
Abstract
Background:
Monitoring oxygen delivery to the oxygenator of a heart lung machine (HLM) is typically accomplished with an O2 analyzer connected to the gas inflow line. It is assumed when the FiO2 is greater than 21% that oxygen is being delivered to the oxygenator. However, this assumption is imperfect because the connection of the inflow line to the oxygenator is downstream from the O2 analyzer. FiO2 monitoring will not alert the perfusionist if the inflow line is not actually connected to the oxygenator. Measuring the fraction of expired oxygen (FEO2) is a more reliable way of monitoring O2 delivery.
Methods:
An O2 analyzer was placed on the scavenging line that is attached to the exhaust port of oxygenator (FEO2).
Results:
Whenever the FiO2 is greater than 21%, and the inflow line is properly connected, the FEO2 exiting the oxygenator is greater than 21%. The FEO2 falls to 21% when the inflow line is not functioning.
Conclusion:
Monitoring the FEO2 is a more reliable way to verify O2 delivery to an oxygenator. An alarm can be set on the FEO2 monitor to alert the perfusionist if the FEO2 falls below a predetermined threshold so any issue with O2 delivery will always be recognized.
Overview
The Heart Lung Machine (HLM) is a complex technological system; while allowing oxygen and blood delivery to patients undergoing cardiopulmonary bypass (CPB) procedures, it has points of vulnerability where failures may occur. One critical aspect of the HLM is the oxygen delivery system; failure to deliver oxygen to the oxygenator will cause deoxygenated blood to enter the arterial limb of the CPB circuit potentially resulting in direct patient harm. 1 Mejak et al. 2 reported in a retrospective study on the probability of occurrence of perfusion incidents that 273 oxygenator failures had occurred in a 2-year span at the hospitals surveyed. Of those failures, 129 were due to oxygen delivery issues, not structural failures of the oxygenator requiring change out. To safeguard oxygen delivery to the oxygenator, the Standards and Guidelines for Perfusion Practice recommend using an inline oxygen analyzer. 3 This is spliced into the gas inflow line between the oxygen source and the oxygenator connection. A significant limitation of this configuration is that the oxygen analyzer is located upstream of the oxygenator; as such, inadequate oxygen delivery downstream from the analyzer might not be detected until the patient’s arterial saturation begins to decline. A disconnected gas inflow line, exhaust port obstruction, or vaporizer output reduction are examples of events that could result in critically low oxygen delivery despite a fraction of inspired oxygen (FiO2) as high as 100%. 4 We propose a simple, inexpensive, and more comprehensive approach of confirming oxygen delivery to the oxygenator by monitoring the fraction of expired oxygen (FEO2) leaving the exhaust port of the oxygenator.
Description
Per OSHA recommendations, a scavenging line under suction should be connected to the exhaust port of the HLM oxygenator to capture isoflurane gas exiting the device. 5 We added an O2 analyzer to the scavenging line of an Affinity NT oxygenator (Medtronic, Minneapolis, MN, USA) to measure the FEO2. It should be noted that this oxygenator has multiple gas vents to prevent membrane damage in the event of accidental occlusion of the scavenging line or vacuum system. If safety vents were not present on a particular oxygenator, it would be prudent to add an open “Y”-connector to the exhaust port to prevent occlusion.
We observed that when the FiO2 delivered to the inlet of the oxygenator was greater than room air (21%), the FEO2 exiting the oxygenator was also greater than 21% (Figure 1). Upon cessation of delivery of a higher than room air FiO2 to the oxygenator (the FiO2 was reduced to 21% or the gas inflow line became disconnected from the gas inlet of the oxygenator) the FEO2 fell to 21% (Figure 2).
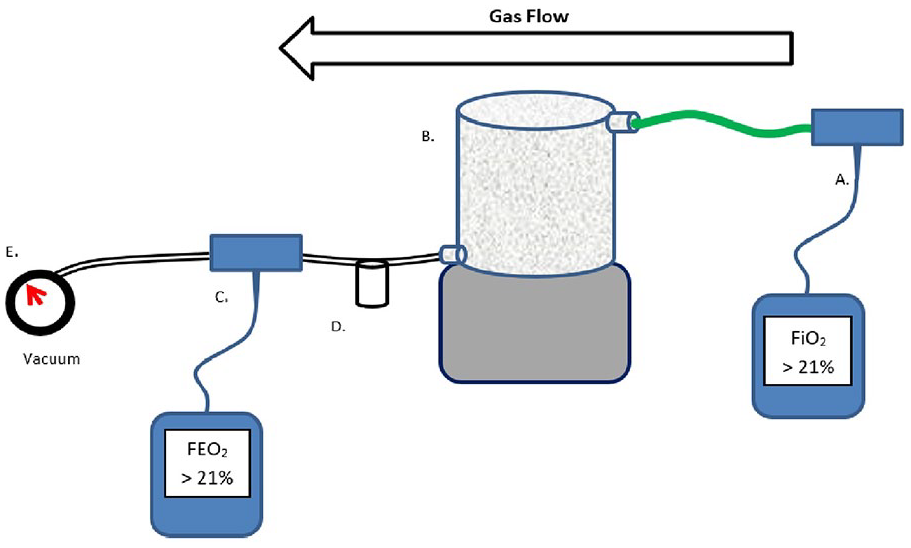
Schematic of a FEO2 analyzer with gas inflow line attached.
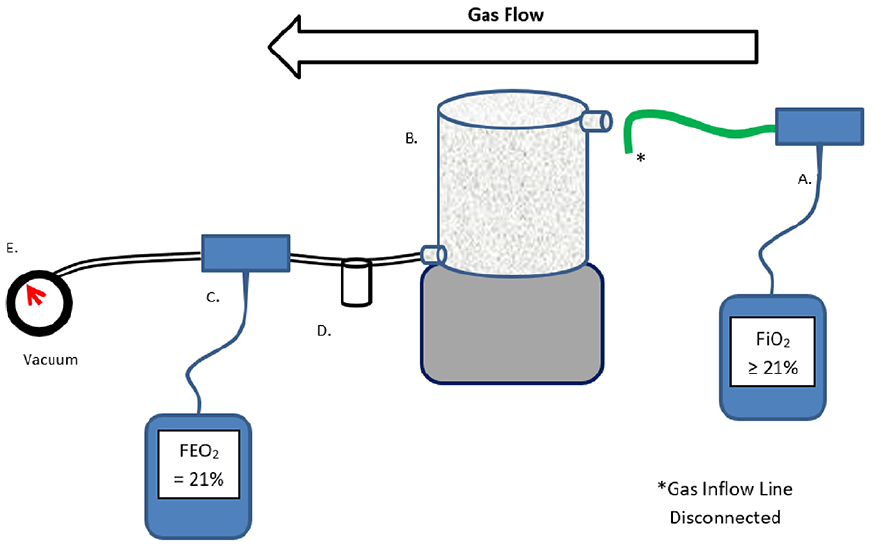
Schematic of a FEO2 analyzer with gas inflow line detached.
Discussion
Application of this technique demonstrates that monitoring the FEO2 on the scavenging line with an oxygen analyzer is a simple, inexpensive, and reliable way to verify oxygen delivery to the oxygenator. A FEO2 >21% serves as verification that the oxygen delivery system on the HLM is connected and functioning because the only mechanism to achieve a FEO2 >21% is to deliver a FiO2 higher than what is found in the atmosphere to the oxygenator. Relying on FiO2 monitoring alone will not provide evidence of a disconnected oxygen line because the line connection to the oxygenator is downstream of the oxygen analyzer.
This FEO2 monitoring safeguard could be extended further with the addition and activation of an audible alarm on the O2 analyzer that triggers when the FEO2 levels drop below a customized threshold. In our practice the O2 analyzer alarm is set at a FEO2 of 25%. Hence, if the oxygen line becomes disconnected, or another O2 delivery failure occurs, the FEO2 will fall below the 25% threshold and trigger the alarm within seconds.
Other methods of verifying oxygen delivery to an oxygenator have been proposed, but they are more complex and require the purchase of new devices. 6 This technique requires only an oxygen analyzer, which most perfusion teams already own, and takes advantage of the isoflurane scavenging line. Some centers already use capnographs on the exhaust ports of oxygenators as a predictor of arterial carbon dioxide tension. 7 These capnographs are often capable of measuring FEO2. In these instances, centers should consider taking advantage of their system by monitoring the FEO2 in addition to the PexCO2.
It is important to note that monitoring FEO2 alone will not validate the FiO2 setting on the gas blender, as a specific FEO2 will not directly correlate with a specific FiO2. This is the result of variances in gas exchange due to different membrane manufacturers, blood temperature, flow rate and resident time variability, and room air drawn into the scavenging line through the safety ports or “Y”-connector diluting the exhaust oxygen. However, in our clinical practice we have observed the FEO2 always remaining >21% when the oxygen delivery system is functioning appropriately. Clinicians should focus on this parameter rather than the absolute value of the FEO2. It may also be useful to simultaneously monitor FiO2 and FEO2 with separate O2 analyzers. This allows the perfusionist to concurrently verify that the FiO2 correlates with the blender setting, and that the oxygenated gas has passed through the oxygenator.
Footnotes
Article note
This work was presented as a poster presentation at the AATS Patient Safety Course, Boston, MA, June 29th–30th, 2018.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.