
Abstract
Introduction:
Lactate dehydrogenase (LDH) is widely used as an indicator of pump thrombosis in a centrifugal pump. However, due to the low specificity of LDH, pump thrombosis is difficult to detect in the clinical environment. We measured plasma free hemoglobin (pfHb) with the portable device in ICU. The goal of this investigation is to evaluate its diagnostic ability for pump thrombosis.
Methods:
We enrolled 31 consecutive patients who needed Extracorporeal Membrane Oxygenation (ECMO) therapy and pfHb was determined with HemoCue® plasma/Low Hb photometer. Pump thrombosis was analyzed macroscopically at the timing of pump explantation or exchange. Also, we divided the pump thrombosis into a grading scale by the place of thrombosis.
Results:
The median of peak pfHb was significantly lower in the none thrombus group (0.03 g/dL) than that of in the thrombus group (0.05g/dL) (p = 0.01). In our grading criteria, pfHb was significantly higher when the thrombus is existing near the shaft (p = 0.015). Contrary, no significant difference was found for LDH.
The ROC analysis of pfHb revealed an AUC of 0.77 for detecting pump thrombosis with the best statistical cutoff value at 0.05 g/dL (specificity, 78%; sensitivity, 77%). Also, ROC analysis of LDH was performed (AUC, 0.44; cutoff value, 1200 IU/L; specificity, 59%; sensitivity, 54%) and compared with pfHb. AUC was significantly higher in pfHb (p = 0.04).
Conclusion:
Our results showed the efficacy of pfHb for detecting centrifugal pump thrombosis.
Introduction
Pump thrombosis is one of the most critical conditions in Extracorporeal Membrane Oxygenation (ECMO) therapy with a centrifugal pump. Pump thrombosis can cause several complications such as cerebral infarction, hemolysis, and mechanical failure of the pump. Therefore, early diagnosis for pump thrombosis is the key to appropriate timing to perform pump exchange.
Three major indicators for the detection of pump thrombosis is clinically used. 1 Those are the presence of hemolysis (diagnosed by lactate dehydrogenase (LDH) greater than three times the upper limit of normal; generally 600–700 IU/L), worsening heart failure, and abnormal pump parameters. Two of the three indicators included above should raise concern for thrombus.
However, we often have difficulties with the diagnosis of hemolysis, especially in a patient under hemodynamic instability. Because their laboratory data is influenced by multiple organ damage. Usually, the LDH level is elevated before the initiation of a centrifugal pump, and the baseline of elevated LDH is considerably different in each patient. Therefore, we can not simply compare baseline levels of LDH to detect pump thrombosis when LDH is elevated.
In addition, LDH exists not only at RBCs, but it also exists widely at heart muscles and skeletal muscles. As a result, low tissue specificity of LDH makes it difficult to diagnose hemolysis. Plasma free hemoglobin (pfHb) is a diagnostic method of hemolysis that has high specificity.2,3 We used HemoCue® plasma/Low Hb photometer (HemoCue Corp, Ängelholm, Sweden) to try to diagnose hemolysis which is caused by pump thrombosis.
Methods
Patients
Between August 2017 and June 2019, 64 patients underwent ECMO therapy with a centrifugal pump at our facility. We excluded 33 cases of pump time less than 24 hours because it included cases that could not maintain target pump flow due to several reasons such as major bleeding and sepsis.
We enrolled 31 consecutive patients who needed ECMO therapy for more than 24 hours. (Table 1) The number of V-A ECMO, V-V ECMO, V-A + V-V ECMO was 24, 3, 4, respectively. Patients consisted of 25 men and six women, with a mean age of 63.4 ± 12.3 years old. Acute coronary syndrome was the most common indications for ECMO therapy (55%).
Patient characteristics.
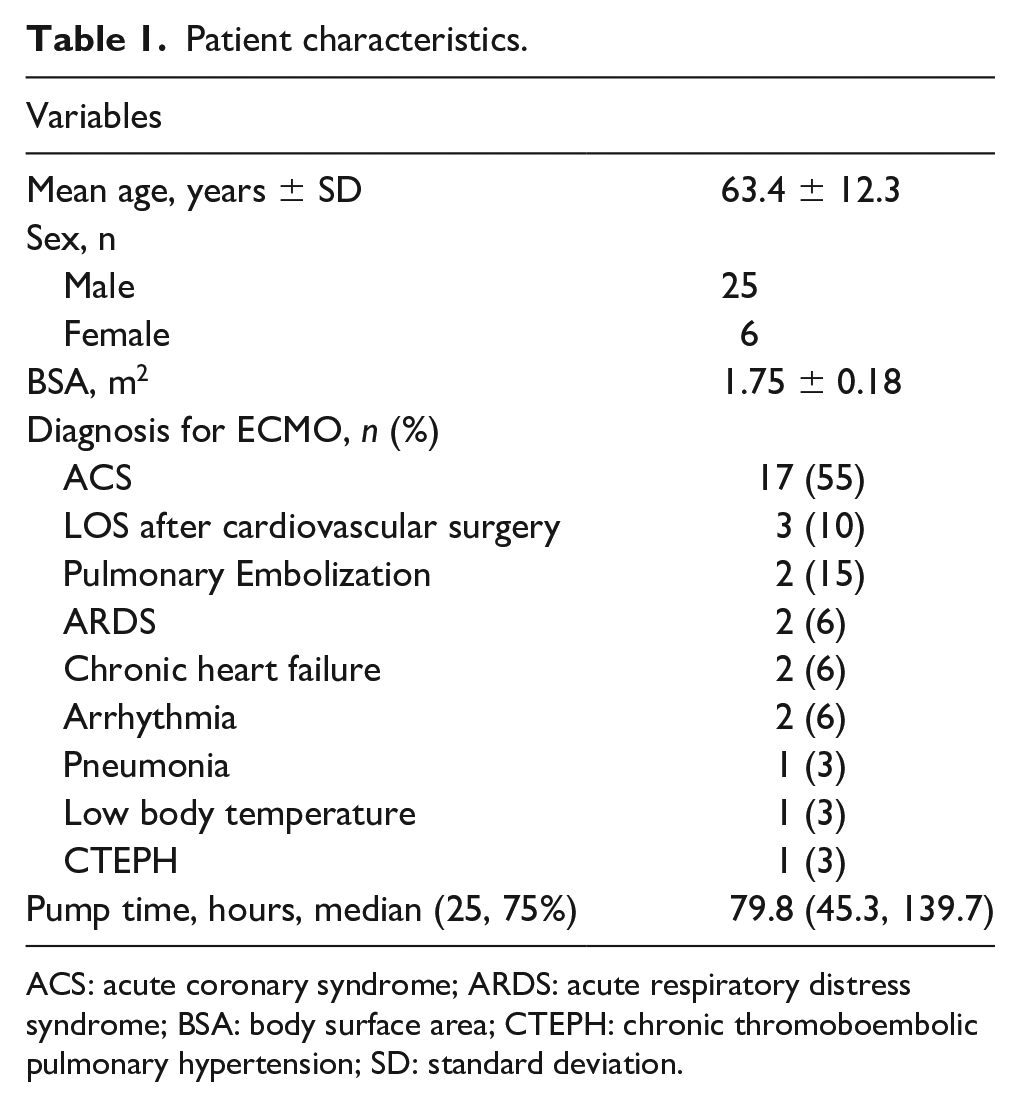
ACS: acute coronary syndrome; ARDS: acute respiratory distress syndrome; BSA: body surface area; CTEPH: chronic thromoboembolic pulmonary hypertension; SD: standard deviation.
Centrifugal pump devices and anticoagulation therapy
In all cases, we used Capiox CX-SL45X centrifugal pump (Terumo Corp, Tokyo, Japan). Target pump flow was 3.5 L/min in both veno-venous (V-V), veno-arterial (V-A) ECMO, and the median pump support time was 79.8 (45.3–139.7) hours. Continuous intravenous injection of naphamostat mesylate or heparin was administered for anticoagulation therapy. Naphamostat mesylate was administered in 16 cases, heparin was applied in one case, and both were applied in 14 cases. Active clotting time was maintained between 180 to 200 seconds. The timing for ECMO explantation was entrusted to each physician without criteria.
Study protocol
After the initiation of ECMO, blood samples were collected every 12 hours. We measured pfHb in the ICU. LDH was measured in the central clinical laboratory every morning at approximately the same time to pfHb check. Also, we inspected thrombus in the centrifugal pump and ECMO circuit including membrane oxygenator. Taken together, we evaluated the ability to diagnose pump thrombosis by pfHb and compared to LDH.
Detection of pump thrombosis
Pump exchanges were performed as soon as possible with the following criteria. First, it was performed within every 7 to 10 days even there is no trouble. Second, pfHb greater than 0.05 g/dL was observed. Third, the pressure drop at the membrane oxygenator was increased. Regarding the pressure drop, we referenced the normal value from the catalog by the pump manufacturer. We did not use precise cutoff.
As a result, 20 patients were able to explant ECMO and six pump exchanges were performed. ECMO support was withdrawn in 11 patients due to critical conditions such as irreversible low output syndrome, sepsis, and brain death. Pump thrombosis was examined macroscopically when the centrifugal pump was exchanged or removed. Circuits of non-survivors were also examined immediately.
Also, we divided the pump thrombosis into three grades by the place where thrombus existed. We named thrombus at shaft and shaft sleeve “Grade-2.” Thrombus anywhere in the pump housing except among shaft was “Grade-1.” No thrombus at all in the pump is “Grade-0”. (Figure 1) Grade-0 also included cases that have thrombosis in the membrane oxygenator.
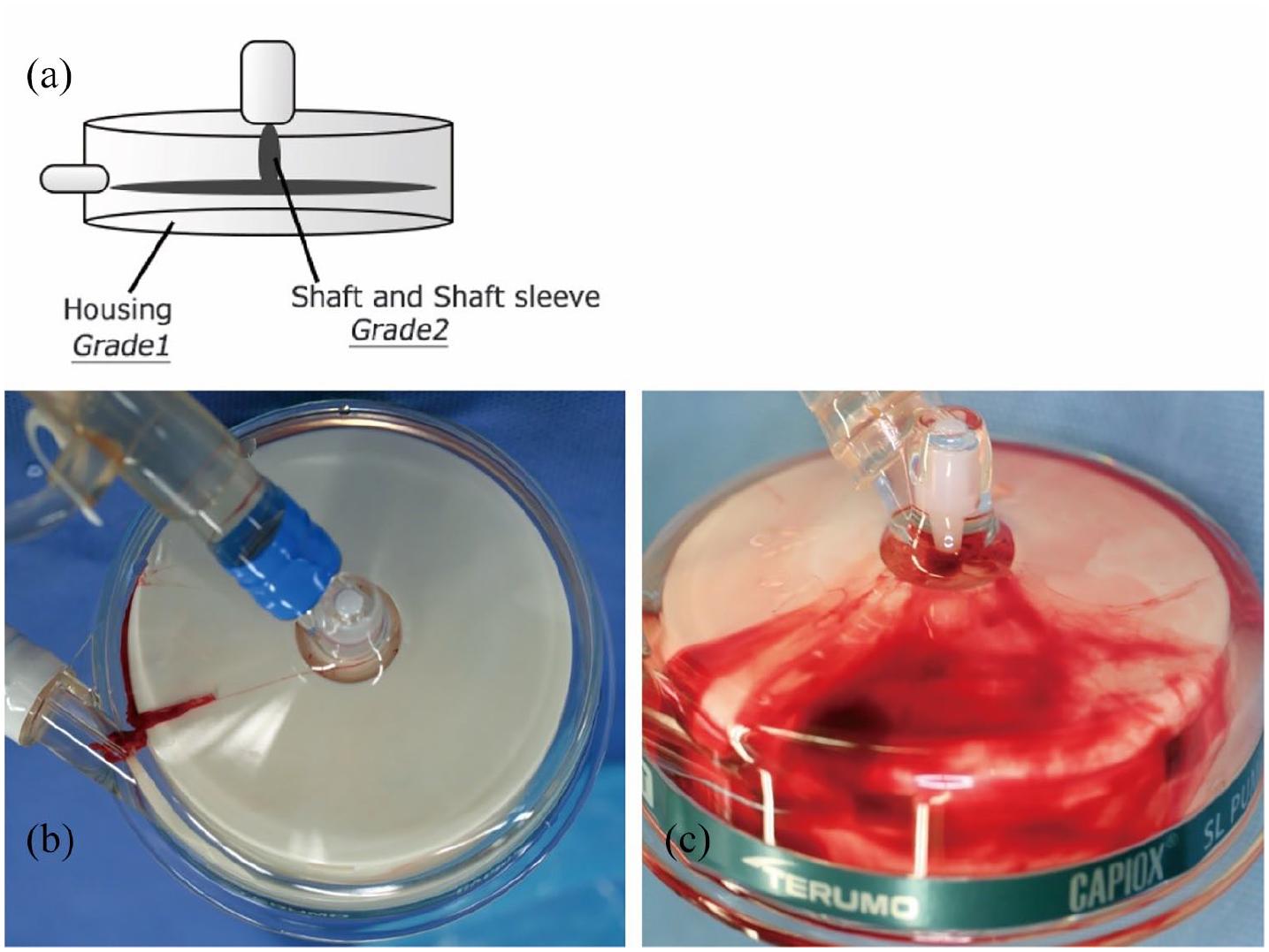
(a) Thrombus grade. Thrombus was divided into three grades. Grade-0 none thrombus, Grade-1 thrombus in anywhere in housing except shaft and shaft sleeve, Grade-2 thrombus at shaft and shaft sleeve. (b) Grade-1 thrombus. (c) Grade-2 thrombus.
Measurement of plasma free Hb
Blood samples were dispensed to a 0.8 ml microcentrifuge tube using a micropipette immediately. Centrifugation was performed at 3000 rpm over 30 minutes. When centrifugal separation was finished, plasma was sent to HemoCue® plasma/Low Hb photometer (HemoCue Corp, Ängelholm, Sweden) and measured pfHb. This device consists of a photometer together with the microcuvettes. A sample of approximately 20 microL is drawn into the cavity by capillary action. The photometer measures at two wavelengths in order to compensate for a certain degree of turbidity, and the hemoglobin level is calculated and presented.
All processes of the examination were finished in the ICU.
Measurement of LDH
Blood samples were sent to the central clinical laboratory. Centrifugation was performed at 3000 rpm, 7 minutes. When centrifugal separation was finished, automatic sample processor IDS-CLAS 2800 (IDS Co. Ltd., Kumamoto, Japan) and clinical chemistry analyzer BioMajesty® JCA-8020G (JEOL Ltd., Tokyo, Japan) were used for analysis.
Statistical analysis
The values were expressed as mean ± standard deviation or median (interquartile range). Their differences were assessed by one-way analysis of variance (ANOVA), Mann-Whitney U test, and Pearson’s chi-squared test. For significant interactions, the Bonferroni post-test was performed. P-value of less than 0.05 was considered statistically significant. The performance of pfHb and LDH were determined using receiver operating characteristic (ROC) curve analysis. Statistical analyses were processed using the software (EZR on R commander ver. 1.40, Tochigi, Japan). 4
Results
Thrombus was observed in 13 cases (41.9%). Patient characteristics in the none thrombus group and thrombus group are summarized in Table 2. The normal value of pfHb is less than 0.01 g/dL in our facility.
Patient characteristics in each grade.
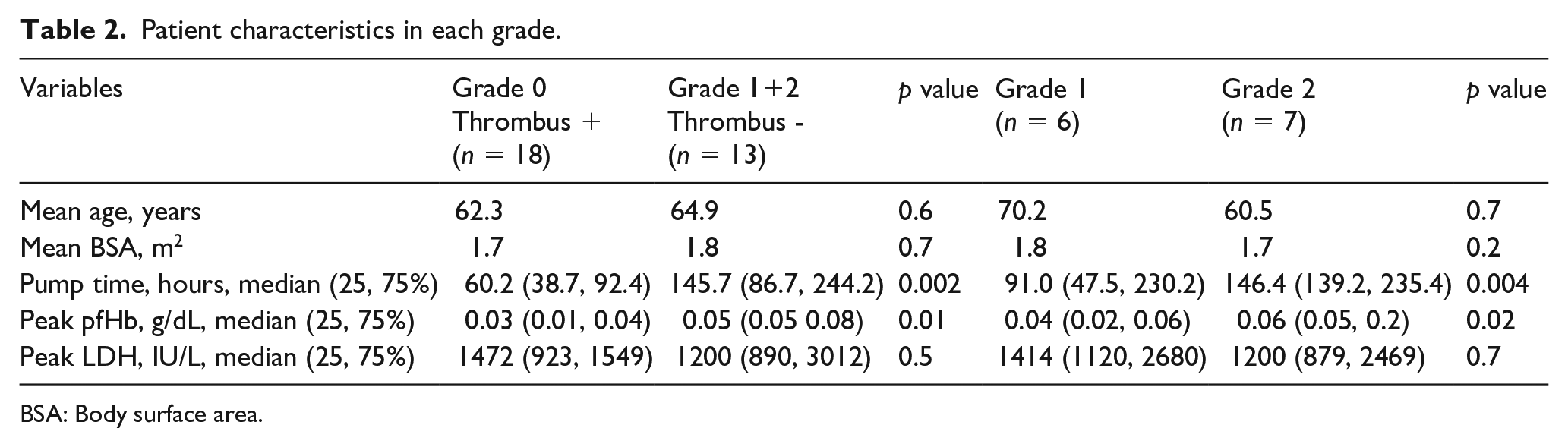
BSA: Body surface area.
The median of pump time in the none thrombus group (60.2 hours) was significantly shorter than that of the thrombus group (145.7 hours) (p = 0.002). Also, the median of peak pfHb was significantly lower in the none thrombus group (0.03 g/dL) than that of in the thrombus group (0.05g/dL) (p = 0.01). Conversely, the median of LDH did not show significant differences between groups (p = 0.5).
Furthermore, in our grading criteria, the median of pump time was 60.2 hours, 91.0 hours, and 146.4 hours in grade-0, grade-1, grade-2, respectively (p = 0.004). A significant difference was found between grade-0 and grade-2 by post hoc test (p = 0.004). Median of peak pfHb was 0.03 g/dL, 0.04 g/dl, and 0.06 g/dL for each grade (p = 0.02), respectively. Post hoc test showed significant differences between grade-0 and grade-2 (p = 0.015). There was no correlation between the grade of thrombus and survival (p = 0.7). Median of peak LDH was 1472 IU/L, 1414 IU/L, and 1200 IU/L for grade-0, grade-1, and Grade-2 (p = 0.7). There were no significant differences among groups.
Figure 2 shows the progression of increasing pfHb over time in each grade. This line graph reveals that a sharp increasing spike of pfHb reaches 0.05 g/dL is observed especially in grade-2.
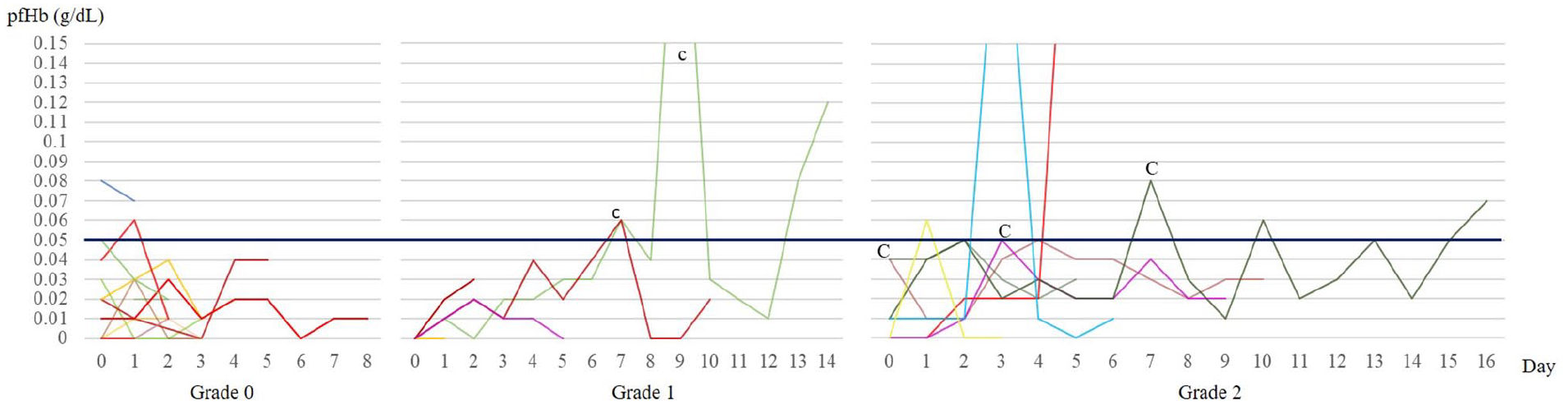
Progression of increasing pfHb over time in each grade of thrombosis. C; pump exchange.
The ROC analysis of pfHb revealed an AUC of 0.77 for detecting pump thrombosis with the best statistical cutoff value at 0.05 g/dL (specificity, 78%; sensitivity, 77%). Also, ROC analysis of LDH was performed (AUC, 0.44; cutoff value, 1200 IU/L; specificity, 59%; sensitivity, 54%) (Figure 3), and compared with pfHb. AUC was higher in pfHb (Figure 4).
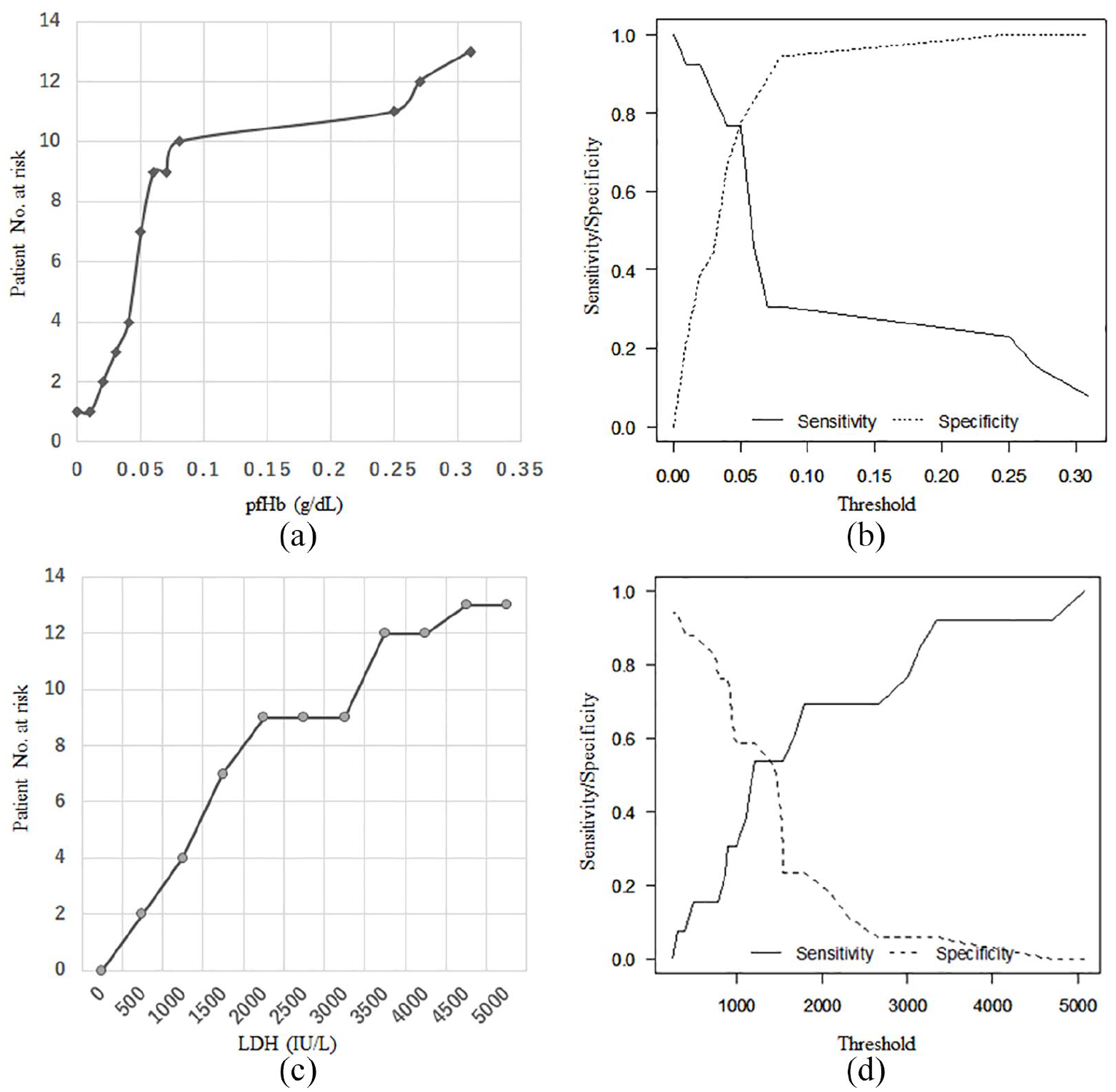
(a) Cumulative number of patient with pump thrombosis in pfHb. (b) Threshold of pfHb. The best statistical cutoff value at pfHb 0.05 g/dL. (c) Cumulative number of patient with pump thrombosis in LDH. (d) Threshold of LDH. The best statistical cutoff value at LDH 1200 IU/L.
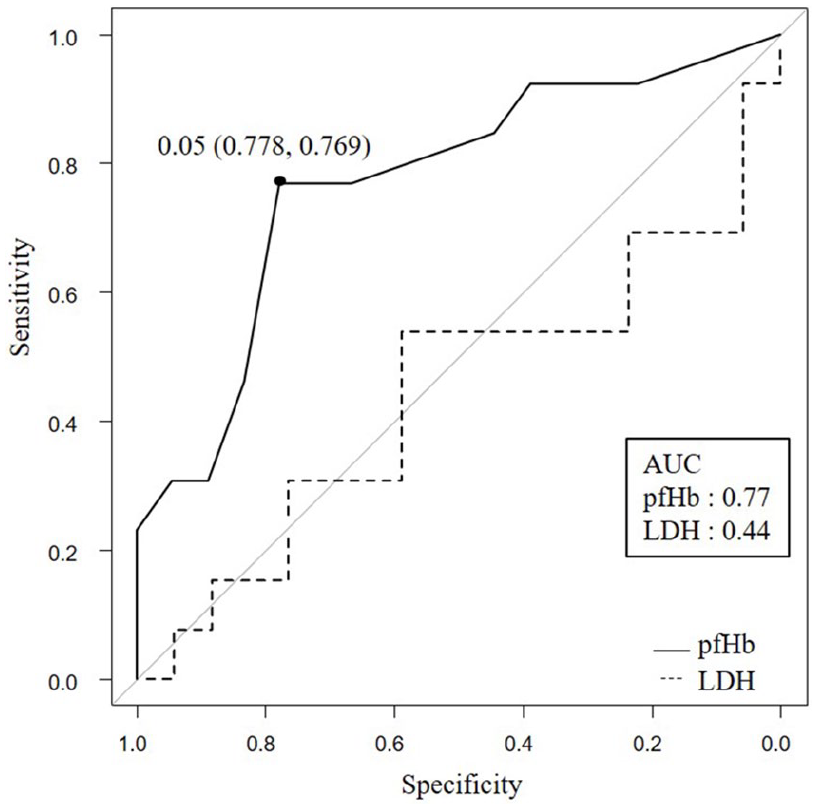
Receiver Operatorating Characteristic curve (ROC) of pfHb and LDH.
Discussion
In this study, we have shown that quick routine measurement of pfHb using HemoCue® plasma/Low Hb photometer will help to diagnose pump thrombosis. Also, this device maintains not only rapidity but simplicity because we can place the device near the bedside and get data within 40 minutes. Examiners will easily to re-examine if they observe the abnormal value in midnight. In addition, the measurement of pfHb is no longer entrusted in the central clinical laboratory at our facility or outsourcing company in Japan.
We observed pump thrombosis in 41% cases and it appears higher than the past report. The reported incidence was between 5% and 18%. 5 One explanation for that would be our grading criteria which were examined macroscopically and the time to check was not uniform. It would bring about an increase of grade-1 thrombus.
Comparing pfHb with LDH, ROC analysis revealed that pfHb is an examination with high specificity for diagnosing hemolysis. Furthermore, in the severe hemolysis case, pfHb measured by HemoCue® plasma/Low Hb photometer is an effective indicator for detecting pump thrombosis in the acute phase of ECMO therapy.
On the contrary, LDH had lower sensitivity and specificity in our study. The reason for our result, we assume that the indication of ECMO therapy had interferences in our results. Our data showed LDH greater than three times the upper limit of normal in the none thrombus group. Elevation of LDH was influenced by acute coronary syndrome which was the most common indication for ECMO. Furthermore, there is a possibility to obtain distinct results in the long support case.
With regards to the cutoff value of pfHb, Goldstein et al. reported that pfHb greater than 40 mg/dL should be a concern for possible thrombus. 6 Also, Extracorporeal life support Organization (ELSO) established the cutoff value of pfHb greater than 0.05 g/dL.7,8 Our results are similar to their data. Furthermore, as Neal et al. 2 suggested, a rapid spike of pfHb is also important. Our data indicate that a rapid spike of pfHb reaches up to 0.05 g/dL is an important predictor of pump thrombosis.
The accuracy of HemoCue® plasma/Low Hb photometer was shown by Morris et al. They revealed it’s reliability for quantifying plasma hemoglobin. 9 Furthermore, hyperbilirubinemia has the possibility to interfere with the data because this device quantifies pfHb by spectrometry. Morris et al. also reported there was no consistent trend identified between pfHb and total bilirubin. 10 Moreover, the use of bilirubin oxidase can eliminate the interference of hyperbilirubinemia. 11 Besides, bilirubin has accumulative properties, so it will not be a problem in the acute phase.
Limitations of the study
This study has several limitations. First, we checked thrombus macroscopically when the pump was removed, therefore, the time to check thrombus was not uniform. Second, we used the same types of centrifugal pumps in all cases. Pump characteristics and the shape of the device might influence the level of hemolysis. 12 Accordingly, the cut off value of peak pfHb with other kinds of pumps is still unknown. Third, our study was a small study with heterogeneous patients.
Conclusion
Our results showed the efficacy of routinely measured pfHb for detecting centrifugal pump thrombosis, especially in the acute phase of therapy. Also, our result indicates that our pfHb measurement using HemoCue® plasma/Low Hb photometer is an effective solution for detecting pump thrombosis. However, our study was in a relatively small set of heterogeneous patients. A further prospective study is required to solidify HemoCue as a tool for detection.
Footnotes
Correction 2025:
Article amended to include a second affiliation for author Taiyo Kuroda.
Authors’ Contributions
All authors participated in drafting and reviewing. All authors read and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.