt.
Discussion:
With extracorporeal membrane oxygenation being widely applied in more clinical settings, especially in catheterization lab, risks of air in extracorporeal membrane oxygenation increase. More attention should be paid to patients with communication between right and left heart system, especially in situations when venous accesses’ exposure to air could not be avoided.
Conclusion:
Air in the extracorporeal membrane oxygenation circuit should never be overemphasized, especially during special procedures.
Keywords
Introduction
Air in extracorporeal membrane oxygenation (ECMO) circuit may lead to deleterious consequence, either by tripping the pump or causing air embolism. As venoarterial ECMO is applied with extended indications and more complex interventions are performed on ECMO, 1 risks increased. Here we present three typical cases we encountered recently. Our institutional review board approved the case reports and waived the need for informed consent.
Case report
Case 1
A 79-year-old man was admitted with diagnosis of acute anterior-inferior-wall infarction, post-infarction ventricular septal defects, and cardiogenic shock. Considering high-surgery risk, multidisciplinary team decided to do percutaneous septal closure and coronary angioplasty on ECMO. ECMO was cannulated via right femoral vein and left femoral artery. After full flow (3,500 mL/min) was achieved, percutaneous septal repair was started via right jugular vein and right femoral artery. During the procedure, massive air was seen returning into venous line and oxygenator. Arterial line was clamped immediately, pump was stopped, and air was expelled through oxygenator. Air was considered introduced from right jugular venous sheath by negative pressure. To avoid more air in, pump speed was maintained below 2000 r/min until septal repair was completed. Hemodynamic parameters and circuit were closely monitored. De-air was performed twice subsequently. No visible air bubbles entered arterial line during entire procedure. Then, coronary stenting was performed via right brachial artery. However, after the procedures, the patient gradually developed progressive conscious disturbance. Although he was weaned from ECMO with cardiac function recovered after 7 days, he did not survive because of irreversible brain injury. Brain injury was considered might be related to cerebral air embolism through ventricular septal right-to-left shunt. Brain image was not performed to confirm the diagnosis.
Case 2
A 17-year-old man diagnosed with hypertrophic cardiomyopathy underwent heart transplantation. Femoral venoarterial ECMO (3,300 L/min, 2900 r/min) was implanted postoperatively because of primary graft failure. On the third day, continuous air bubbles were noticed entering the venous line. Arterial line was clamped, and air was expelled. Careful examination of all the venous accesses revealed that air came from an incompletely closed stopcock on pulmonary artery catheter. Circuit resumed normal work after shutting the stopcock. The patient was weaned from ECMO successfully after 6 days without neurological dysfunction.
Case 3
A 55-year-old woman was placed on femoral venoarterial ECMO from cardiopulmonary bypass due to primary graft dysfunction after heart transplantation. During chest closure, she was hypovolemia due to massive bleeding. ECMO speed was 3,000 r/min, while ECMO flow fluctuated greatly (1.0-2.5 L/min). A small amount of air entered venous line and oxygenator. After de-airing, the pump was restarted. Meanwhile, all the venous accesses were checked safely closed. It was noticed that right atrial wall was adhered to side holes of femoral venous cannula by negative pressure. Sewing holes on atrial wall were considered as the portal of air. Another possible reason might be cavitation caused by severe hypovolemia. After volume resuscitation and sewing holes repair, no more air entered circuit. The patient was discharged from hospital 1 month later with good neurologic outcome.
Discussion
Centrifugal pump generates negative pressure in venous side of ECMO as well as venous system of patients, which will be enhanced greatly if venous limb is kinked or occlusion, or if patients are hypovolemic. Any exposure to air in venous system may introduce air into venous limb of ECMO and even into arterial side, causing air embolism. Protocol of our institute is summarized in Table 1.
Protocol for air in ECMO circuit.
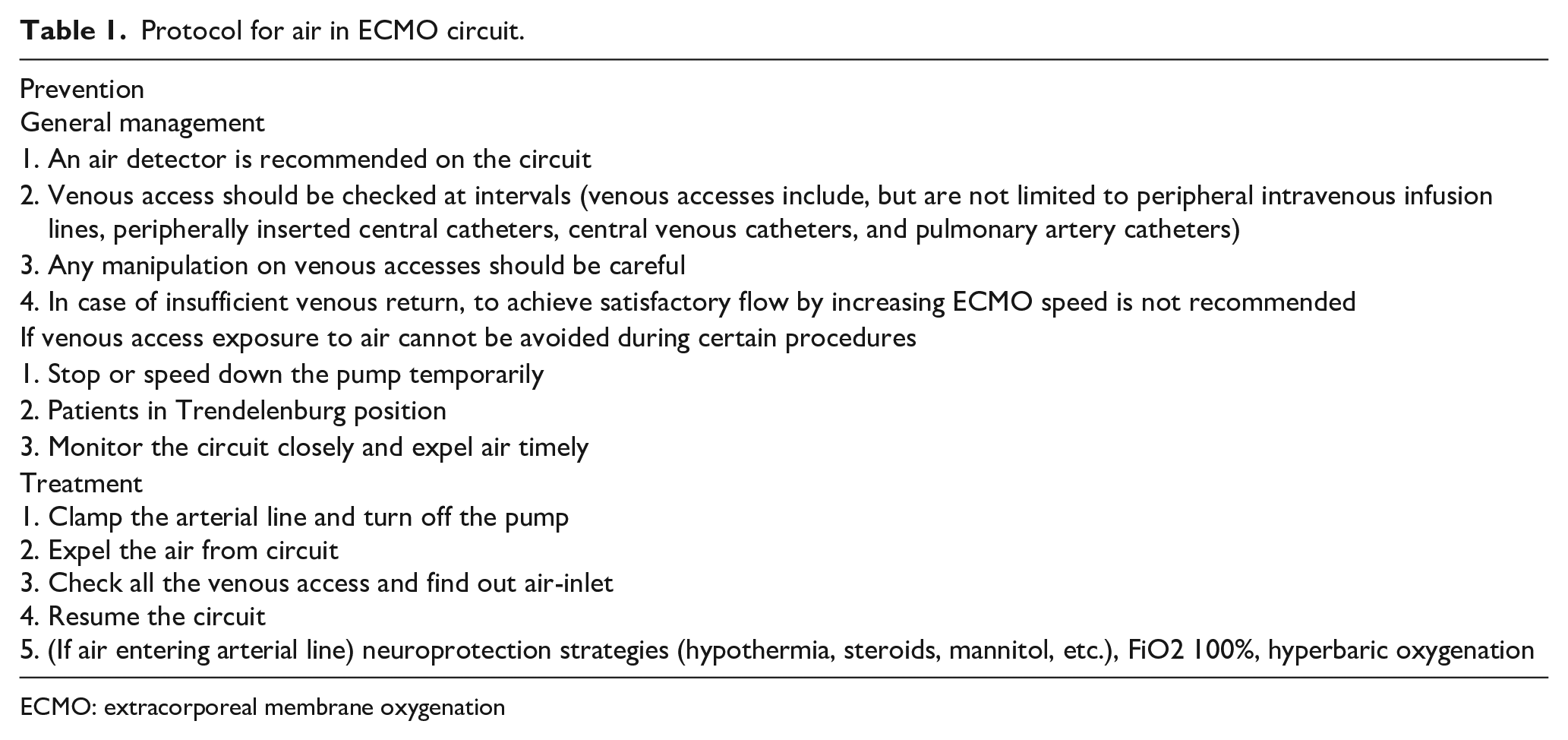
ECMO: extracorporeal membrane oxygenation
Case 2 was the most familiar clinical scene of air in ECMO, and ECMO specialists were able to prevent and manage the accident quickly and successfully. Case 1 and Case 3 were special as air was introduced during complex intervention on ECMO by medical staff who were not familiar with the principle of ECMO. Because of the working property of ECMO, massive air may be pulled in by incautious procedures which is considered safe in normal conditions. Therefore, every ECMO team member should be fully aware of the risks, and perform procedures or surgeries carefully to avoid exposure to air in venous system. However, sometimes exposure to air could not be avoided. One example is catheter interventions via venous access. In our limited experience, air intrusion could be reduced by flushing vascular catheters and retracting guidewire gently, but could hardly be eliminated. It is extremely important to monitor the circuit closely. If intracardiac shunt exists, arterial air embolism may occur, as shown in Case 1. Catheter interventions through venous access on ECMO in patients with intracardiac shunt should be regarded as high-risk procedure. We suggest ECMO should be stopped temporarily when venous access is exposed to air.
Theoretically, performing atrial septostomy on ECMO faces similar risks. However, arterial or cerebral embolism has rarely been reported.2,3 One possible explanation is that left atrium in patient requiring atrial septostomy is of extremely high pressure, which helps prevent air bubble into left atrium. Another explanation is that risks only present near the end of the process after atrial septal defect is made. Nevertheless, in our opinion, atrial septostomy on ECMO should also be regarded as high-risk procedure.
Conclusion
Air in the ECMO circuit can never be overemphasized as it may lead to fatal consequence. Every ECMO team member should be fully aware of the risks and be more careful. Risks of air embolism increase exponentially in patients with intracardiac shunt. More attention should be paid to these patients, especially in situations when air exposure could not be avoided.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.