
Abstract
Introduction:
Extracorporeal life support (ECLS) patients are at risk for complications caused by gaseous microemboli (GME). GMEs can cause hypoxia, inflammation, coagulation, and end-organ damage. The objective of this in vitro study was to assess dynamics of GME formation during circulation of whole blood or a glycerol blood surrogate. We hypothesized that there is no difference in GME counts and sizes between whole blood and the glycerol blood surrogate and that the membrane lung reduces GME counts over time.
Methods:
A circulation platform was developed using the Cardiohelp ECLS system to run either donor blood or glycerol solution. We conducted 10 repetitions consisting of three phases of ultrasound GME detection using the EDAC™ Quantifier (Luna Innovations, Charlottesville, VA, USA) for each group. Phases were 3-minute recordings at the initiation of 2 L/min flow (Phase 1), post-injection of a GME suspension (Phase 2), and 10 minutes after injection (Phase 3). The number and size of GME pre- and post-ML were recorded separately and binned based on diameter ranges.
Results:
In Phase 1, GME count in blood was higher than in glycerol. In Phase 2, there was a large increase in GME counts; however, most GME were reduced post-membrane in both groups. In Phase 3, there was a significant decrease in GME counts compared to Phase 2. GME > 100 μm in glycerol decreased post membrane.
Conclusions:
We demonstrated GME formation and decay dynamics during in vitro circulation in an ECLS system with blood and glycerol. GME counts were higher in blood, likely due to varying rheological properties. There were decreases in GME levels post membrane in both groups after GME injection, with the membrane lung effectively trapping the GME, and additional reduction 10 minutes after GME injection.
Introduction
Extracorporeal life support (ECLS) is a family of critical-care interventions that supplements or replaces the function of one or more visceral organs or organ systems. A special subset of ECLS capabilities, which pertains to replacement of lung and cardiovascular function, is known as extracorporeal membrane oxygenation (ECMO, henceforth both terms are used interchangeably). The CESAR trial results published in 2006, as well as the successes of ECLS utilization during the H1N1 epidemic in 2009, has led to the increased use of ECLS in both clinical 1 and research settings.2–6 In addition, newer, simplified, and optimized ECLS devices were introduced to the market, fueling a renaissance in ECLS utilization.
One of the under-reported topics in ECLS therapy is that patients are at risk for formation and exposure to gaseous microemboli (GME), especially during transport conditions and during out-of-ICU management in general. GME are bubbles that are trapped in blood vessels and capillary beds and block blood flow, leading to hypoxia and ischemia, endothelial injury and glycocalyx damage followed by edema, inflammation, platelet aggregation, and complement activation.7–9 This can result in neurocognitive dysfunction when capillaries in the brain are affected. 6 These microscopic gas bubbles may be introduced in a patient’s bloodstream as a result of injuries (e.g. chest injuries perforating a lung), cannulation procedures, and/or operator interventions such as during blood draws or infusions of medications. In addition, ECLS priming, high and variable flow rates, turbulence within the ECLS tubing, or pressure changes can introduce microbubbles to an ECLS system and the patient. 9 We conjecture that the above factors are underappreciated as sources of morbidity in critically injured patients undergoing ground transport or, even more so, aeromedical evacuation.
GME can be detected using ultrasound; ultrasound waves that are directed at the fluid are scattered as they interact with GME and other particles. The reflected signals are picked up by the transducer and processed to determine GME sizes and counts over time. 10 Previous GME detection studies were predominantly performed in older cardiopulmonary bypass systems and not in modern ECLS systems used for lung support.7,11–21 More recent work by De Somer et al. found that the EDAC™ was suitable for assessment of GME formation during ECLS. 22
The goal of this study was to construct an in vitro circulation system for GME quantification and calibration ahead of use in clinically relevant large-animal studies on utilization of ECLS for trauma during ground and altitude evacuation. Our objective was to measure GME distributions in an in vitro ECLS circuit with the EDAC™ using both whole blood and a glycerol-water solution as blood surrogate as per De Somer et al., comparing GME characteristics between those media. We hypothesized that there is no difference in GME counts and sizes between whole blood and the glycerol blood surrogate. This hypothesis is essentially an equivalency test between blood and blood surrogate with respect to GME formation. From a potential clinical insight stand point we further hypothesized that the membrane lung reduces GME counts over time.
Methods
This study was performed in an AAALAC-accredited research laboratory after approval by the Institutional Animal Care and Use Committee.
Equipment
Our in vitro perfusion set up involved the Cardiohelp ECLS system and the EDAC™ quantifier (Figure 1). The Cardiohelp system consists of the main drive console with disposable membrane lung (ML, HLS Advanced Set 7.0, Maquet/Getinge Group, Rastatt, Germany) and circuitry. The ML has a gas-exchange surface area of 1.8 m2 of stacked hollow polymethylpentene (PMP) fibers. Standard manufacturer-provided circuitry was used for in vitro circulation, and included a priming bag and tubing (2.3 m in length pre- and post ML with 9.525-mm internal diameter).

In vitro set up. Cardiohelp and HLS advanced set (ML) (a) used for in vitro circulation. Priming bag is used to simulate a patient (b). GME injection port inserted into the pre-ML circuit near the patient surrogate (c). One-way valve inserted into the post-ML tubing near the patient surrogate (d). EDAC™ connectors are spliced into the tubing both pre- (e) and post-membrane (f), with EDAC™ transducers attached to connector.
The EDAC™ system is an FDA-approved device designed to be used in conjunction with an extracorporeal bypass circuit in cardiac surgery. The EDAC™ has hollow plastic connectors that are spliced into ECLS tubing before circulation, which serve as an attachment point for the ultrasound transducers to perform measurements on the fluid (Figure 1(d) and (e)). The EDAC™ is capable of detecting GME from 10 to 1000 μm in diameter, at flows from 0.2 to 6 L/min. 23
In vitro setup
The priming bag was placed 100 cm above the Cardiohelp to facilitate GME trapping (Figure 1(b)). A straight connector fitted with an injection valve on the luer port (Qosina, Ronkonkoma, NY, USA) was inserted in the pre-ML tubing 20 cm from the priming bag to serve as a GME injection port (Figure 1(c)). A one-way valve (Figure 1(d)) was inserted in the post-ML tubing 20 cm from the priming bag to prevent backflow. EDAC™ connectors were spliced into the circuit pre- (Figure 1(e)) and post-ML (Figure 1(f)), 190 cm from the ML.
Study design
The study was carried out in two groups of experiments. The blood group utilized whole blood from donor swine collected in CPDA blood bags (Terumo Cardiovascular Group, Ann Arbor, MI, USA). The glycerol group utilized a blood surrogate consisting of 30%:70% glycerol-water mixture prepared as described by De Somer et al. 22 The in vitro system was primed with blood from donor animals according to IACUC approved studies. Circulation was started within 1 hour of collection of blood from donor animals.
In both groups, 2 L of media (blood or glycerol) were used to prime the in vitro set up. The Cardiohelp was set to circulate at 2 L/min immediately after priming the system. Fluid was maintained at 37°C with a Hemotherm heater (CSZ/Terumo, Ann Arbor, MI, USA) connected to an HLS heat exchanger. For each group, we conducted 10 repetitions consisting of three phases, with each phase having a 3-minute GME recording window. During this recording window, the number and size of GME passing through the EDAC™ connectors pre- and post-ML were recorded separately.
To simplify reporting, recorded GME counts for each phase were “binned” into ranges of measured diameters (Figure 2). The bins used were 10–50 μm, 50–100 μm, 100–150 μm, 150–200 μm, 200–250 μm, and >250 μm (the latter including all GME between 250 and 1000 μm). We discarded any measured counts from 0 to 9 μm, as the EDAC™ counts at this range are unreliable. 22
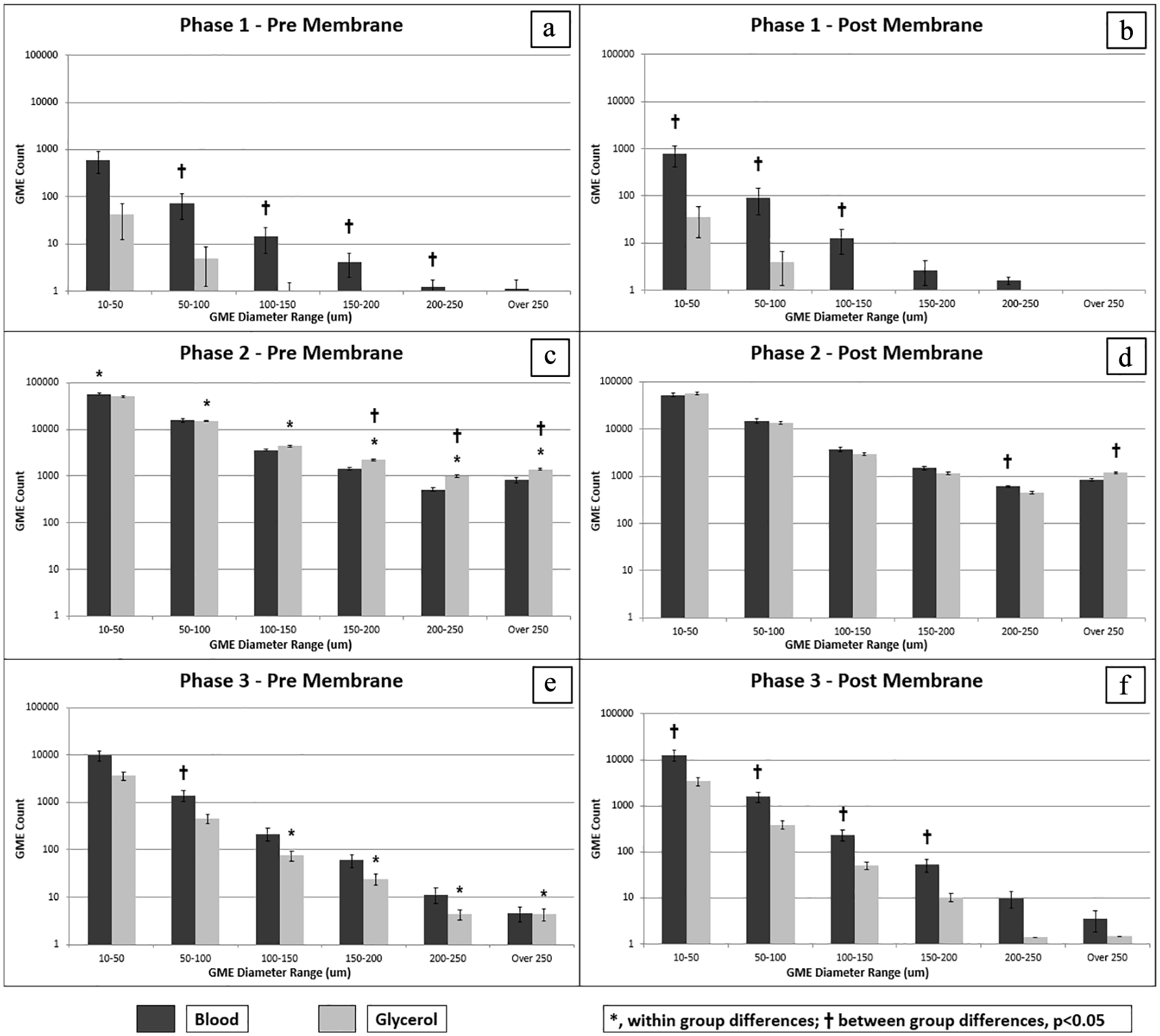
Graph of results. Phases 1 and 2 had 0 GME counted at all size ranges (a–d). Phase 1 (a, b) showed an increase in GME counts in almost all size ranges upon initiation of ECLS flow. Phase 2 (c, d) depicts a 10- to 100-fold increase in GME counts after manual GME bolus insertion. Phase 3 (e, f) showed decreased GME 10 minutes after GME bolus, but counts were higher compared to phase 1.
At the start of each repetition, flow was temporarily stopped to confirm that the EDAC™ was not reporting false positives due to improper contact between transducer and connector. Flow was then increased to 2 L/min, and phase 1 recording began. An intervention which mimics administration of a bolus of medication or blood sampling/flushing was performed for phase 2 in both groups. A GME emulsion was created by mixing a 10-mL bolus of air with either 10 mL of blood or glycerol between two 30-mL syringes (BD, Franklin Lakes, NJ, USA) connected via a stopcock (Braun Medical. Bethlehem, PA, USA). Ten milliliter of the resulting emulsion was introduced to the system via the GME injection port at a rate of 1 mL/s (Figure 1(c)). Once the emulsion was injected, phase 2 recordings began. Phase 3 recordings began 10 minutes after the GME injection. The end of phase 3 marked the end of the repetition.
After each repetition, the Luer ports on the ML were aspirated with a syringe to remove trapped GME. The system was left undisturbed with a flow of 2 L/min until the GME count decayed to under 2 emboli/s for both the pre- and post-ML channels. On average, this state was reached in 30 minutes. Another repetition was performed shortly thereafter (Table 1).
Table detailing the various phases of the repetitions of the experiment.

Statistical analysis
All data were exported and processed first in Excel (Microsoft, Richmond, WA, USA) and then SAS 9.3 (Cary, NC, USA). Using SAS, a two-sample test for equivalence was conducted comparing pre- and post-ML GME counts for each phase, followed by an independent variable test to compare between groups for each pre- and post-ML measurement at each GME size range. Values are reported as mean count ± SEM of GME measured within the diameter range bin identified. Tests were two-sided and significance was accepted at p < 0.05.
Results
GME were successfully detected in the Cardiohelp ECLS system with the EDAC. In the blood group, hematocrit was 30% ± 1% after transfer. We observed similar detection trends between blood and glycerol, with slight differences based on GME diameters. We observed changes in GME counts between pre- and post-ML detectors.
For phase 1 pre-ML (Figure 2(a)), GME were detected in all the diameter ranges for blood, and GME under 150 μm were detected in glycerol. We observed a trend toward higher GME counts with decreasing GME diameter. For phase 1 post-ML (Figure 2(b)), fewer GME across all diameters were detected in blood, with a similar trend in glycerol. The blood group showed higher GME in all size ranges versus glycerol, with most located in the 0–50 μm range (Figure 2(a) and (b)). There were no significant differences between pre- and post-ML GME counts within each group in Phase 1.
In phase 2, GME counts were detected in both groups and all reported size ranges (Figure 2(c) and (d)). GME counts were 10–100 times higher compared to Phase 1, for all ranges. For phase 2, pre-ML and post-ML blood and glycerol groups exhibited similar detection patterns, with slight differences for GME larger than 150 μm. In the blood group, GME counts were only significantly reduced between pre- and post-ML in the 0–50 μm size range. In the glycerol group, there was a significant decrease in GME counts between pre- and post-ML in diameter ranges larger than 50 μm.
In phase 3, GME were detected in both groups and all reported size ranges (Figure 2(e) and (f)). All GME counts were decreased compared to Phase 2 but were still higher than Phase 1. The blood group showed higher GME counts than the glycerol group for most of the ranges post-ML. For the blood group, there was no significant difference between pre-and post-ML GME counts outside the 10–50 μm range. For the glycerol group, was a significant decrease in all sizes >100 μm.
Discussion
The principal findings of the study are as follows. (1) With some exceptions, we documented similar GME formation dynamics and size distribution, in both blood and glycerol. (2) Injection of GME caused an increase in GME counts in both groups, but more so in blood. (3) There were significant, but varying, decreases in GME levels post membrane in both groups. (4) There were significant decreases in GME counts 10 minutes post injection of GME. We conclude that the EDAC™ is suitable for GME detection in the Cardiohelp system and that the Cardiohelp ML traps most GMEs in glycerol and GMEs under 50 μm in blood during in vitro testing at 2 L/min flow. 24 We also find that the ML reduces GME counts as the GME are introduced into the system, with further reduction over time.
Investigation of GME formation has historically been carried out in cardiovascular bypass systems and only recently been extended to new-generation ECLS devices used for treatment of ARDS. One such device, the Cardiohelp (Maquet/Getinge, Rastatt, Germany) ECLS system, is approved by the US Food and Drug Administration for treatment of cardiogenic shock, and is widely used internationally as an off-label treatment for refractory respiratory failure. 3 During transport of the critically ill, especially at high altitude, the problem of GME formation is likely underappreciated as it is; and is most likely only going to be exacerbated with increased utilization of ECLS. 24 To our knowledge, no study of GME formation dynamics during transport have been previously reported. This manuscript describes preliminary in vitro device testing prior to executing in vivo testing in simulated transport scenarios under hypobaric conditions. 25 We also build upon previous work by De Somer et al., and others who utilized blood surrogates for GME detection.22,26 The results from our study provide insight into the capabilities and limitations of the EDAC™ GME detector, GME formation in the Cardiohelp system during the initiation of ECLS therapy (Phase 1), operator interventions on an ECLS patient (Phase 2 and 3), and GME behavior in blood surrogates. We interpret changes between pre- and post-ML within each group as the ML’s ability to remove GME during a hypothetical single pass of blood. We interpret the changes between phase 2 and phase 3 as the ML’s ability to remove GME over a longer period of sustained flow.
What is the importance of detecting microbubbles in an ECLS system? It is well known that the infusion of a large volume of air into the circulatory system can lead to deadly, catastrophic results. 27 Most modern ECLS systems have a bubble detector to screen for and prevent the device from propagating large volumes of air; however, these systems do not detect small GMEs.
As proposed by Stehouwer et al., 28 some of the initial air release risk can be mitigated by a CO2 flush before priming. This approach would not counteract GME formation later during blood sampling and or flushes of saline back to patient during management. Under those conditions, utilization of air eliminating filters might be advisable. 29 In a clinical setting, effects of GME depend on multiple factors, including size, tissue location, clinical status of the patient, and other unknown factors. Studies have shown GME can cause lasting injury to an ECLS patient;9,30 although arterial air emboli could reach any organ, occlusion of cerebral and cardiac circulation is particularly deleterious because these organs are highly vulnerable to hypoxia and suffer irreversible cellular damage. 9
Curiously, in our in vitro model, we find that simply turning on the pump (as seen in Phase 1) can result in circulating GME. The only change to the system to precipitate this increase was an initiation of circulation; no exogenous GME were injected yet. Initiation of fluid flow may have released GME that were formed during ECLS circuit priming and attached to tubing and between the ML fibers.
As expected, for phase 2, injection of GMEs led to a large increase in GME counts in all groups. There was a decrease in GME counts between pre- and post- membrane lung in blood in the 10–50 μm diameter range. We suspect that the GME, particularly in this size range, were trapped within the ECLS membrane or were caught in the membrane air trap that is situated above and behind the membrane fibers. If our conjecture is correct, utilization of the Cardiohelp ML may present certain protective effects during GME formation but needs to be validated in subsequent translational studies involving trauma.
The phase 2 GME injection was designed to mimic provider interventions on an ECLS patient, such as drug or fluid bolus injections, blood draws, and flushing of lines or to model formation of GMEs during atmospheric pressure changes (e.g. during rapid aircraft depressurization). Of note, the Cardiohelp bubble alarm was never triggered. This is because the Cardiohelp bubble sensor is designed to detect emboli greater than 5 mm, 31 while the EDAC™ has a maximum range of 1000 μm. 23
The phase 3 results show a significant decrease in GME counts for all size ranges compared to phase 2, in both groups, 10 minutes after the GME bolus was injected. In both groups, larger decreases were observed in the larger size ranges; we believe that larger GME are more easily trapped by the system. In glycerol, GME counts decrease between pre- and post-membrane in GME diameters >100 µm. However, in blood we did not observe any significant decreases between pre- and post-membrane, which might be an important distinction between the two fluid groups.
In all of the phases for both groups, we observed similar inverse relationships between GME count and GME diameter; there was a higher concentration of small-diameter GME. We believe, and previous work confirms, 29 that formation of smaller diameter GME is more prevalent and shear stress from the pump breaks down large GME into smaller emboli.
One of our objectives was to compare and contrast blood and glycerol as a circulating fluid in this in vitro model. De Somer et al. concluded that the EDAC™ system suffered limitations when used for GME detection in “worst-case” scenarios, 22 thus this study was undertaken to confirm De Somer’s findings and validate the EDAC™ system in our laboratory prior to executing in vivo testing of GME formation under hypobaric conditions. 25
Significant differences in GME counts between blood and glycerol were visible during periods of low GME volumes (Phase 1 and Phase 3), and these differences appeared to diminish during periods of high GME presence in the circulating fluid (Phase 2). We suspect that differences in rheological properties; both the lower viscosity of the glycerol mix (1.852 mPa·s at 37°C 32 ) versus blood (3.5–4.5 mPa·s at 37°C 33 ), as well as the presence of microparticles in whole blood 33 would lead to variances in GME detection. In addition, the EDAC™ is calibrated for whole blood circulation, not for a simple glycerol-water mix. We caution in putting too much faith in experiments carried out using blood substitutes and recommend donor blood for future studies.
The results from this study should be interpreted in light of the following limitations: the in vitro nature of our experiment prevents direct translation into an in vivo setting. The EDAC™ detector is inaccurate at high flow rates (>5 L/min), during periods of high GME volume, and if GME are under 10 μm. 22 The overabundance of GME present in phases 2 and 3 were likely not accurately counted. In our study design, the EDAC™ counted all GME circulating in the system over a 3-minute period and it is possible that the GME were overcounted. Air eliminating filters would likely solve this limitation, however we decided to use manufacturer provided circuits to mirror the follow-on in vivo study and to standardize testing without additional modification of circuits.
Conclusion
We demonstrated feasibility and utility of GME detection in modern ECLS systems using both blood and a glycerol surrogate. Both injection of samples and flow dynamics can contribute to currently underappreciated levels of GME formation during ECLS, with the membrane lung acting as a trap for GME of most sizes. This GME detection approach laid the groundwork for in vivo studies using the Cardiohelp during ground and aeromedical evacuation at altitude levels relevant to transport of critically injured as well as healthy civilians, many of whom may not be purview to delayed mortality caused by GME formation during changes in altitude and microembolization of vessels potentially leading to organ damage.
Footnotes
Author’s Note
The opinions or assertions contained herein are the private views of the authors, and are not to be construed as official or as reflecting the views of the Departments of the Army, Air Force, or Defense.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.