
Abstract

The cardiopulmonary bypass (CPB) recently received some technological developments in particular in terms of biocompatibility but it maintains some intrinsic limitations such as the inflammatory response, the coagulation alterations, the temporary dysfunction of the microcirculation, and the transient “suffering” of the metabolism of tissues and organs. 1 A component of the “conventional” extracorporeal circulation is the venous reservoir. It is usually a rigid container used to collect and “manage” venous blood from the right heart sections and equipped with filters to eliminate gaseous and lipid embolisms. The visualization of the volume and the “level” in the venous reservoir is essential to manage the administration of fluids, deliver an adequate cardiac output and guarantee a bloodless and relaxed heart during cardiac surgery procedures. The venous reservoir in the conventional CPB is essential but, being an open system to atmospheric air, it involves an “air-blood” contact interface. We assumed that the administration of ozone in the venous reservoir could limit the concentration of nitrogen, which would normally be 78% of the air, in direct contact with the blood surface (Figure 1). The ozone therapy (O3) is burdened with some serious side effects, nevertheless it has been extensively applied and studied; in particular the O3 therapy is believed to be effective in treating the heart failure and orthopedic problems.2–4 O3 is characterized by a strong oxidizing power, by a higher solubility in the blood than that of oxygen and is able to supply energy and oxygen to damaged tissues. 5 Some studies have shown that O3 improves the ischemia of the injured tissues through the release of oxygen to the tissues themselves, the activation of the pentose phosphate pathway, the elevation of the 2,3-DPG content in the erythrocytes and the stimulation of the erythrocyte oxygen metabolism. 5 In addition, O3 can also protect blood cells from oxidative stress by inducing the expression of antioxidant enzymes.4,6 Ozonated autohemotherapy (Ozone-AHT) was initially applied in clinical practice in 1968 and is now widely used in various clinical disciplines, particularly for the treatment of systemic diseases on an ischemic basis.7–9 This bibliographic base for the treatment of systemic and ischemic diseases, has made us hypothesize that the Ozone-AHT applied in the venous reservoir, in addition to the component of O3 itself which dissolves in the blood, can create a protective gaseous layer that blocks the contact between the blood surface and air.
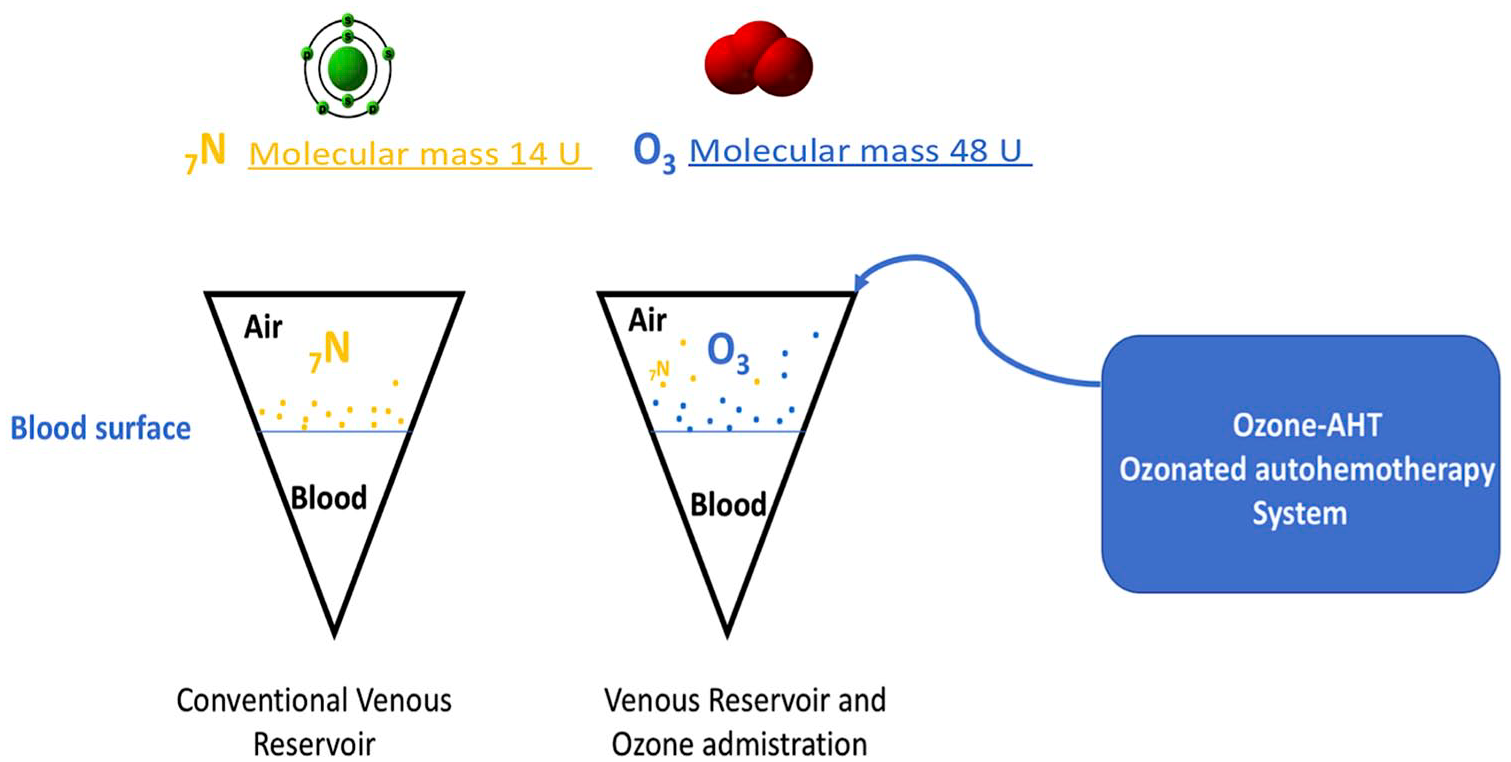
The administration of ozone in the venous reserve could limit the concentration of nitrogen, which would normally be 78% of the air, in direct contact with the blood surface.
The use of gases present in the atmosphere at low concentrations is very common in cardiac surgery, as in the case of carbon dioxide (CO2). The latter, because of its high solubility with respect to oxygen and the higher molecular weight, is used in the operating field to prevent gas embolism caused by nitrogen in the air. However, carbon dioxide brings with it inflammatory effects and changes in the blood corpuscular components. However, its role in the prevention of cerebrovascular events of an embolic nature makes its use essential. Ozone has a molecular weight of 48 U greater than carbon dioxide which has a weight of 44 U. 10 This molecular weight supports our hypothesis of ozone’s ability to contain the inflammatory response caused by the contact between nitrogen and blood in the venous reservoir of the open circuits.
A study was conducted by Deng et al. and aimed to study the effect of ozone on hypoxia, hemolysis, and morphological changes of blood from patients with aortic dissection to provide preliminary evidence of the application of Ozone-AHT in this type of patients. These authors concluded that ozone improves oxygen content and reduces oxidative damage in the blood of patients with aortic dissection and the therapeutic dose of ozone does not induce hemolysis and morphological changes of the erythrocytes. 5 However, we have to highlight that the publication from Deng et al. is a in-vitro study; suggesting the need of an in-vivo examination.
So, in conclusion, we believe that the application of ozone in the airspace of the venous reserve with its increase in molecular concentration compared to nitrogen could reduce inflammation from “air-blood” contact with consequent benefits in terms of reducing the inflammatory response. Our hypothesis is a new field of study which must be developed and accompanied by an experimental use of ozone in the Reservoir with analysis of its effect in clinical and laboratory terms.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.