
Abstract
Background
Acute kidney injury (AKI) after cardiac surgery is a well-known risk factor for increased postoperative mortality and morbidity. The effect of postoperative developed AKI on postoperative outcomes in patients after Bentall procedure has been incompletely investigated. The present study was dedicated to assessing the impact of postoperative AKI on morbidity and 30-day mortality in this specific cohort.
Methods
In a retrospective observational study, we investigated 249 patients undergoing Bentall procedure from January 2014 to March 2018 at the University Hospital of Cologne, Germany. After excluding patients with preoperative renal impairment, patients were divided into an AKI group (n = 88) and a non-AKI group (n = 97). Postoperative outcomes and 30-day mortality were analyzed using univariate regression analysis. AKI was defined by AKIN criteria.
Results
Mortality during ICU and hospital stay, as well as 30-day mortality, was significantly higher in the AKI group (all p < 0.001). Patients with postoperative developed AKI revealed 9.3-fold higher odds for ICU mortality and 6.7-fold higher odds for 30-day mortality in comparison to non-AKI group (all p < 0.004) as well as 4.5-fold higher odds for stroke. Coronary artery bypass time, as well as cross-clamp time, were similarly distributed between groups, whereas incidences of postoperative bleeding, myocardial infarction, and need for rethoracotomy occurred significantly more often in patients with postoperatively developed AKI (all p < 0.04).
Conclusion
Patients undergoing Bentall surgery who postoperatively developed AKI showed significantly higher morbidity and mortality. AKI points out to be an early predictor for poor outcomes. Thus, as a consequence, patients with postoperatively developed AKI should be highly monitored for immediate intervention.
Introduction
Acute kidney injury (AKI) after cardiac surgery is a well-known risk factor for increased postoperative mortality.1,2 Incidence of acute kidney injury (AKI) after cardiac surgery ranges from 1% to 30%.1,3 Some studies report that use of cardiopulmonary bypass (CPB) during cardiac surgery initiates a systemic inflammatory response (SIRS) often contributing to the development of post-surgical complications, including AKI. 4 Bentall procedure is considered the gold standard in the treatment of patients requiring aortic root replacement and is associated with an extended cardiopulmonary bypass time due to the complexity of surgical procedure. 5 Besides these risk factors, a history of preoperative existing hypertension and diabetes mellitus, as well as anamnesis of smoking and left ventricular dysfunction, can negatively influence perioperative kidney function.6–8
Postoperative complications, such as the need for blood transfusions, are known to trigger the incidence of development of postoperative AKI. 9 Volume decrease due to blood loss could induce a pre-renal dysfunction and lead to episodes of postoperative atrial fibrillation. 10 Also, the increased necessity of re-exploration and more frequent postoperative bleeding are associated with impaired kidney function.11,12
Outcomes and mortality of patients after Bentall surgery with postoperative developed AKI have been incompletely investigated. The present study assessed the impact of postoperative AKI development on outcomes and mortality in patients undergoing Bentall surgery with the objective of presenting AKI as an early marker on poor outcomes and mortality.
Materials and methods
Two hundred forty-nine consecutive patients were diagnosed for Bentall procedure and were referred to our institution for surgical treatment from January 2014 to March 2018. After excluding patients with preoperative renal impairment residual patients were analyzed with particular focus on the impact of postoperative developed AKI on outcomes and mortality. Patients were divided into AKI group (n = 88) and non-AKI group (n = 97). Elective, as well as emergent and urgent Bentall surgeries, were included in this study. Outcomes and 30-day mortality were analyzed as primary endpoints as well as baseline characteristics and perioperative parameters. Univariate regression model was used for determining odds ratios.
This study has been carried out in accordance with the Declaration of Helsinki. The study design was a retrospective review of collected registry data. The Ethics Committee of the Medical Faculty of the University of Cologne waived ethics approval and written informed consent for data collection from patients.
AKI was defined according to Acute Kidney Injury Network (AKIN) as a serum creatinine increase of >0.3 mg/dL within 48 h or serum creatinine increase>/ = 50% after surgery. We did not use urine output criteria for defining AKI. 13
The main indication for surgery was aortic valve disease associated with ascending aorta or root dilatation. Patients with acute or chronic aortic dissection or aortic root endocarditis were excluded. The type of valved conduit was chosen based on patient age. Moreover, patients’ lifestyle, preference, compliance to oral anticoagulants, and risk factors for bleeding or thrombosis were also considered. The primary outcome of the study was overall mortality. Secondary results were major adverse events.
Surgical procedure
The Bentall procedure is a type of cardiac surgery involving composite graft replacement of the aortic valve, aortic root, and ascending aorta, with reimplantation of the coronary arteries into the graft. A median sternotomy is used to approach the heart and the aorta. A moderately hypothermic cardiopulmonary bypass with cannulation of ascending aorta or proximal aortic arch was used in most cases. When required, an open distal anastomosis of the graft was performed during a period of hypothermic circulatory arrest using either antegrade or retrograde cerebral perfusion according to the surgeon’s preference. Aortic root replacement with a valve-graft composite was performed with either a biological or mechanical valve prosthesis depending on the patient’s age. First, an aortotomy was performed, followed by removal of the affected portion of the ascending aorta and the aortic valve. The coronary arteries were disconnected. Subsequently, a graft with an inside valve was then sewn to the heart and the other side of the aorta. Two small openings were made in the graft, and the coronary arteries were then implanted into the valve-graft composite. After hemostasis thorax was closed by common steps.
Statistical analysis
IBM SPSS Statistics for Windows, Version 23 (IBM Corp. Released 2012; IBM Corp, Armonk, NY, USA) was used for statistical analysis. Continuous data was evaluated for normality using one-sample Kolmogorov–Smirnov Test confirmed by histograms. Continuous variables were expressed as mean +/− standard deviation (SD) in cases of normal distribution or median (interquartile range) in cases of non-normal distribution. Categorical data were expressed as total numbers and percentages. P-Values were determined using Student’s t-Test for normally distributed and Mann–Whitney U-Test for non-normally distributed continuous variables, and the X2 test or Fisher’s Exact Test was used for parametric variables depending on the minimal expected count in each crosstab.
Odds ratios (ORs) were analyzed by using univariate regression analysis. A p-value < 0.05 was considered as significant.
Results
Association of demographics and preoperative baseline characteristics of patients undergoing Bentall surgery with and without development of postoperative acute kidney injury (AKI).
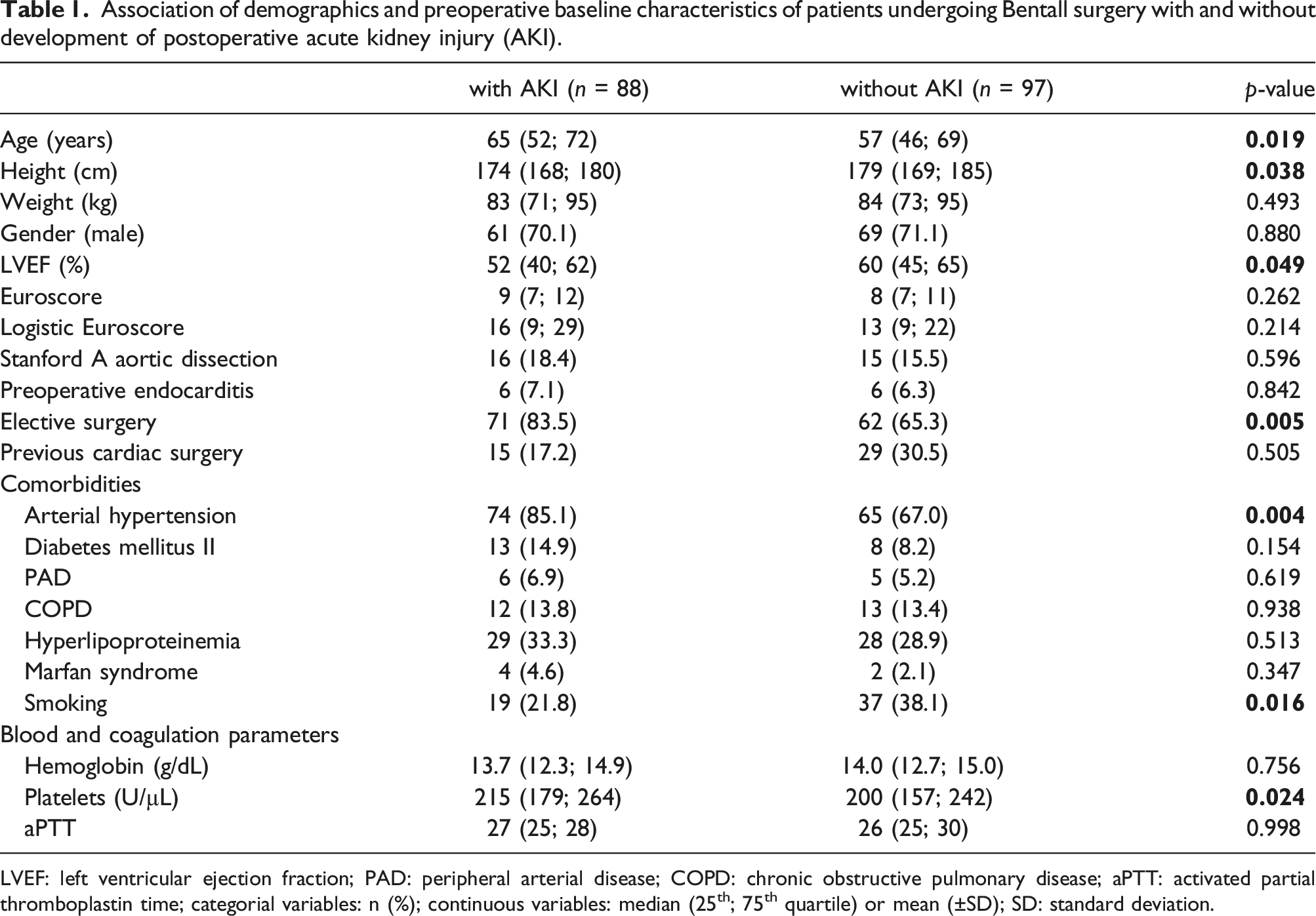
LVEF: left ventricular ejection fraction; PAD: peripheral arterial disease; COPD: chronic obstructive pulmonary disease; aPTT: activated partial thromboplastin time; categorial variables: n (%); continuous variables: median (25th; 75th quartile) or mean (±SD); SD: standard deviation.
Perioperative variables and postoperative outcomes of patients undergoing Bentall surgery with and without the development of postoperative acute kidney injury (AKI).
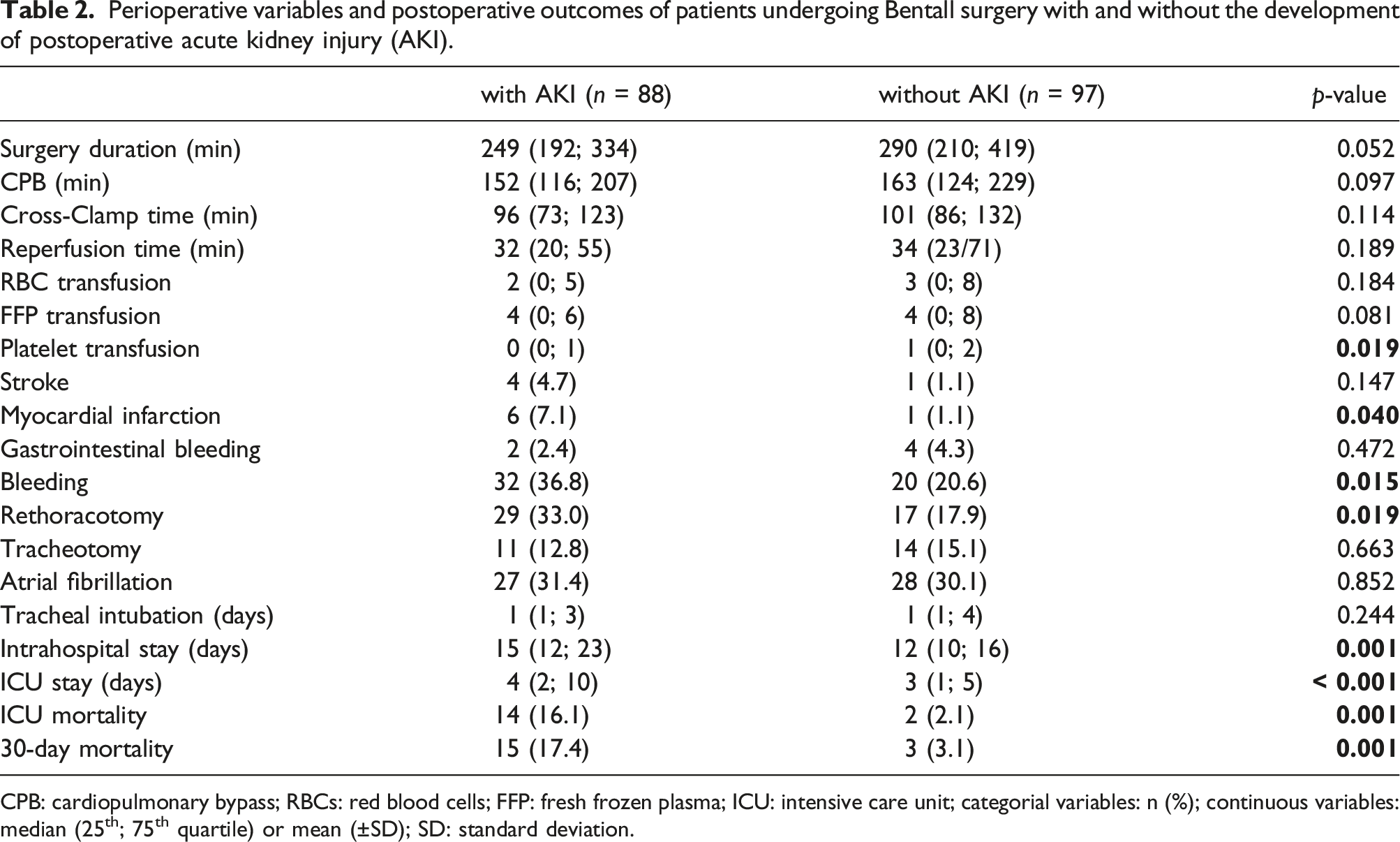
CPB: cardiopulmonary bypass; RBCs: red blood cells; FFP: fresh frozen plasma; ICU: intensive care unit; categorial variables: n (%); continuous variables: median (25th; 75th quartile) or mean (±SD); SD: standard deviation.
Odds ratios (ORs) in favor of AKI development of selected variables.
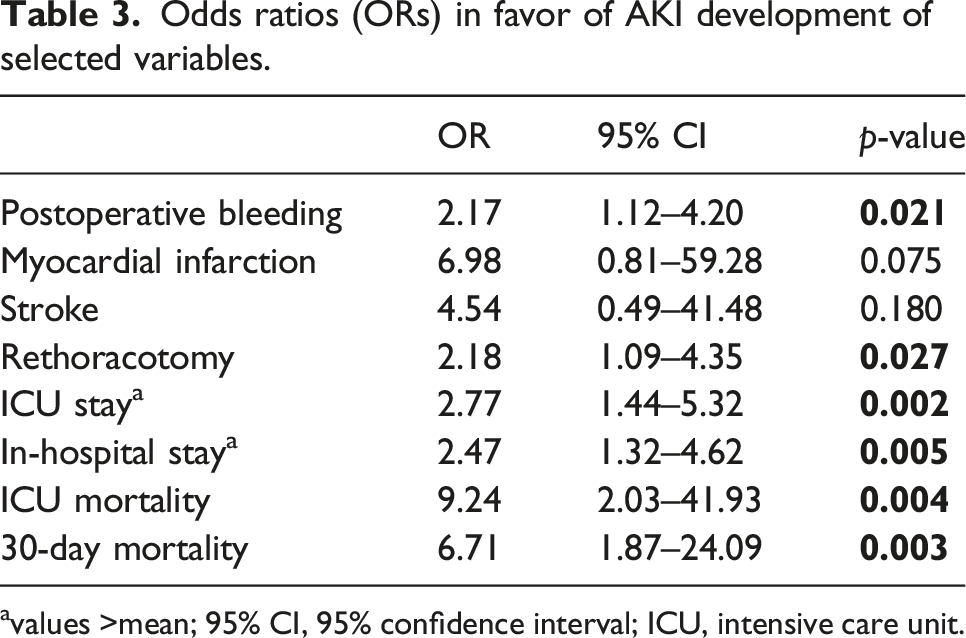
avalues >mean; 95% CI, 95% confidence interval; ICU, intensive care unit.
Discussion
Bentall procedure is the standard therapy for the treatment of acute or chronic aortic valve and aortic root diseases. 5 Despite substantial improvements in surgical techniques, this kind of surgery is still associated with increased morbidity and mortality. 14
Incidence of postoperative AKI after Bentall procedure in our study was higher than in other previous studies.15,16 This discrepancy could be attributed to the longer CPB time in our institution and different definitions of AKI as well as patient profiles.
Patients in AKI group were older than non-AKI group. However, comorbidities such as diabetes, COPD and peripheral arterial disease were similarly distributed between the two groups. Some studies with similar objectives revealed that patients with AKI had a higher prevalence of these comorbidities, such as chronic obstructive pulmonary disease (COPD) and diabetes. 15
Patients with postoperatively developed AKI did not reveal a higher need for transfusions of packed red blood cells and FFP than those without AKI. Interestingly, the non-AKI group needed more platelets than the AKI group. Khan et al. examined the role of blood transfusion in triggering the development of AKI in adults and concluded that the risk of AKI was highest in patients receiving more than two units of red blood cells (RBCs). 17 However, the study was limited by being observational. The direct causal relationship between the need for elevated RBC transfusion and AKI could not be confirmed.
Rethoracotomy due to bleeding was significantly more often performed in patients with AKI. Many potential risk factors for the development of AKI such as hemodilution, decreased hemoglobin level, need for intraoperative transfusion, incidence of hypotension, and status of inadequate oxygen delivery are well-known risk factors for prevalence of peri- or postoperative bleeding.11,12 Patients with acute kidney injury may suffer from disturbance of the coagulation system potentially influencing the prevalence of surgical re-exploration due to bleeding after the initial surgical procedure. 18
Importantly, after a 30-day follow-up, more patients with AKI died, which is similar to the results by Najjar et al 15 . Another study by Lassnigg et al. 19 showed that even a small rise in postoperative serum creatinine was associated with significantly higher mortality. They demonstrated that even a slight creatinine increase in patients revealed a 2.77-fold higher risk for 30-day mortality in comparison to these without creatinine increase. The results were qualitatively similar to the study by Thakar et al 20 .
We also observed that episodes of postoperative atrial fibrillation were similarly distributed between groups. However, patients with AKI who in addition postoperatively developed atrial fibrillation had not only a longer length of in-hospital stay but also a 9-fold increase in mortality compared to the non-AKI group. 21
Limitations of the study
This study is a retrospective analysis of collected registry data from a single tertiary referral center. Thus study power was limited due to a relatively small patient cohort. The non-randomized design, complexity, and variability of the pathophysiology and morphology of the clinical picture of patients requiring Bentall procedure may also have affected the results.
Conclusion
The main message is that postoperative developed AKI is a good early predictor for poor outcomes and mortality. Patients with postoperative developed AKI revealed 9.3-fold higher odds for ICU mortality and 6.7-fold higher odds for 30-day mortality in comparison to non-AKI group (all p < 0.004) as well as 4.5-fold higher odds for stroke. As a consequence, patients with risk for a postoperative development of AKI should be highly supervised. Kidney function in patients after Bentall procedure should be carefully monitored for immediate intervention to minimize severeness and duration of AKI in order to reduce postoperative major adverse events and mortality. Regular measurements of serum creatinine and glomerular filtration especially in the early postoperative phase may prevent further severe complications.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.