
Abstract
Objective:
Intra-aortic balloon pump (IABP) is currently recommended as a strategy to address the increased afterload in patients who received venoarterial extracorporeal membrane oxygenation (VA-ECMO). The benefit of VA-ECMO with IABP in postcardiotomy cardiogenic shock is inconclusive. A systematic review and meta-analysis was conducted to assess the influence of VA-ECMO with IABP for postcardiotomy cardiogenic shock (PCS).
Methods:
The Cochrane Library, PubMed, and Embase were searched for all articles published from 1 January, 1964 to July 11, 2020. Retrospective cohort studies targeting the comparison of VA-ECMO with IABP and isolated VA-ECMO were included in this study.
Results:
We included 2251 patients in the present study (917 patients in the VA-ECMO with IABP group and 1334 patients in the isolated VA-ECMO group). Deaths occurred in 589 of 917 patients (64.2%) in the VA-ECMO with IABP group and occurred in 885 of 1334 patients (66.3%) in isolated VA-ECMO group. Pooling the results of all studies showed that VA-ECMO with IABP was not related to a reduced in-hospital mortality in patients who received VA-ECMO for PCS (RR, 0.95; 95% CI, 0.86–1.04; p = 0.231). In addition, VA-ECMO with IABP was not related to an increased rate of VA-ECMO weaning in patients who received VA-ECMO for PCS (RR, 1.28; 95% CI, 0.99–1.66; p = 0.058).
Conclusions:
This study indicates that VA-ECMO with IABP did not improve either in-hospital survival or weaning for VA-ECMO in postcardiotomy cardiogenic shock patients.
Keywords
Introduction
About 0.5%–1% of patients undergoing cardiac-related operations suffer from refractory postcardiotomy cardiogenic shock (PCS), which is related to an increased mortality.1,2 Venoarterial extracorporeal membrane oxygenation (VA-ECMO) has been incrementally applied to treat PCS over the past over the last few decades. 2 However, the effect of VA-ECMO on PCS remains unclear. VA-ECMO increases left ventricular pressure attributable to retrograde aortic perfusion, which might slow myocardial recovery or damage the myocardium and negatively affect survival. Intra-aortic balloon pump (IABP) is currently recommended as a strategy to address the increased afterload in patients who received VA-ECMO. 3 By decreasing the afterload of left ventricular, IABP might theoretically help myocardial recovery and facilitate successful weaning from VA-ECMO, ultimately resulting in improved survival in PCS patients. Actually, the effect of VA-ECMO with IABP in PCS is uncertain. Several retrospective cohort studies showed that VA-ECMO with IABP did not reduce either short-term mortality or morbidity in PCS patients.4–6 Given the debatable efficacy of VA-ECMO with IABP, a systematic review and meta-analysis was conducted to compare isolated VA-ECMO to VA-ECMO with IABP, aiming to evaluate the effects of VA-ECMO with IABP for patients who underwent cardiac surgery.
Materials and methods
This study was performed based on the manuals of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and the meta-analysis of observational studies in epidemiology (MOOSE) group.7,8 The Cochrane Library, PubMed, and Embase were searched for all articles published from 1 January,1964 to July 11,2020. We used these terms: “extracorporeal or extracorporeal membrane oxygenation or extracorporeal life support or ECMO or ECLS” and “intra-aortic or intra-aortic balloon pump or intra-aortic balloon counter-pulsation and IABP.” The ongoing or completed studies on the same topic on ClinicalTrials.gov were also searched. Furthermore, we reviewed the references of the identified studies to obtain more relevant publications.
Literature selection criteria
We establish the selection criteria for our systematic review and meta-analysis according to the population, intervention, comparator, outcome, and study design (PICOS) approach. We excluded studies with incomplete data. We included studies if they meet the following criteria:
Population: We included postcardiotomy patients who experience refractory heart failure. We excluded studies which included patient with an age of less than 18 years or patients with acute respiratory failure or non-PCS. We excluded small studies that included fewer than 30 patients. When there was an overlap among studies in population, we only included the study with the largest population.
Intervention: VA-ECMO with IABP. We excluded studies targeting venovenous ECMO or left ventricular assist device.
Comparator: The isolated VA-ECMO group and the VA-ECMO with IABP group.
Outcome: VA-ECMO weaning, in-hospital mortality.
Study Design: Retrospective cohort studies.
Data collection and quality assessment
D.H. and A. X. independently identified all retrospective cohort studies meeting our inclusion criteria. We contacted the authors of included studies to get more detail information if data was missing. We will discuss if there were disagreements between the two authors. The following information was extracted by the two authors: authors, year, country, number of patients, age, male, surgical procedures, VA-ECMO weaning, and in-hospital mortality. We used the Newcastle Ottawa Scale to evaluate the methodological quality of retrospective cohort studies. A score of less than five indicated a high risk of bias, whereas a higher overall score suggested a lower risk of bias. The authors also evaluated the risk of bias together.
End points
The primary end point was in-hospital all-cause mortality, and deaths that occurred after hospital discharge were censored. The secondary end point was successful VA-ECMO weaning.
Statistical analyses
We used Risk Ratios (RR) with a 95% confidence interval (95% CI) to show the results. We used the Q statistic (p of less than 0.1 suggested a significant heterogeneity) and I2 test (I² of more than 50% indicated a significant heterogeneity) to assess statistical heterogeneity (13). Considering different clinical and methodological characteristics across the retrospective cohort studies, we used the random-effects model for outcome comparisons. We used the Mantel–Haenszel method to pool the estimated RR. The Egger tests and funnel plot were performed to assess publication biases. In addition, we performed a one-way sensitivity analysis to assess the effect of each study on the estimated effect by omitting one study at a time. p-Values of less than 0.05 were considered statistically significant. We used R version 4.0.3 software (the R Foundation, https://www.r-project.org/) for all data analyses.
Results
Search selection
The study search and selection process and reasons for exclusion are depicted in Figure 1. We identified 817 records through a systematic search of the online databases. Of those, 114 were excluded because of duplicates and 633 were excluded after screening based on titles and abstracts. We reviewed the full-text of the remaining 70 publications and selected 10 studies meeting the inclusion criterion.4–6,9–15 Characteristics of included studies are showed in Table 1. We included 2251 patients in the present study (917 patients in the VA-ECMO with IABP group and 1334 patients in the control group). None of the included studies were randomized controlled trials. There was only one multicenter study among the ten included studies. 10 In-hospital mortality was reported in all studies, and VA-ECMO weaning rate was reported in only four studies. Moreover, about 66% of patients came from three studies.4,10,14 In most of the included publications, patients undergoing VA-ECMO had a mean age of more than 60 years, and 72% of the patients were men. Surgical operations related to cardiogenic shock included coronary artery bypass grafting, valve procedure, and aortic procedure.
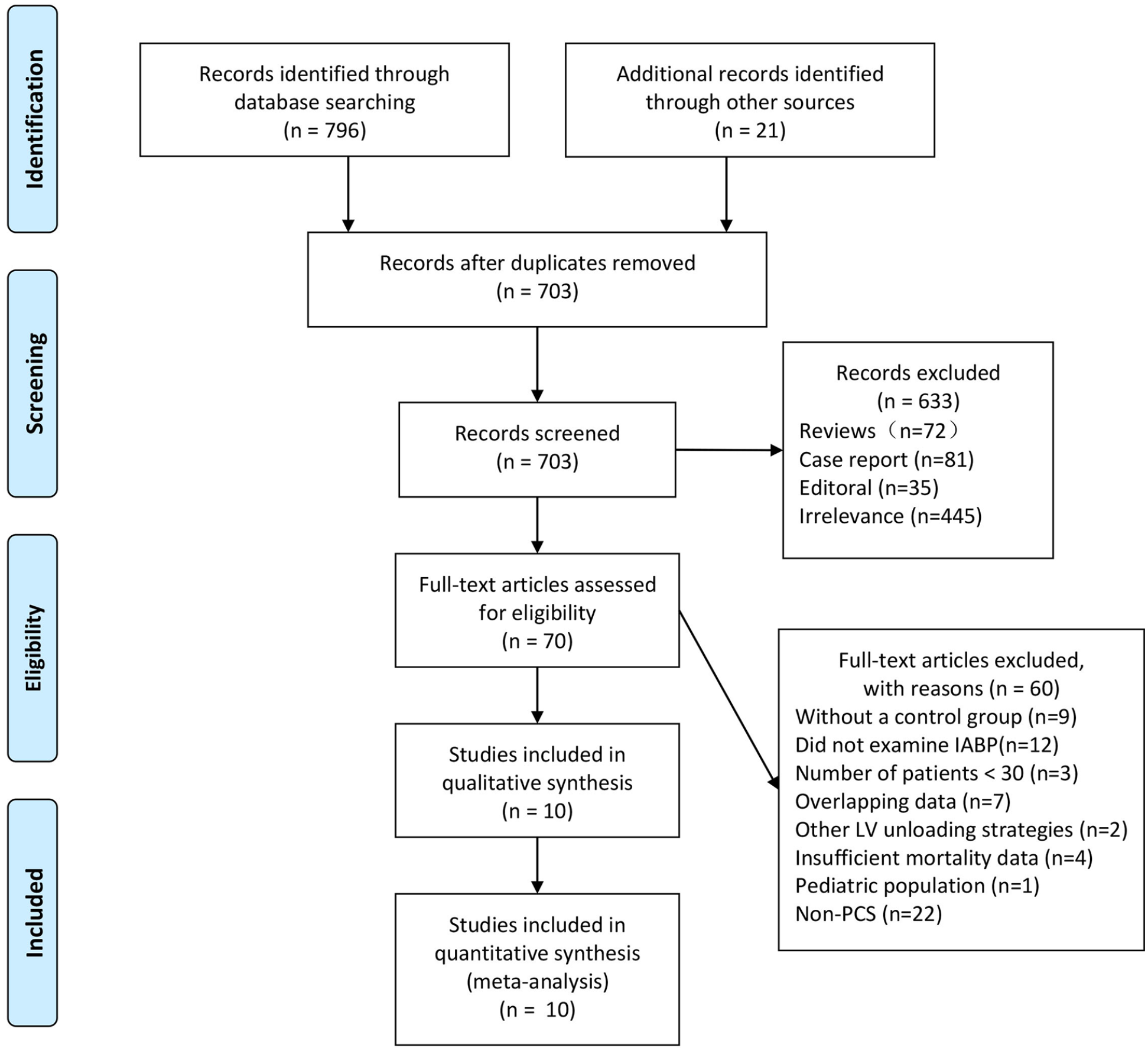
Study search and selection process.
Characteristics of included studies.
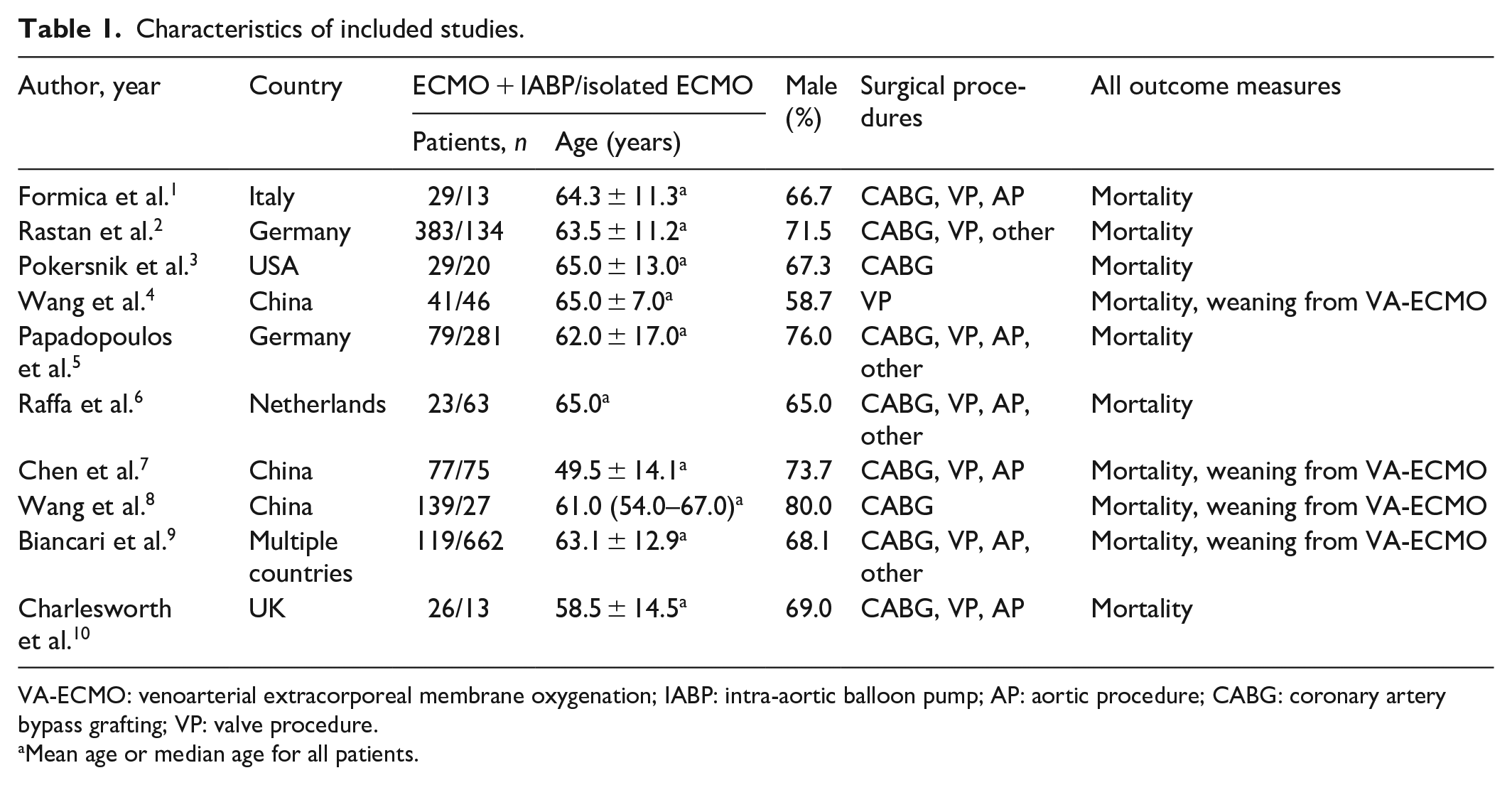
VA-ECMO: venoarterial extracorporeal membrane oxygenation; IABP: intra-aortic balloon pump; AP: aortic procedure; CABG: coronary artery bypass grafting; VP: valve procedure.
Mean age or median age for all patients.
Risk of bias
Risk of bias for all studies based on the Newcastle-Ottawa Scale was presented in Table 2. All of the included observational studies had a score of more than 5, suggesting a low risk of bias. However, among included studies, characteristics of patients did not have good comparability between the VA-ECMO with IABP group and the isolated VA-ECMO group.
Risk of bias for observational studies.
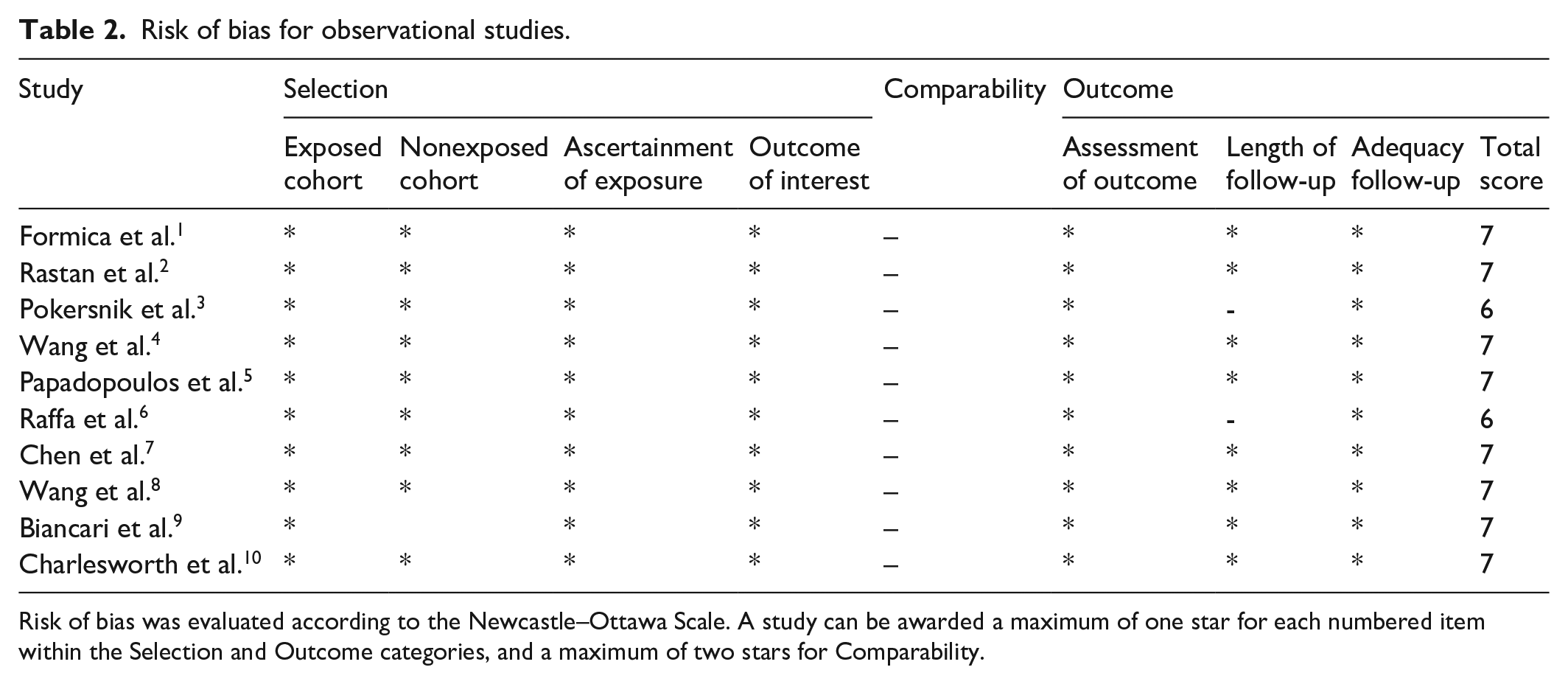
Risk of bias was evaluated according to the Newcastle–Ottawa Scale. A study can be awarded a maximum of one star for each numbered item within the Selection and Outcome categories, and a maximum of two stars for Comparability.
Primary endpoint
In-hospital mortality was available in all of the included studies.4–6,9–15 We presented the pooled results of in-hospital mortality in Figure 2. We included a total of 2251 patients in this analysis. In the VA-ECMO with IABP group, deaths occurred in 589 of 917 patients (64.2%); in the isolated VA-ECMO group, deaths occurred in 885 of 1334 patients (66.3%). Pooling the results of the included studies showed that VA-ECMO with IABP was not related to a reduced in-hospital mortality in patients who received VA-ECMO for PCS (RR, 0.95; 95% CI, 0.86–1.04; p = 0.231), without substantial heterogeneity (I2 = 22.1%, p = 0.240). The results of the Egger test (p = 0.32) and the symmetrical funnel plot was symmetrical (Figure 3) might suggested a low risk of publication bias. One-way sensitivity analysis was also performed to estimate the effect of each study on in-hospital death, in which omission of each study did not make a significant difference (Figure 4).
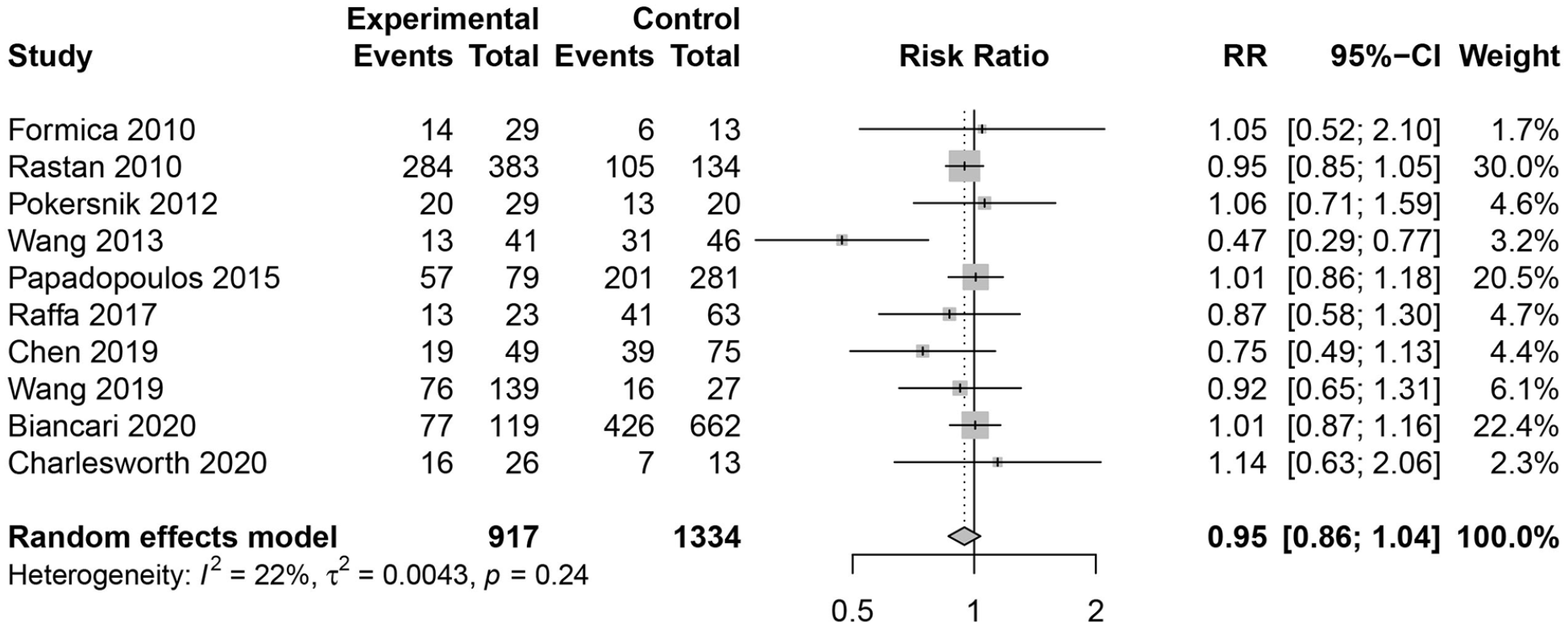
In-hospital mortality in patients supported on VA-ECMO with IABP versus isolated VA-ECMO.
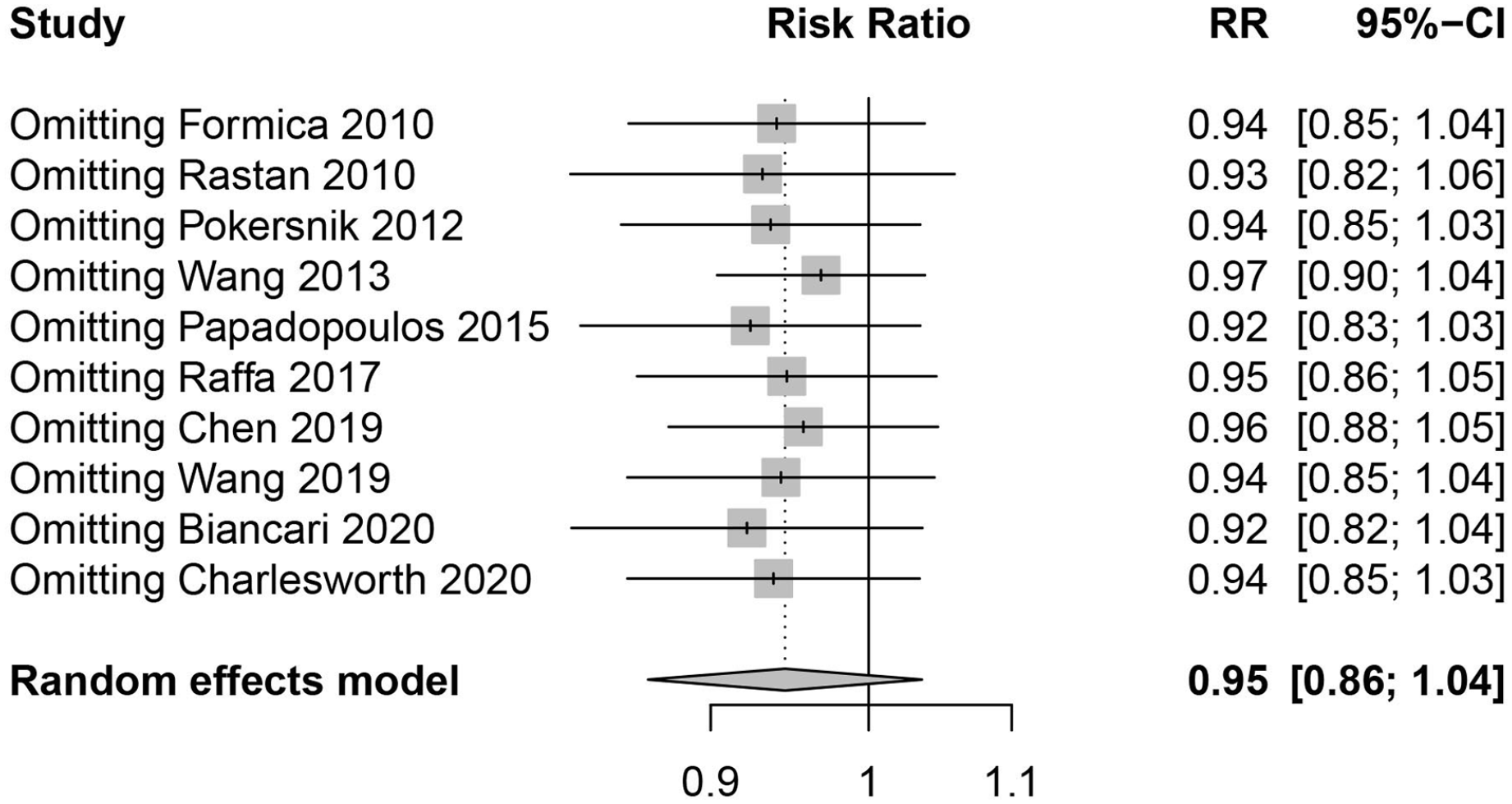
One-way sensitivity analysis of in-hospital mortality.
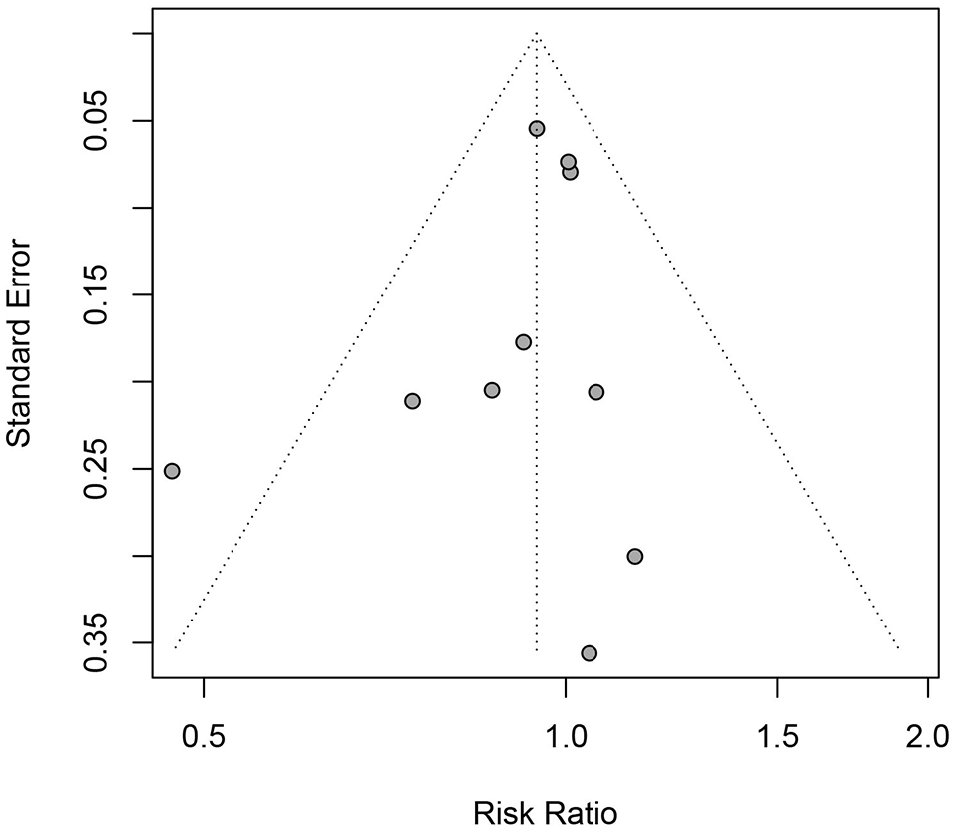
Funnel plot of in-hospital mortality.
Secondary endpoint
The incidence of weaning from VA-ECMO was available in four studies.10–12,15 In the VA-ECMO with IABP group, successful weaning occurred in 225 of 348 patients (64.7%); In the isolated VA-ECMO group, successful weaning occurred in 429 of 810 patients (53.0%). Pooling the results of the included studies showed that VA-ECMO with IABP was not related to an increased rate of VA-ECMO weaning in patients who received VA-ECMO for PCS (RR, 1.28; 95% CI, 0.99–1.66; p = 0.058; Figure 5), with a significant heterogeneity (I2 = 70%, p = 0.017).

Incidence of weaning from VA-ECMO in patients supported on VA-ECMO with IABP versus isolated VA-ECMO.
Discussion
Our study included 10 observational studies to evaluate the effects of VA-ECMO with IABP for patients who suffered from PCS after cardiac surgery. This study suggested that VA-ECMO with IABP was not related to a reduced in-hospital mortality and did not increase the incidence of VA-ECMO weaning in patients who received VA-ECMO for PCS.
VA-ECMO use addresses the central problem of severely reduced cardiac output in cardiogenic shock by providing adequate tissue perfusion. However, increased afterload because of retrograde aortic perfusion interferes with myocardial recovery and could negatively affect outcome. Decreasing the afterload of left ventricular during VA-ECMO may either provide an actual approach to functional rest and facilitate myocardial recovery. IABP has been widely used to provide circulatory support during the last few decades, which could reduce left ventricle afterload and increase coronary artery blood flow. 16 In this context, IABP has been widely used as an approach of left ventricle unloading in patients undergoing VA-ECMO for PCS. However, there always has been controversy regarding whether IABP use can improve outcomes in patients who received VA-ECMO for PCS.
Previously, several publications have centered on the comparison of VA-ECMO with IABP and isolated VA-ECMO use. Russo et al. 17 included 17 observational studies with 3997 patients receiving VA-ECMO and found that left ventricular unloading was related to reduced mortality in patients supported with VA-ECMO for cardiac shock. Kowalewski et al. 18 also found that VA-ECMO with left ventricular unloading was related to a lower in-hospital mortality and higher incidence of VA-ECMO weaning. Wang and Xing 19 conducted a systematic review and meta-analysis with 3704 patients to assess the effect of ECMO with IABP in cardiac shock or cardiac arrest, and they demonstrated that ECMO with IABP could increase the incidence of successful weaning from VA-ECMO, but did not reduce in-hospital mortality. However, all these meta-analyses have not only focused on patients supported on VA-ECMO combined with IABP or patients with PCS.
Currently, there are few systematic review and meta-analyses to focus on patients who received VA-ECMO for PCS for assessing the effect of VA-ECMO with IABP in PCS. In our study, 10 retrospective cohort studies with 2251 patients were selected and one-way sensitivity analysis was performed to assess the effect of each study on the estimated effect by omitting one study at a time. Moreover, risk of bias for each study based on the Newcastle-Ottawa Scale indicated that all studies were of good methodological quality.
In our study, we included 2251 patients who underwent VA-ECMO for PCS, and patients supported on ECMO with IABP had lower short-term mortality than those supported on isolated VA-ECMO (64.2% vs 66.3%). However, VA-ECMO with IABP was not related to a reduced in-hospital mortality in patients who received VA-ECMO for PCS when pooling the results of the included studies. In many centers, IABP was always the first choice for PCS. 20 VA-ECMO might be implanted directly when IABP did not work or was not immediately available. When there were signs of increased afterload, IABP can be used to unload left ventricular during VA-ECMO. Only small number of patients might receive additional IABP for left ventricular unloading during VA-ECMO in the included studies, which might account for our findings. Pooling the results of the included studies showed that VA-ECMO with IABP was not related to an increased rate of VA-ECMO weaning for those who received VA-ECMO for PCS. Actually, the rate of ECMO weaning seemed to be much higher in the VA-ECMO with IABP compared to the control group (64.7% vs 53.0%). VA-ECMO with IABP had an imprecise association with weaning from VA-ECMO when using random effects model. One possible reason was only four studies reporting data on VA-ECMO in the present study.
However, there are some limitations in our study. First, we included only 10 studies and all studies were retrospective cohort studies without random allocation of intervention, which may have affected our results. The real effect of VA-ECMO with IABP in PCS has not been certain and still required randomized controlled trials. Second, the rate of VA-ECMO weaning available in only four studies. The real influence of IABP on VA-ECMO weaning might have been underestimated. Third, characteristics of patients did not have good comparability between the VA-ECMO with IABP group and the isolated VA-ECMO group, which might have affected the effect of VA-ECMO with IABP in PCS. Finally, our conclusion seemed to depend on the pooled results of three large studies. In this context, one-way sensitivity analysis was performed to assess the influence of each study on the estimated influence by removing one study at a time, in which the results were stable.
In a word, this study indicates that VA-ECMO with IABP did not improve either in-hospital survival or VA-ECMO weaning in patients supported on VA-ECMO for PCS. Randomized controlled studies targeting outcomes of VA-ECMO with IABP are still need to evaluate the effects of VA-ECMO with IABP for patients with PCS.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
The study was a systematic review and meta-analysis. Ethics approval and consent to participate was not required.
Authors’ contributions
Conception and design: DH and AX. Analysis and interpretation: QG and JQ. Drafting of the manuscript: DH. Revision of the manuscript: CZ. All authors read and approved the final version.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.