
Abstract
Introduction
Acute intoxication (AI) related morbidity and mortality are increasing in the United States. For patients with severe respiratory failure in the setting of an acute ingestion, veno-venous extracorporeal membrane oxygenation (VV ECMO) can provide salvage therapy. The purpose of this study was to evaluate outcomes in patients with overdose-related need for VV ECMO.
Methods:
We performed a retrospective review of all patients admitted to a specialty VV ECMO unit between August 2014 and August 2018. Patients were stratified by those whose indication for VV ECMO was directly related to an acute ingestion (alcohol, illicit drug, or prescription drug overdose) and those with unrelated diagnoses. Demographics, pre-cannulation clinical characteristics, ECMO parameters, and outcomes data was collected and analyzed with parametric and non-parametric statistics as indicated.
Results:
189 patients were enrolled with 27 (14%) diagnosed with AI. Patients requiring VV ECMO for an AI were younger, had lower median BMI and PaO2/FiO2, and higher RESP scores than non-AI patients (p = 0.002, 0.01, 0.03 and 0.01). There was no difference in pre-cannulation pH, lactate, or SOFA scores between the two groups (p = 0.24, 0.5, 0.6). There was no difference in survival to discharge (p = 0.95). Among survivors, there was no difference in ECMO time or hospital stay (p = 0.24, 0.07).
Conclusion:
We demonstrate no survival difference for patients with and without an AI-related need for VV ECMO. AI patients should be supported with VV ECMO when traditional therapies fail despite potential stigma against acceptance on referral.
Introduction
The use of veno-venous extracorporeal membrane oxygenation (VV ECMO) is increasing as the technology and expertise to offer this potentially life-saving intervention becomes more common. 1 Indeed, even referral to an ECMO center is associated with improved outcomes in patients with respiratory failure refractory to conventional therapy. 2 However, guidelines concerning patient selection for this resource intensive therapy vary between institutions. While the utilization of veno-arterial ECMO for overdoses of cardiotoxic exposures is relatively well-established3–5 and has been found to be cost-effective, 6 VV ECMO utilization criteria for patients with respiratory failure following acute intoxication (AI) have not been assessed.
A retrospective study by Stoyle and colleagues demonstrated a small increase in the number of complications in patients with a history of drug or alcohol dependency on VV ECMO compared to those without a history of dependency. 7 While there was no statistical difference in rates of survival, there have been a number of case reports, which demonstrate the effective use of VV ECMO in patients with drug-related respiratory collapse. The etiology of the respiratory compromise is varied, including opioids, cocaine,8,9 and marijuana cigarettes laced with phencyclidine or formaldehyde. 10
A number of scoring systems exist which predict ECMO outcomes such as the Respiratory ECMO Survival Prediction (RESP) score 11 or Acute Physiology and Chronic Health Evaluation (APACHE) II score 12 to predict in-hospital mortality.13,14 However, these predictive models do not incorporate intoxication into their schema. The aim of this study was to evaluate outcomes of patients requiring VV ECMO for acute alcohol- or drug intoxication-related respiratory failure. We hypothesized that these patients would have comparable outcomes when compared to other VV ECMO patients.
Methods
Patients
A retrospective cohort study was performed of patients admitted to a dedicated, multi-disciplinary intensive care unit for patients on VV extracorporeal membrane oxygenation between August 2014 and August 2018. Trauma patients and those who were bridging to lung transplantation were excluded. Patients with a diagnosis of AI on presentation (alcohol, illicit drugs, or prescription pharmaceuticals) were compared to patients who had ARDS from another etiology. Demographic data, substance use history, pre-ECMO data, ECMO details, and patient outcomes were collected. The study was approved by the institutional review board at the University of Maryland, Baltimore, USA (IRB # HP-00091990).
Institutional ECMO practices
At our institution VV ECMO most commonly provided via two single-lumen catheters using a Rotaflow Centrifugal Pump System (MaquetTM Cardiopulmonary AG, Hirrlingen, Germany). Return cannulas are typically placed through a percutaneous right internal jugular approach and the drainage cannula is placed similarly in one of the common femoral veins (typically the right). Clinical practice for patients on VV ECMO at our institution has been standardized in effort to minimize variations in practice among providers. During the study period, anticoagulation with a heparin infusion was titrated to a partial thromboplastin time of 45 to 55 seconds to prevent clotting of the circuit. Once cannulated, a pressure-controlled ventilation strategy is implemented. Inspiratory pressure is set at 20 cm H2O with a positive end expiratory pressure of 10 cm H2O generating a driving pressure of 10 cm H2O. Prone positioning of patients is initiated at the discretion of the clinical team. Proned patients have their inspiratory pressure set at 25 cm H2O and positive end expiratory pressure set at 15 cm H2O. Flow on the ECMO circuit is titrated to maintain a SpO2 of greater 88%, while the sweep gas is titrated to maintain a patient pCO2 of 35 to 45 mmHg assuming no evidence of right heart dysfunction. Patients with evidence of right heart dysfunction on echocardiography have their pCO2 titrated to 35 to 40 mmHg along with inhaled prostacyclin and an infusion inotropic dose of epinephrine. A minimum hemoglobin threshold of 8 g/dL and platelet transfusion threshold of 40,000/µL is used assuming no active bleeding. Once patients have adequate oxygenation and ventilation parameters on minimal sweep a trial off ECMO support is attempted. Serial arterial blood gases are analyzed and if adequate patients are decannulated within 24 hours. Prior to transfer, most patients are paralyzed and initiated on an empiric broad spectrum antibiotic regimen.
Statistical analysis
Statistical analysis was performed using SAS 9.3 (SAS Corporation, Cary, NC, USA). Continuous variables were summarized as the median value and interquartile range and categorical values were summarized as the number and percentage of patients. Dichotomous outcomes were compared using either the Chi-Squared Test or Fisher’s Exact Test as appropriate.
Results
A total of 189 patients were supported with VV ECMO during the 4-year study period. Baseline demographic information can be found in the Table 1. Twenty-seven (14.3%) of these patients had ARDS related to AI with Table 2 describing the substances used. Additional substances included oral narcotics (Percocet and methadone), ecstasy, intranasal heroin, cocaine, marijuana, and an intentional overdose of calcium channel blocker. A few patients partook in multiple substances. The non-AI group did not have any significant history of drug or alcohol abuse. The most common etiologies of respiratory compromise and indication for VV ECMO in the intoxication group included aspiration pneumonitis (15, 55.6%) and bacterial pneumonia (9, 33.3%). A comparison between baseline characteristics for the two cohorts can be found in Table 3. When compared to patients cannulated for respiratory failure not associated with an acute ingestion, AI patients were younger, had lower BMI and a higher RESP score (p-values 0.002, 0.008, 0.01 respectively) at time of cannulation. They had similar pH, peak inspiratory pressures, and Sequential Organ Failure Assessment (SOFA) scores.
Demographics, pre-ECMO, ECMO and outcome (n = 189).
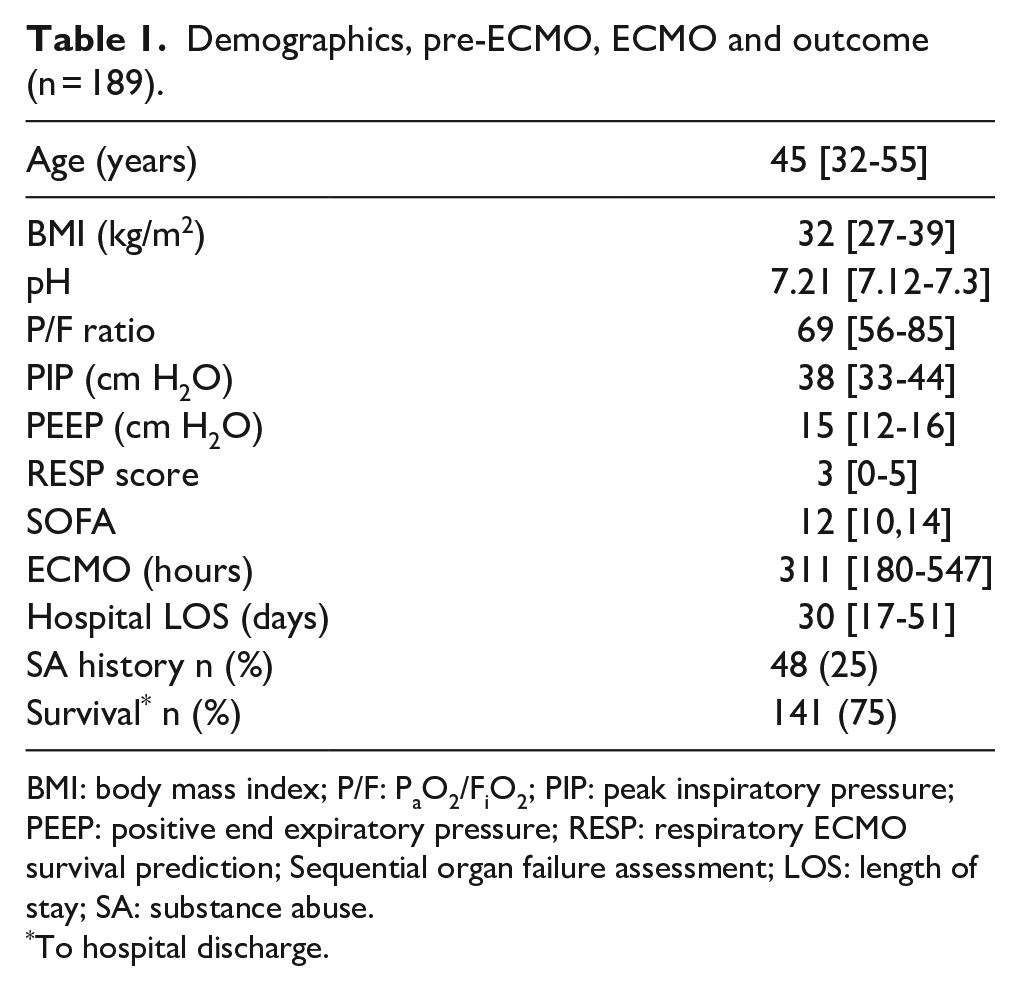
BMI: body mass index; P/F: PaO2/FiO2; PIP: peak inspiratory pressure; PEEP: positive end expiratory pressure; RESP: respiratory ECMO survival prediction; Sequential organ failure assessment; LOS: length of stay; SA: substance abuse.
To hospital discharge.
Types of acute ingestions (n = 27).
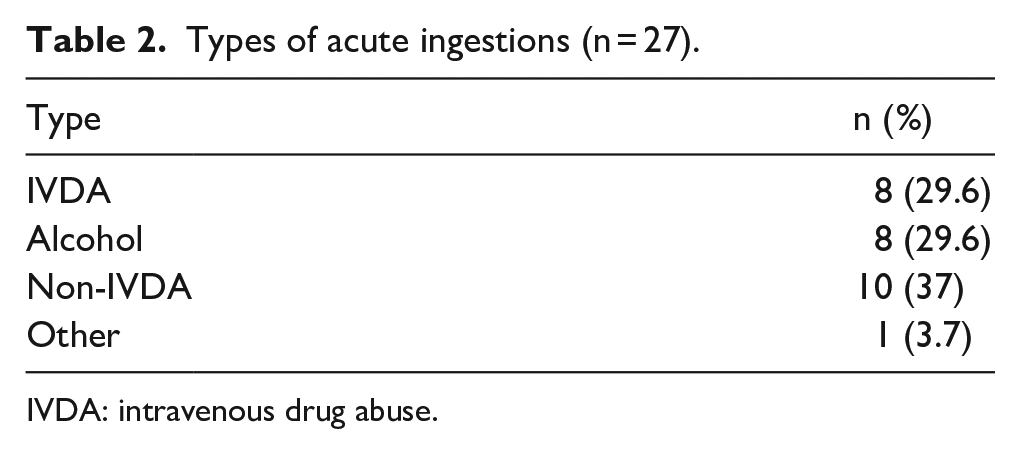
IVDA: intravenous drug abuse.
Comparison acute ingestion (AI) versus no acute ingestion.
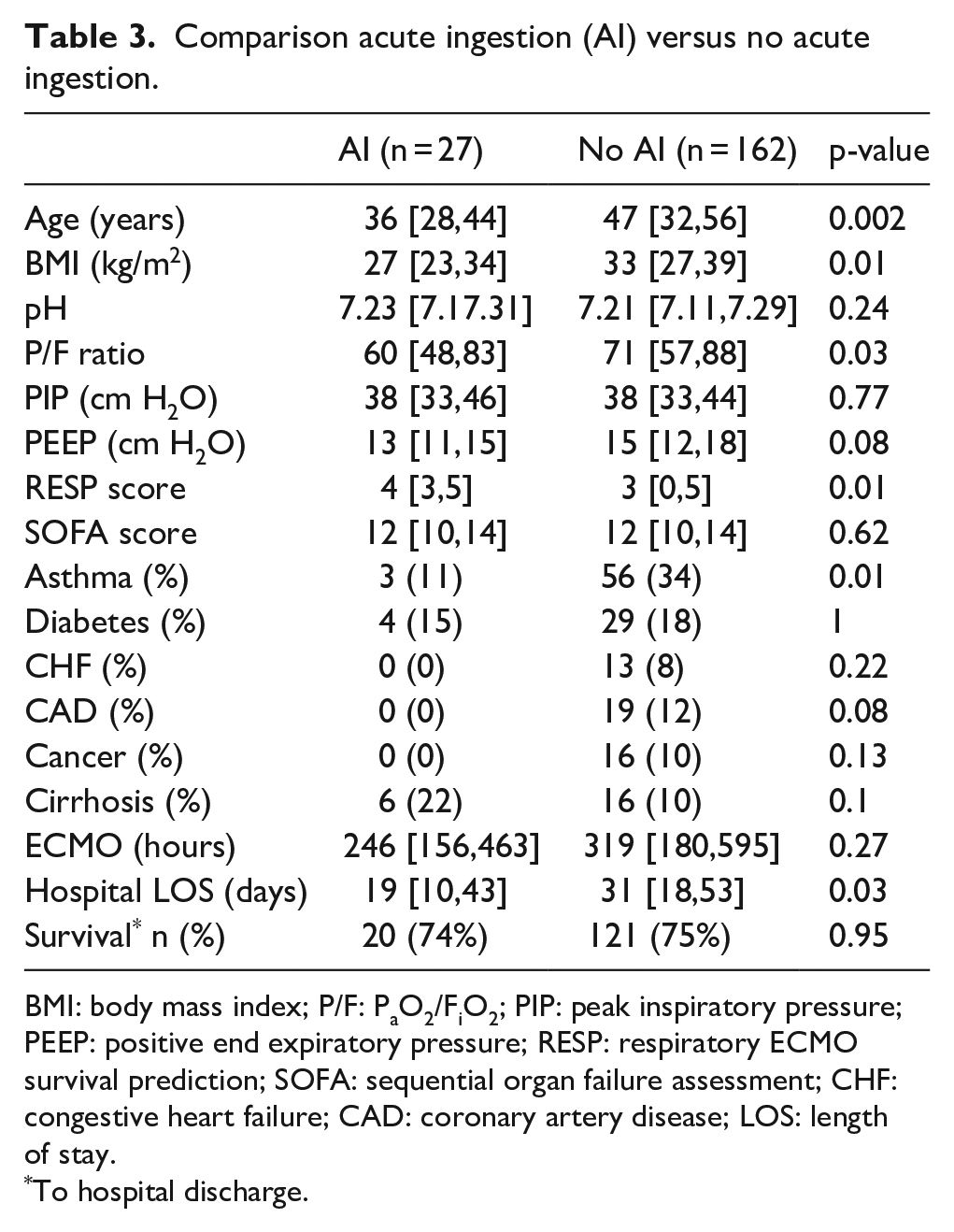
BMI: body mass index; P/F: PaO2/FiO2; PIP: peak inspiratory pressure; PEEP: positive end expiratory pressure; RESP: respiratory ECMO survival prediction; SOFA: sequential organ failure assessment; CHF: congestive heart failure; CAD: coronary artery disease; LOS: length of stay.
To hospital discharge.
The AI cohort had 11 patients (39.3%) placed on continuous renal replacement therapy (CRRT). Four (36.3%) of these patients survived and none of these individuals required dialysis on discharge. Of the 162 non-intoxication patients, 85 (52.8%) were placed on CRRT with 55 (64.7%) surviving and 4 of them requiring dialysis on discharge. While there was a statistically significant difference in AI patient survival depending on CRRT use (p = 0.002), this was not true for the non-AI cohort, and indeed there was no difference in overall CRRT use between the two groups.
Twenty (74.1%) of the AI patients survived to hospital discharge. Half were transferred to rehabilitation facilities and the remainder discharged directly home. This is similar to the rehabilitation facility discharge disposition rates of the non-intoxication cohort (70%, p = 0.51). Three AI survivors subsequently died following discharge at 46, 78, and 229 days following decannulation; one succumbed to another overdose. The duration of ECMO was similar between intoxication patients and non-intoxication patients, but the intoxication cohort had a shorter hospital stay (19 vs. 31 days, p = 0.027). When only survivors were considered in both cohorts, the median length of stay was similar (30 vs. 32 days).
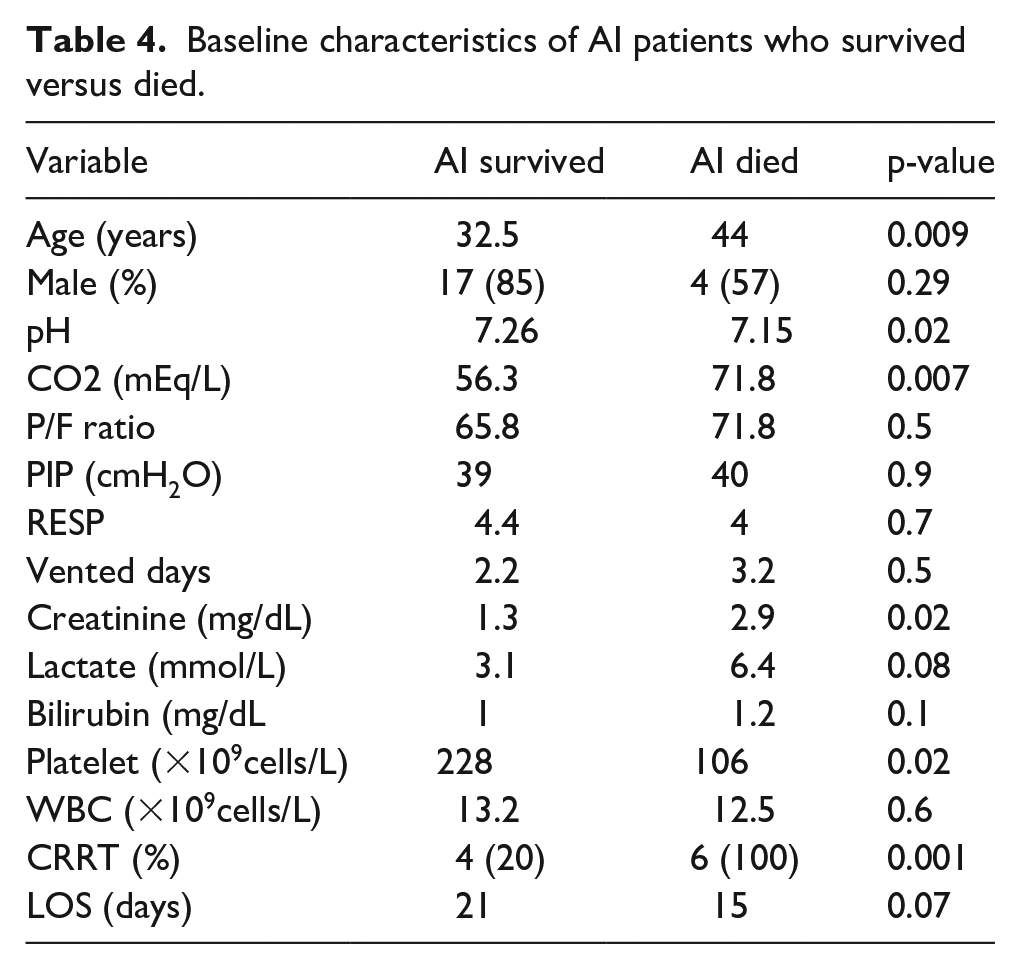
Table 4 describes the differences between those AI patients on VV ECMO who survived and those AI patients who died. Survivors were generally younger (32.9 vs. 46.3 years, p = 0.009), had higher pre-cannulation pH (7.26 vs. 7.15, p = 0.02), lower preECMO CO2 (56.3 mmHg vs. 71.8 mmHg, p = 0.007), lower serum creatinine (1.32 mg/dL vs. 2.88 mg/dL, p = 0.02) and higher platelet levels (227×103/µL vs. 106×103/µL, p = 0.02. Unlike the differences between the AI and non-AI cohort, AI survivors had a similar RESP score to those AI patients who died.
Baseline characteristics of AI patients who survived versus died.
Discussion
This study represents a large cohort of patients requiring VV ECMO for respiratory failure following acute intoxication. Prior investigations involving drug and alcohol dependent patients on VV ECMO did not specify that the inciting underlying diagnosis be the result of an acute intoxication, rather that the patients have an ongoing history of substance use. 7 Similar to our baseline statistics, their drug-dependent group had a lower weight than their non-drug-dependent matched cohort. However, the duration of ECMO was increased by almost 2 days in that drug-dependent cohort, which stands in contrast to our findings.
The main findings in our study were that despite worse pre-ECMO lung injury based on P/F ratio and RESP scores, there was no statistically significant difference in survival to hospital discharge or ECMO duration between intoxication patients and non-intoxication patients. Given that the AI cohort consisted of younger patients, it is conceivable that the lower P/f ratios in AI patients represents a more robust immunologic response to the initial insult, resulting in increased pulmonary inflammation compared to the non-AI group. However, P/f ratios are not necessarily reflective of ECMO outcomes and are not included in prognostic metrics. 15 This suggests that AI should not be an absolute contraindication for VV ECMO therapy for patients who have respiratory failure refractory to conventional therapies. However, within the AI cohort, mortality was associated with older age, hypercapnia, and worsening renal function at the time of cannulation.
Our study findings of similar mortality despite worse RESP scores could be related to differences in baseline demographic variables and comorbidities between intoxication patients and non-intoxication patients. Patients with AI were younger by an average of a decade and had a significantly lower BMI, although this latter variable may not predict as significant a prognostic influence as had been previously thought.16–18 While the age difference is statistically significant, they would both receive a “0” score on the RESP scale and 47 is just 2 years over the cutoff for the youngest cohort in the PRESERVE scale. Thus, this may be statistically, but not clinically significant.
Additionally, the intoxication event often led to aspiration pneumonitis which portends a better outcome with rapid recovery if able to endure the initial insult. This may be reflected in the significant difference in the RESP scores (4 vs. 3) between the two groups. Still, these patients had mortality rates similar to the predicted outcomes of their risk class (II, 76% survival). 15 Of note, mortality rates of patients with opioid overdoses requiring intensive care admission is about 10%, and this mortality is most often related to respiratory failure. 19 The overall numbers of these patients has doubled over the past 10 years, which suggests that this indication for ECMO will likely become more prevalent. 20
While there were substance use-specific consultations for the patients in this study, there was no standardization in the counseling provided; especially given the variety of drugs and alcohol used. During the follow-up period three of the surviving intoxication cohort patients died after discharge. The cause of death was unknown for two of them, but the third was secondary to another overdose. This highlights the need for counseling and intensive follow-up with addiction specialists. Of note, a prior case series studying ECMO for patients following suicide attempts stressed that prior psychiatric illness should not preclude the use of this therapy unless it disqualifies from a likely destination treatment modality such as transplantation. 21 Interestingly, the patients in that series were relatively young (median age 36) and 80% presented with positive drug screens. Thus, patients with AI should not be stigmatized against when considering acceptance by an ECMO referral center based solely on their overdose status.
Stigmatization of drug-using patients by healthcare providers is well-documented generally, though there is a paucity of studies concerning this phenomenon in the critical care setting; and none at all concerning ECMO. Brener et al described predictors of support for discriminatory treatment among health care workers for those who inject drugs. 22 Multiple regression analysis found that discomfort with the practice itself and the supposed behavior of the patients predicted advocacy for proposed hypothetical discriminatory treatment and care. This stigma is frequent and has far reaching implications for these patients as noted by Van Boekel et al in their systematic review of unequal healthcare delivery by nurses and physicians for substance-use patients. 23 Here we demonstrate similar outcomes as would be predicted by standard ECMO scoring systems despite their underlying drug use.
There are several limitations to this study. First is its retrospective nature. These patients are referred to our center from outside hospitals and so records pertaining to their pretransfer care and initial laboratory values are incomplete. Patients were transferred based on reports from referring facilities, which included their intoxication history in their referral, but did not include specific quantitative values for drug levels. Nor were duration and type of invasive ventilation strategies prior to transfer well documented. This makes for a rather heterogeneous acute intoxication population without many specifics concerning the individual events other than a general description of the underlying etiology. Our available data lacks the granularity to differentiate between a single large aspiration event vs. an accumulation of multiple smaller chronic aspirations which might portend a different type of lung injury and outcome.
However, this ambiguity is typical of referrals to tertiary ECMO centers, which often base acceptance on established algorithms, none of which include intoxication status. So, while not necessarily meaningful for specific intoxications, this data demonstrates that AI in general is not associated with increased adverse outcomes and should be acceptable for cannulation and transfer.
The second limitation is that this is a single center study. These patients were admitted to a dedicated, high-volume, VV ECMO unit and may limit the external validity of these findings while likely decreasing variability in their care. 24 Third, although we have institutional guidelines for the indications for VV ECMO, we do not have information on AI patients referred for VV ECMO that were not offered the therapy and thus introducing a survival bias. Fourth, there was no comprehensive follow-up data available for these patients including any disease-specific long-term endpoints. Thus, questions concerning relapse rates or extended survival are unanswerable for many of these patients.
Conclusion
We demonstrated no difference in survival to hospital for discharge for patients supported with VV ECMO following an AI when compared with non-AI patients. For those who survive to hospital discharge it is imperative that the underlying pathology of the acute intoxication be addressed with counseling and referral to addiction specialists to prevent relapse episodes. However, respiratory failure refractory to conventional therapies due to an acute intoxication should not be considered an absolute contraindication for VV ECMO therapy and so patients may be accepted for transfer to ECMO centers.
Footnotes
Authors’ Note
The views expressed in this manuscript are those of the authors and do not reflect the official policy of the Department of the Army, the Department of the Air Force, the Department of Defense, or the United States Government.
Standard Disclaimer and Copyright Protection
Our team is comprised partly of military service members and employees of the US Government. This work was prepared as part of our official duties. Title 17 U.S.C. 105 provides that ‘Copyright protection under this title is not available for any work of the United States Government.’ Title 17 U.S.C. 101 defines a U.S. Government work as a work prepared by a military service member or employee of the US Government as part of that person’s official duties.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.