
Abstract
Introduction:
Intraoperative cardiac arrest (ICA) is a feared complication during liver transplantation (LTx), typically occurring during reperfusion. Veno-arterial extracorporeal membrane oxygenation (VA-ECMO) has been used for post-reperfusion cardiac arrest.
Case report:
We present a case of successful resuscitation after hyperkalemic ICA during the pre-anhepatic phase of a second liver transplantation by converting veno-venous bypass (VVB) to VA-ECMO.
Discussion:
While this technique has been recommended for ICA during reperfusion, it has never been reported during the pre-anhepatic phase. VA-ECMO can be a lifesaving extension to cardiopulmonary resuscitation for ICA during LTx with beneficial neurological outcome by providing perfusion while the cause of ICA is reversed.
Conclusion:
Conversion of VVB to VA-ECMO should be considered in all patients who suffer from ICA during LTx with use of VVB. With VVB installed, conversion to VA-ECMO is fast and effective. If VVB is not used, early VA-ECMO should be considered for ICA.
Keywords
Introduction
Intraoperative cardiac arrest (ICA) is a feared complication occurring in up to 5.5% of liver transplantations (LTx) with a mortality of 12% to 29.4%.1–4 ICA during LTx is typically a dramatic manifestation of post-reperfusion syndrome in which electrolyte and metabolic disturbances (hyperkalemia, acidosis), hypovolemia and vasoplegia are implicated.1,2 Veno-arterial extracorporeal membrane oxygenation (VA-ECMO) has been used for refractory post-reperfusion cardiac arrest. 3 We present the first reported case of successful resuscitation, prior to reperfusion, with conversion of veno-venous bypass (VVB) to VA-ECMO.
Case report
A 34-year old patient underwent a second LTx, with use of VVB, for decompensated cirrhosis due to ischemic cholangiopathy. She had a history of hepatico-jejunostomy at the age of 2 for extrahepatic biliary atresia followed by LTx 2 years later. Her general condition was very poor, renal function moderately reduced and echocardiography normal.
Due to continuous oozing, related to severe coagulopathy, 3 units of packed cells were transfused during the dissection phase. VVB was installed by cannulating the portal vein (28 Fr. DLP® Single-Stage, Medtronic, USA), right femoral vein (20 Fr. DLP® Single-Stage) and left axillary vein (15 Fr. Bio-Medicus®, Medtronic) with the latter as outflow. Satisfactory flow was not achieved.
Before hepatectomy completion, ICA with sudden asystole occurred. Chest compressions were initiated and immediately effective. Blood gas indicated a potassium of 10.5 mmol/l and hemoglobin of 10.4 mg/dl, shown in Figure 1. With the differential diagnosis of hyperkalemic cardiac arrest, adrenalin, vasopressin, bicarbonate, insulin, and calcium were administered. After 18 minutes of cardiopulmonary resuscitation (CPR), return of spontaneous circulation occurred. During hepatectomy completion with ongoing bleeding, three units of packed cells were given. Cardiac arrest with asystole reoccurred, blood gas showed a potassium of 9.7 mmol/l and hemoglobin of 3.1 mg/dl. Chest compressions were restarted and transfusion was initiated.
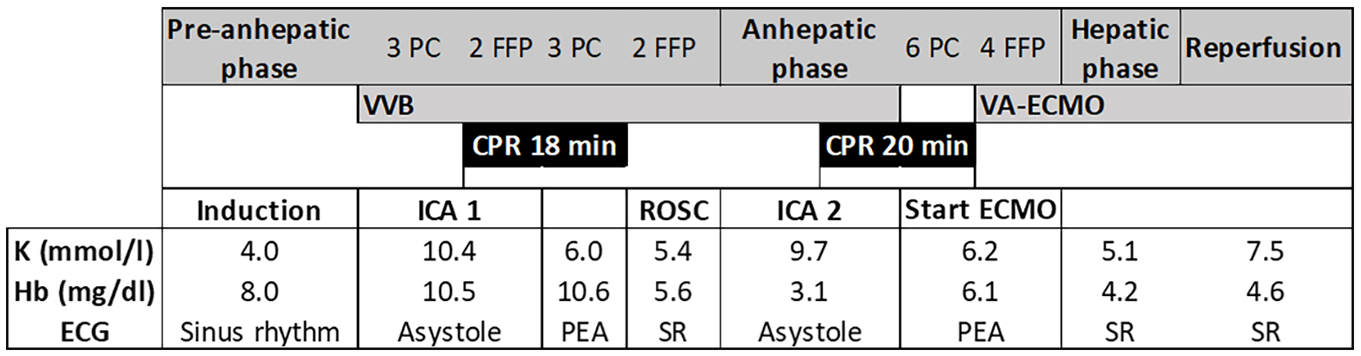
Schematic illustration of the sequence of events during LTx.
As veno-arterial ECMO was deemed the only option, the VVB setup was converted by the transplant surgeon. An outflow cannula was placed in the right femoral artery via cut-down (19 Fr Bio-Medicus®) and the femoral venous cannula was exchanged for a larger one (23 Fr. HLS, Maquet, USA). The portal inflow cannula remained while the axillary cannula was clamped. Tubing was exchanged between the Bio-Medicus 550 Centrifugal pump (Medtronic) and a Medos Deltastream® MDC ECMO system (Xenios AG, Germany), primed with 600 ml cristalloids. After 20 minutes of CPR, VA-ECMO was initiated with rapid stabilization of hemodynamics. By this time, 6 more units of packed cells had been given, hemoglobin had increased to 6.1 mg/dl and potassium decreased to 6.2 mmol/l.
During LTx completion, spontaneous sinus rhythm returned and the patient remained hemodynamically stable. Reperfusion was uneventful. After the abdomen was closed, the patient was weaned from ECMO smoothly and a pre-emptive kidney transplantation was performed in the left iliac fossa. During the entire procedure, 23 units of packed cells, 31 units of plasma and 4 units of platelets were given.
The ICU stay was largely uneventful yet post-anoxemic optic neuropathy was diagnosed due to rightsided blindness. Explant liver histopathology confirmed biliary cirrhosis. After an uncomplicated hospitalization, she was discharged 64 days post-LTx. She is now 40 months post-transplant, doing well with normal hepatic, renal and cardiac function. She provided informed consent regarding use of her data.
Discussion
We present a case of hyperkalemic cardiac arrest during a second liver transplantation. Conversion from VVB to VA-ECMO was a lifesaving measure by maintaining stable hemodynamics while the cause of ICA was reversed and LTx completed.
Both episodes of hyperkalemic ICA were likely multifactorial in origin: preexisting renal dysfunction, extensive liver manipulation, continuous bleeding, hypovolemia and transfusion of multiple potassium-rich units of red blood cells.1,5,6 Treatment of hyperkalemic arrest consists of adrenalin, insulin, glucose, calcium and bicarbonate. 7 While not applied here, a transdiaphragmatic pericardial window for cardiac compressions is advocated in refractory resuscitation during LTx. This avoids rib fractures while enabling internal defibrillation and chest drain placement.1–4
VA-ECMO provides a survival benefit in patients requiring more than 10 minutes of CPR yet survival is poor if initiated after more than 30 minutes.8,9 In our case, ECMO was initiated after a total of 38 minutes of CPR with a postoperative Cerebral Performance Category score of 1 nonetheless. 10 In emergency settings, timely availability of ECMO may be problematic.3,4 With VVB installed and due to the urgency, the abdominal transplant surgeon performed the conversion to VA-ECMO, under guidance of the perfusionist, using a previously described technique. 3 We consider this an argument in favor of VVB in high-risk patients with a greater risk of developing ICA.
Additional recommended measures include transesophageal echocardiography to monitor cardiac function and aid in differential diagnosis.3,11 In our case, this was not performed due to esophageal varices, yet early weaning from ECMO was possible due to successful reversal of the cause of ICA with adequate cardiac output measured invasively.
Conclusion
Conversion from VVB to VA-ECMO has been described for the management of ICA during liver reperfusion. 3 We illustrated the conversion from VVB to VA-ECMO as a lifesaving extension to CPR for ICA prior to hepatectomy. VA-ECMO provides systemic perfusion, enables cardiac recovery and allows correction of reversible causes.3,4 We believe this effective technique, which can be performed rapidly and under guidance of the perfusionist, should be considered for all patients suffering from ICA during LTx with VVB. If VVB is not used, early VA-ECMO should be considered, further emphasizing the important role of perfusionists in liver transplantation centers.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: LVH is the holder of a predoctoral grant “Strategic basic research” (SB 1S70220N) from the Research Foundation Flanders (FWO).