
Abstract
Factor XII (FXII) deficiency presents as a prolonged activated partial thromboplastin time (aPTT) but is not associated with clinically significant bleeding. Activated clotting time (ACT) is used routinely to monitor anticoagulation with unfractionated heparin in patients undergoing cardiopulmonary bypass (CPB). The coagulation activator reagents in most ACT tests are dependent on adequate FXII concentrations to initiate contact factor coagulation pathways. We report the case of a 14.7 kg girl undergoing CPB with a pre-admission FXII concentration of <1% and aPTT >200 seconds. The child was transfused with fresh-frozen plasma to replenish FXII, allowing safe ACT monitoring of heparin anticoagulation throughout CPB.
Keywords
Introduction
Coagulation Factor XII (FXII) is produced and secreted by the liver. 1 After activation by intimal injury, it contributes to the intrinsic coagulation cascade by activating Factor XI (FXI). Deficiency of FXII is rare and is not associated with clinical bleeding due to the more dominant activation of FXI by thrombin during in-vivo coagulation. 2 FXII deficiency may be diagnosed incidentally during pre-operative assessment as prolonged activated partial thromboplastin time (aPTT). Contact activation based in-vitro diagnostic coagulation tests including aPTT and activated clotting time (ACT) utilise an activator reagent which initiates the contact pathway involving FXII.1,3–5 The baseline prolongation of ACT due to FXII deficiency makes heparin monitoring using ACT unreliable in patients with FXII deficiency undergoing cardiopulmonary bypass (CPB).
This report describes our stepwise approach to the perioperative management of a child with FXII deficiency undergoing CPB.
Case history
An otherwise healthy 14.7 kg 3-year-old girl presented for repair of sinus venous atrial septal defect with partial anomalous pulmonary venous return. During pre-operative workup, a prolonged aPTT of >200 seconds was discovered (ACL TOP series analyser, Hemosil APPT-SP reagent; Werfen Australia, NSW) which completely corrected to 34 seconds on mixing with normal plasma (Figure 1). The patient’s prothrombin time (12 seconds), thrombin time (16 seconds) and fibrinogen level (2.2 g/L) were normal. Further investigations revealed normal concentrations of coagulation factors VIII, IX, XI and von Willebrand factor; however, FXII concentrations were <1% (HemosIL Factor 12 deficient plasma, HemosIL APTT-SP reagent; Werfen Australia, NSW). Repeat testing on the day of surgery calculated a FXII level of 7% (Table 1).
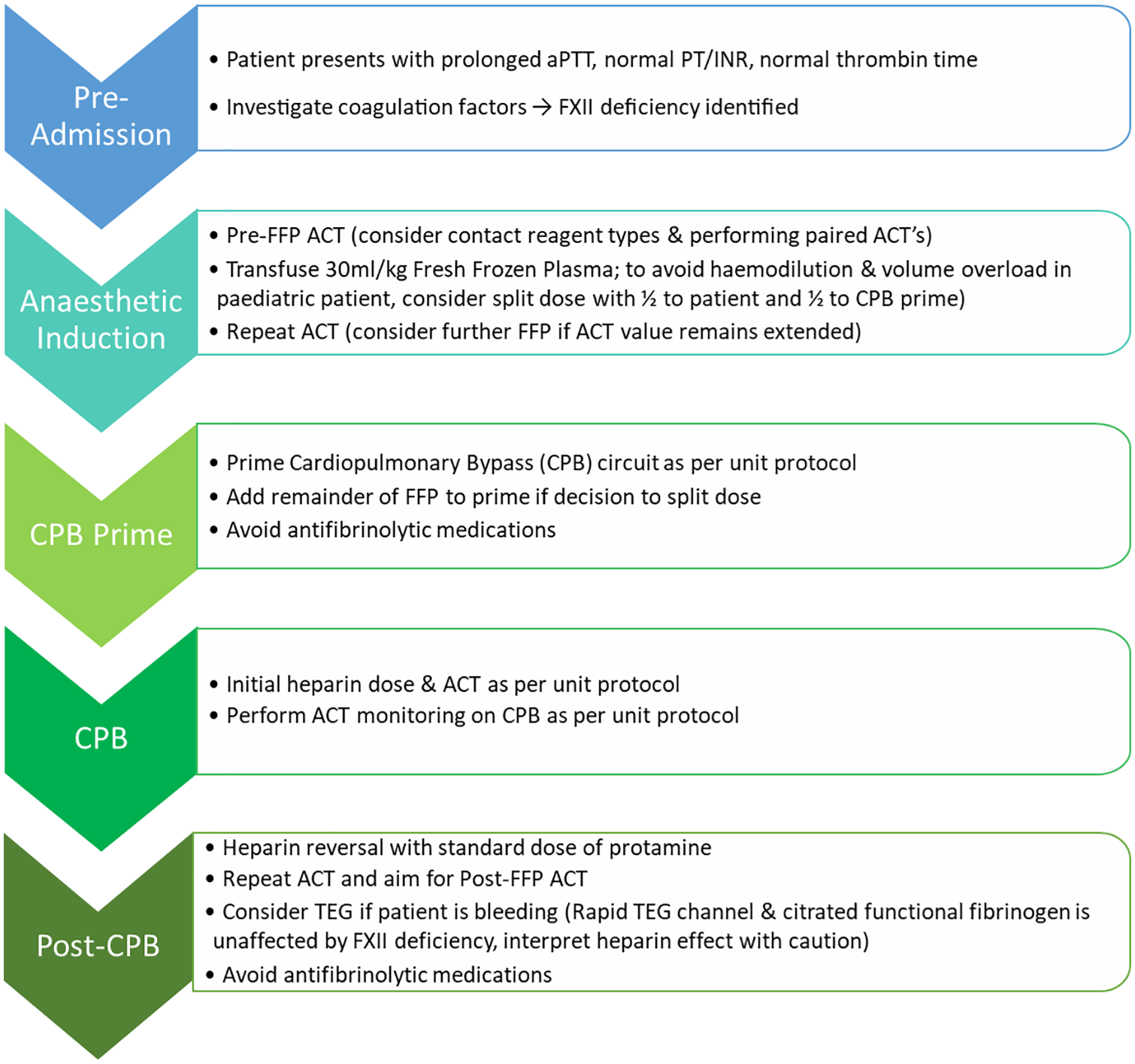
Workflow outlining identification and management of a paediatric patient with Factor XII deficiency.
Perioperative coagulation profile at progressive time points.
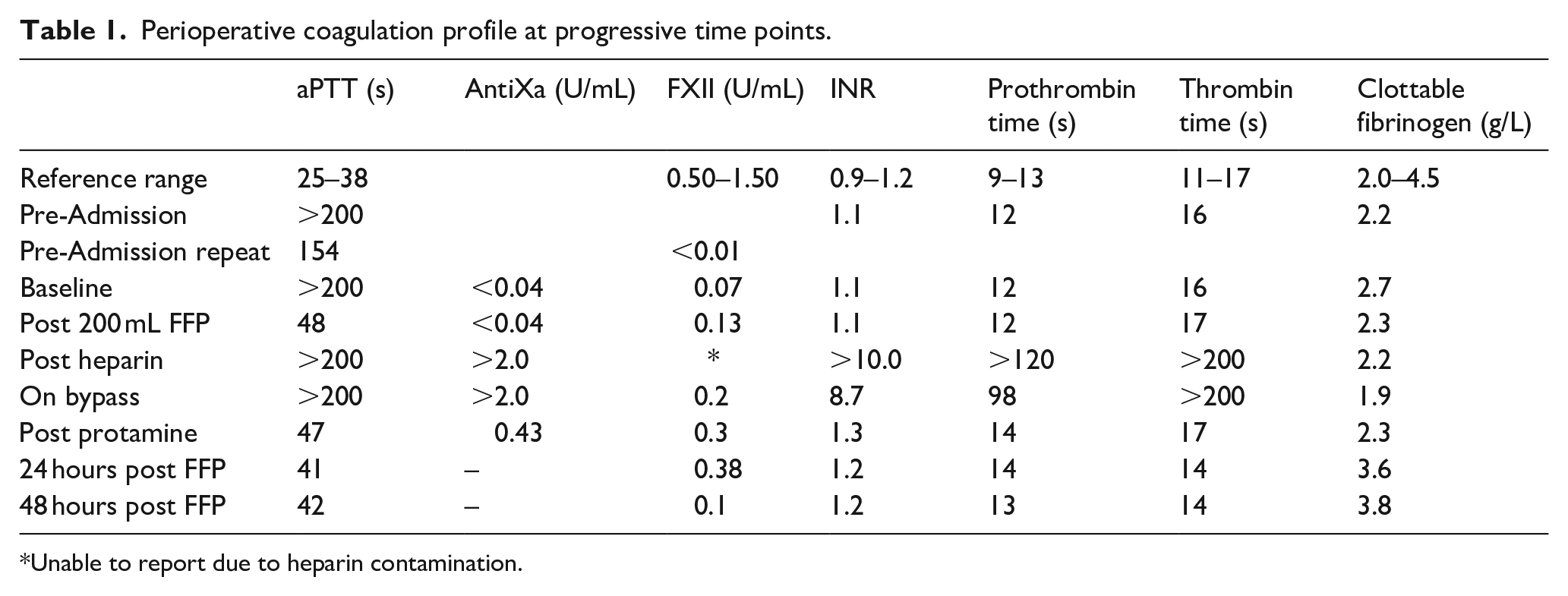
Unable to report due to heparin contamination.
Following a multidisciplinary review with haematology, a plan was established to perioperatively transfuse the child with 400 mL (~30 mL/kg) fresh-frozen plasma (FFP) to correct the ACT, similar to previously published reports.5–7
Baseline investigations were performed during standard anaesthetic induction (Table 1) and half the intended dose of FFP (200 mL, ~15 mL/kg) was transfused to partially replenish FXII while avoiding volume overload and haemodilution. The child was anticoagulated with a standard dose of heparin (400 IU/kg Heparin Sodium (porcine mucous); Pfizer Australia, NSW) and safely transitioned to CPB. Thromboelastography (TEG® 6s; Citrated, Haemonetics Corporation, Chicago, IL, USA) performed prior to FFP transfusion showed markedly prolonged R time (38 minutes) (Figure 2). The rapid TEG channel of this test uses kaolin, tissue factor and calcium chloride as activators. Following FFP transfusion, the R time decreased substantially (10.1 minutes).
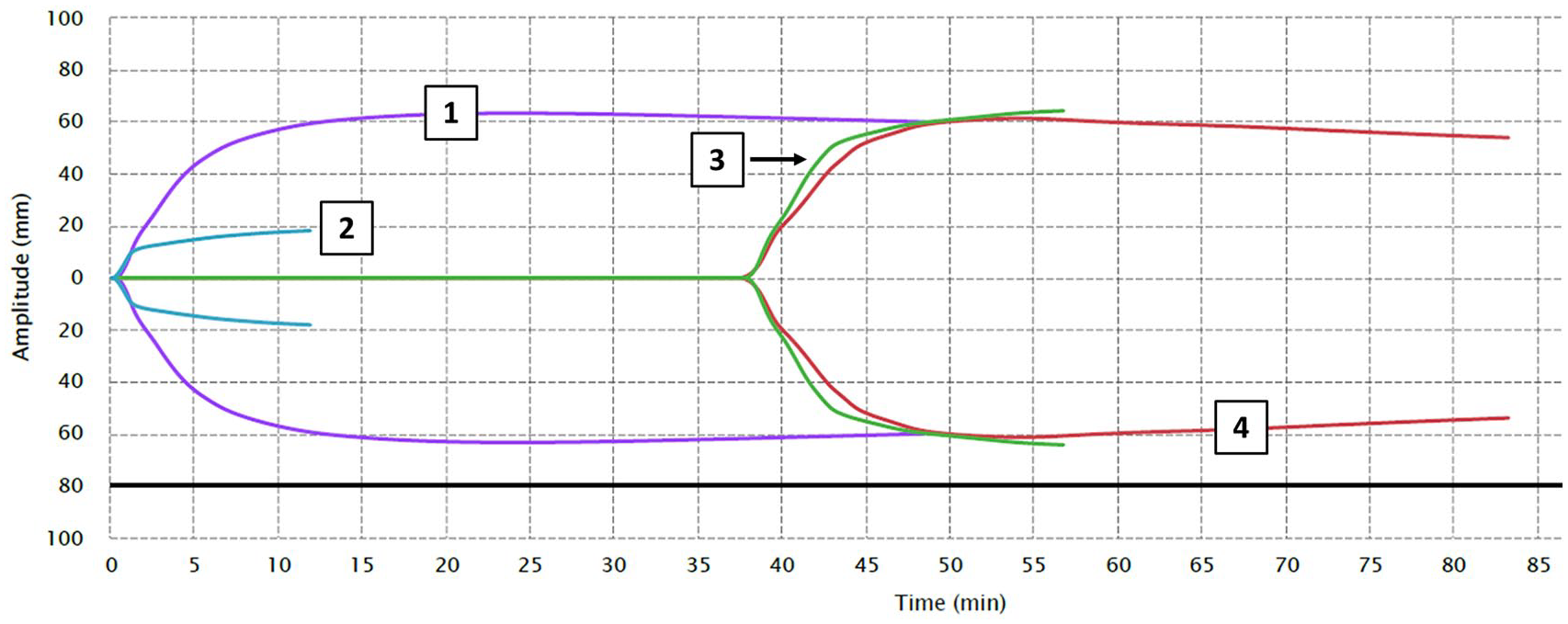
Baseline TEG showing marked prolongation of R time in both the citrate + kaolin and citrate + kaolin + heparinase channel.
The CPB circuit consisted of a Capiox® FX05 Baby-FX hollow fibre oxygenator (Terumo Corporation, Japan) and SMARxT® coated tubing (LivaNova, VIC). The circuit was primed with 200 mL FFP, 280 mL packed red blood cells (to account for haemodilution related to FFP transfusion), 1400 IU heparin, 70 mL Plasma-Lyte 148 (Baxter, NSW), haemofiltered to achieve a haematocrit of 28% and balanced with sodium bicarbonate and calcium chloride. The aortic cross clamp was applied for 13 minutes and total CPB time was 25 minutes. No further heparin was required during CPB and ACT (Hemochron Jr. Signature+, Werfen Australia, NSW) values remained within the desired range (Table 2).
Intraoperative activated clotting times on day of surgery.
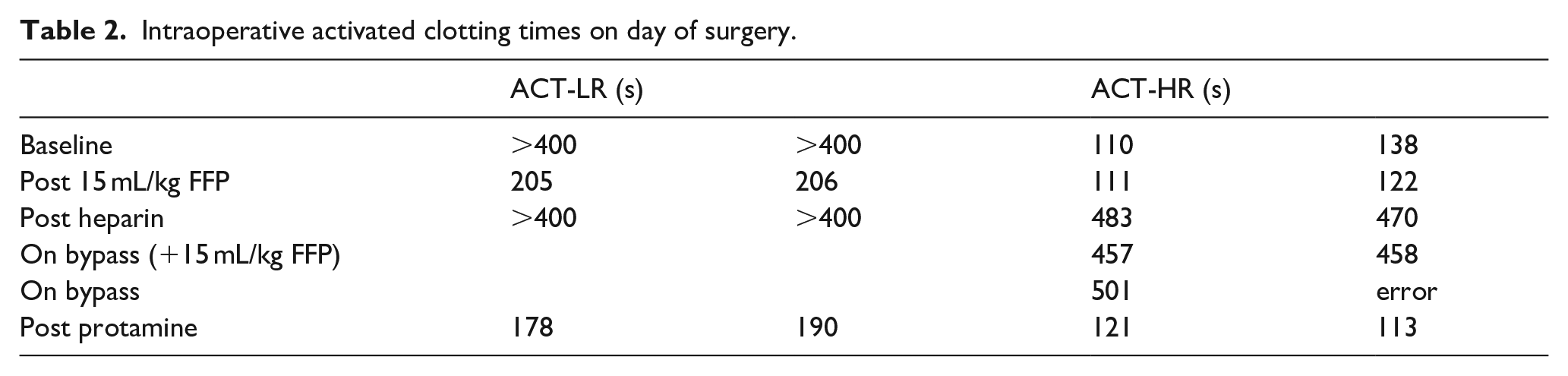
As an added precaution, paired ACT were performed at every time point due to the known variability in results (Table 2). ACT was also measured using two cartridge types; the low range (ACT-LR) cartridge (JACT-LR, Werfen Australia, NSW) comprised of a dried preparation of celite, potato dextrin, stabilisers and buffers and is suitable for heparin concentrations up to 2.5 i.u./mL of blood and the high range (ACT-HR) cartridge (JACT+, Werfen Australia, NSW) which comprised of a dried preparation of silica, kaolin, phospholipid, stabilisers and buffers and is suitable for heparin concentrations of 1 to 6 i.u./mL of blood (Werfen Australia, NSW).
After weaning from CPB, modified ultrafiltration was completed and protamine reversal of heparin (60 mg Protamine Sulphate (Salmon) injection 1%; Sanofi, AUS) returned the ACT to baseline. There was no unusual bleeding and haemostasis was straightforward. The R time was 10.7 minutes (reference range 4.5 to 9.1 minutes; TEG® 6s; Citrated, Haemonetics Corporation, Chicago, IL, USA). There was no significant haemorrhage in the post-operative period. FXII levels remained low when measured at 24- and 48-hours post FFP, and the child was discharged uneventfully on postoperative day four (Table 1).
Discussion
In our case, FXII deficiency was detected during routine pre-operative workup. It interferes with traditional anticoagulation management strategies using ACT measurement during CPB. Previous reports have described a variety of techniques for managing anticoagulation of FXII deficient patients undergoing CPB. Reports of empiric heparin dosing without anticoagulation monitoring or by observing for visible clot in-vitro without anticoagulation monitoring presented an unacceptable risk to our patient.6,8–10 Similarly, in a paediatric patient with severe FXII deficiency, heparin concentration was monitored without measurement of heparin response. 7 Alternatively, modification of the ACT using in-vitro donor FFP and calcium has been described in the FXII deficient patient, though this technique induces haemodilution and does not accurately reflect the composition of plasma circulating in the extracorporeal circuit.11,12 Heparin resistance or antithrombin III deficiency may also be concealed by this method. Preservation of the extracorporeal circuit during CPB is critical. Thus, we made the decision to replace FXII by transfusing FFP prior to surgery. Our approach was consistent with techniques previously reported, allowing for direct measurement of heparin induced anticoagulation rather than an assumption of anticoagulation.5,13,14
On the other hand, thrombin time is unaffected by alterations in the intrinsic and the extrinsic coagulation pathway but reflects heparin effect via the common pathway of the coagulation cascade. Thrombin time reflected the baseline, heparin effect and protamine reversal and was not altered by FXII levels in our patient (Table 1). The use of chromogenic anti-Xa assay to monitor anticoagulation has also been described; however, protamine reversal is less reliably measured because protamine completely neutralises the anti-IIa activity of heparin but not anti-Xa activity. Both thrombin time and anti-Xa assays are unable to be used as point of care tests and are not currently standardised for CPB.11,15
In our case, ACT-HR provided appropriate results pre- and post-FFP transfusion, tracked thrombin time at all stages of surgery and correctly reflected the state of heparinisation without being affected by FXII deficiency. Negatively charged surface activators such as kaolin, celite, dextran sulphate and sulphatides are known to be strong stimulants of the activation of FXII by kallikrein. 16 Kaolin and negatively charged silica are present in the ACT-HR cartridge but absent in the ACT-LR, which contains celite. It is possible that the patient had sufficient residual FXII activity to elicit clot formation in the presence of both kaolin and silica. This was unexpected and in retrospect it would have been beneficial to delay FFP transfusion until after heparinisation to observe a change in ACT-HR.
One other option is to use confirmation of a normal antithrombin level in combination with kaolin ACT monitoring and maintain the target heparin concentration using heparin-protamine titration. 17 However, while heparin-protamine titration indicates the presence of heparin, it does not indicate a heparin response. Both tests are not commonly available as point-of-care tests. Additionally, the use of ACT alone remains the most commonly utilised method to monitor anticoagulation with heparin during cardiopulmonary bypass and in this sense our approach is low-risk and avoids utilising an unfamiliar strategy. 18
FXII levels have not been previously reported over a 48-hour period following FFP transfusion in a severely deficient patient (Table 1). The half-life of FXII is 40 to 50 hours. 3 Heparin contamination and dilution whilst on CPB distorts FXII levels post-heparin and on CPB and these results should be interpreted with caution. Burman et al. 7 have previously reported a 12-year-old child with FXII <1% though they did not monitor heparin response.
There are two reports of thrombosis following antifibrinolytic administration in FXII deficient patients.3,19 Our patient did not receive any antifibrinolytic medication during her admission.
In conclusion, FXII deficient patients requiring CPB can be safely managed by perioperative transfusion with FFP. This is a simple and effective method, allowing anaesthesia and surgery to proceed in an otherwise standard fashion. We recommend using ACT-HR pre- and post-FFP transfusion as it utilises kaolin and silica as contact reagents and is more reliable in the presence of FXII deficiency.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics statement
This case report was written with the approval of the Children’s Health Queensland Hospital and Health Service Human Research Ethics Committee.
Informed consent
Written informed consent was obtained from the child’s mother and father.