
Abstract
Introduction:
The etiology of coronary artery aneurysms is unknown. Coronary atherosclerosis is considered to be the main etiology. This case reports a patient with a large coronary aneurysm of the right coronary artery.
Case report:
A 65-year-old woman was hospitalized with intermittent chest pain and underwent coronary angiography and echocardiography which showed a large coronary aneurysm of the right coronary artery. The patient recovered well after ligation of coronary artery aneurysms with additional coronary artery bypass grafting.
Discussion:
The etiology of coronary aneurysms is unknown, which is relatively rare and mostly secondary. Majority of coronary artery aneurysms are located in the right coronary artery. There is currently no standard treatment. Surgical treatment of coronary artery aneurysms may be considered as a safe treatment option.
Conclusion:
The standard surgical treatment for coronary artery aneurysms is unclear. For symptomatic large coronary aneurysms, ligation of coronary artery aneurysms with additional coronary artery bypass grafting can achieve good results.
Keywords
Case description
A 65-year-old woman was admitted to hospital with intermittent chest pain. She has 3-year history of coronary artery disease with previous myocardial infarction, which was treated with percutaneous coronary intervention (PCI) and stenting to left anterior descending artery. She was given atorvastatin, aspirin, and other medications for the secondary prevention. Latest computed tomographic (CT) coronary angiogram showed aneurysmal dilatation in the distal right coronary artery (RCA), decreased blood flow in the distal circumflex branch and the distal left anterior descending branch, and further enlarged the size of the aneurysm to 16.52 mm × 18.98 mm (Figure 1). The right atrium was compressed outward. The electrocardiogram showed sinus rhythm. Echocardiography showed that left ventricular dilation with impaired systolic function (LVEF was 50%), and there was not significant valvular disease. So here is our conclusion: Over the years, the patient’s aneurysm continued to expand and compress the left heart or any adjacent structures, affecting coronary blood flow. Until the patient comes in with intermittent chest pain, we discussed with the family the risks and benefits of the operation, combining the patient’s age, weakness, and heart function. The family decided to support the operation. Surgical summary: The aneurysm was opened and the inlet and outlet were sutured with acrylic sutures (Figure 2). Completed aneurysm repair was performed with additional coronary artery bypass grafting (CABG) (Figure 3). She recovered well after operation.
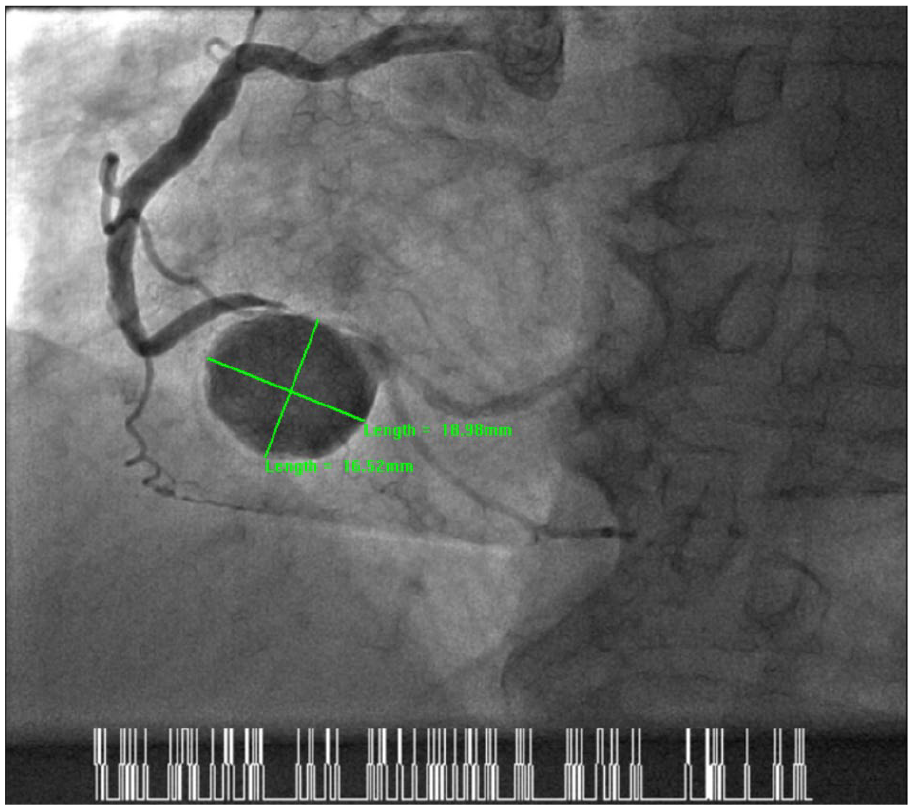
Coronary angiography showing aneurysmal dilatation in the distal right coronary artery, decreased blood flow in the distal circumflex branch and the distal left anterior descending branch, and the size of the aneurysm is 16.52 x 18.98 mm.
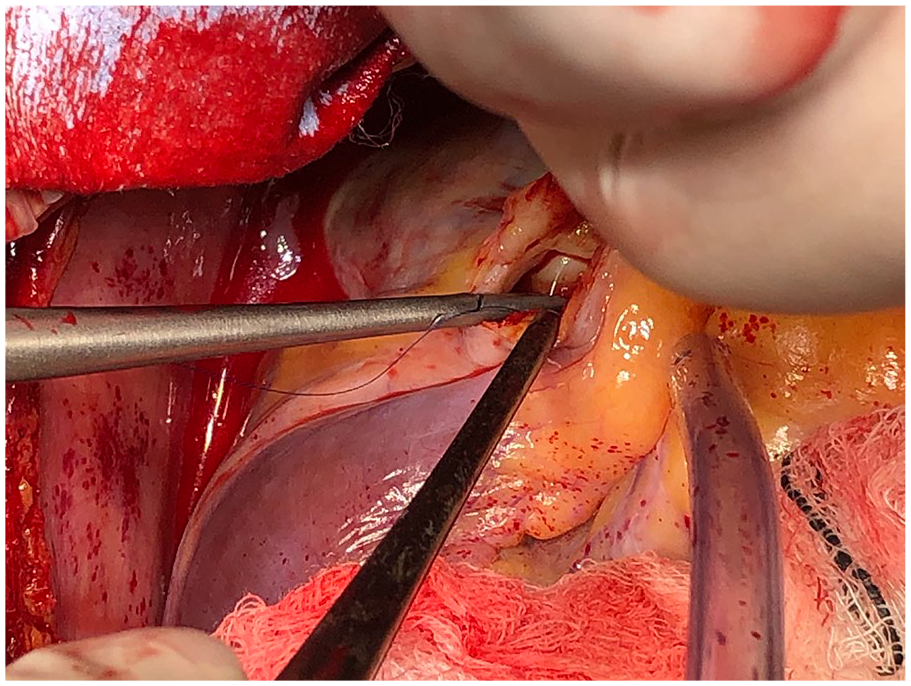
Opening and ligation of the coronary artery aneurysms.
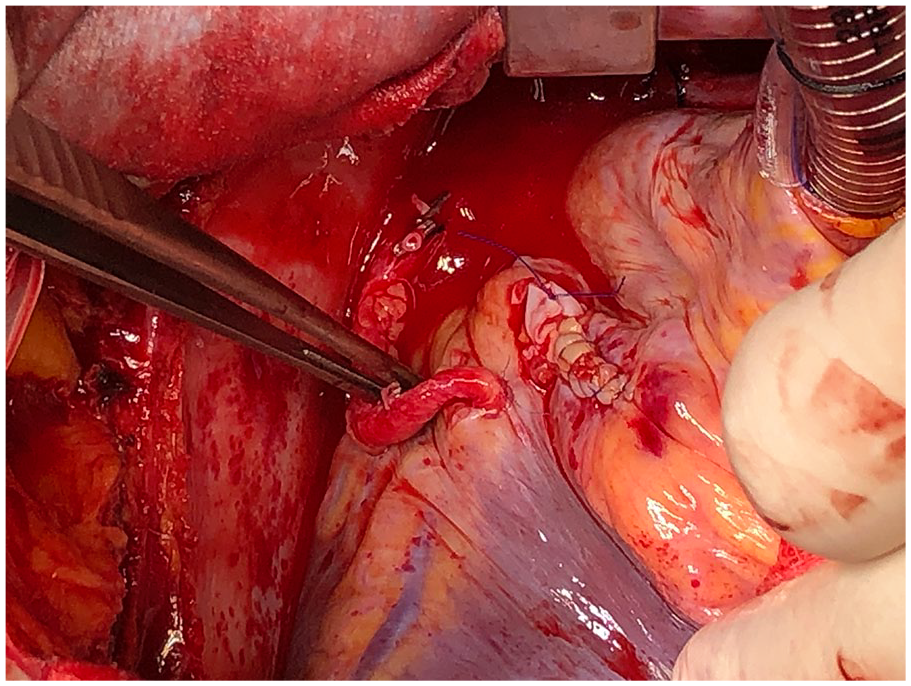
Completed aneurysm repair with additional CABG.
Discussion
Etiology
The etiology of coronary artery aneurysm (CAA) is still uncertain and it may relate to coronary atherosclerosis, Kawasaki disease, inflammation, and so on. It is rear condition with incidence of 0.3-5.3%.1–3 At present, coronary atherosclerosis is considered to be the most important cause. It may be dilatation after stenosis. 4 In children, the main cause of dilatation of coronary artery is secondary to Kawasaki disease, which is the second cause in adults.5–7 At present, CAAs have also been reported in patients with coronary heart disease after stent implantation, especially in patients with drug-eluting stents.8,9 But whether there is a potential connection between them needs to be further explored. In addition, some genome-wide association studies (GWAS) have found that variation on chromosome 9p21.3 may be associated with the occurrence of CAAs.10,11 This case is also a patient with coronary atherosclerosis which was treated with stent implantation in the left coronary artery, but not in the RCA. During the follow-up, RCA aneurysms appeared. The patient had no history of Kawasaki disease or specific inflammation, and the most likely cause is coronary atherosclerosis.
Diagnosis of CAA
CAA is diagnosed when its diameter is 1.5 times greater than the normal diameter. 12 At present, the diagnosis mainly relies on imaging, including intravascular ultrasound (IVUS), coronary angiography (CAG), coronary computed tomographic angiography (CTA), and color Doppler echocardiography. 13 The gold standard of diagnosis is IVUS. Using IVUS, diagnosis and treatment can be achieved at the same time. Follow-up, practicability, and trauma of Kawasaki disease in children lead to unsatisfactory results. Doppler echocardiography has the advantages of safety, simplicity, accuracy, and reliability and can observe the whole process of coronary artery dilatation and its evolution dynamically, but it cannot detect the lesions in the distal part of the coronary artery. Dual-source CT can complement echocardiography. The images are very similar to angiographic images. It has become a new non-invasive technology. This case was diagnosed by CAG and color Doppler echocardiography.
Treatment
At the present stage, the main treatment methods are drug therapy, interventional stent implantation, and surgical CABG. 14 Standard anti-lipid and antiplatelet therapy benefits patients with CAAs. 15 Coronary aneurysms are relatively rare and lack of high-quality randomized controlled trial (RCT) to provide in-depth summary of the disease. Now most of the information is from case reports. The standard surgical treatment is unclear. PCI is a relatively new treatment. There are also less data. 16 Studies have shown that surgical treatment is more appropriate when patients have symptoms and complications or CAA is larger and associated with coronary artery disease. 17 For symptomatic patients, surgical ligation/resection of a coronary aneurysm may be an option, along with bypass grafting of the affected coronary artery. 18 This case is of CAA near the large branch, with a large CAA (dilated to more than four times the diameter of the reference vessel), and can be treated surgically. 19 It achieved good results after ligation of CAA with additional CABG.
Conclusion
The standard surgical treatment for coronary aneurysms is unclear. For symptomatic large coronary aneurysms, ligation of CAA with additional CABG can achieve good results.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The National Natural Science Foundation of China. (No. 81660074). Project leader: Feng Wang.