
Abstract
Anterograde or retrograde cerebral perfusion can protect the brain from ischemic injury during hypothermic circulatory arrest (HCA), but neither type of perfusion provides blood flow to the abdominal viscera. Here, we report a modified retrograde cerebral perfusion (RCP) technique in which we tethered both superior and inferior venae cavae with bands around the cannula and clamped the distal ends of the drainage tubes of both venae cavae. Modified RCP may provide greater blood flow to the brain and lower body than conventional RCP during HCA in hemiarch surgery.
Introduction
Hypothermic circulatory arrest (HCA) is necessary to provide a clear surgical field for aortic arch replacement. During circulatory arrest, applying anterograde or retrograde cerebral perfusion (RCP) can attenuate ischemic injury to the brain. 1 However, neither type of perfusion provides blood flow to the lower body. Here, we describe a modified retrograde cerebral perfusion (mRCP) technique that may perfuse the brain and abdominal organs during HCA.
Methods
Between 28 February 2021 and 30 June 2021, mRCP was performed in 8 male patients (64 ± 6 years old) suffering from acute type A aortic dissection who were scheduled for hemiarch replacement surgery (HRS). This study was approved by the Medical Ethics Committee of West China Hospital, Sichuan University (No. 2018(24)). Written informed consent was obtained before surgery from all patients. We routinely monitored arterial blood pressure, central venous pressure, bilateral regional cerebral oxygen saturation, and nasopharyngeal and rectal temperature. A standard cardiopulmonary bypass circuit was set up. After the oxygenator, the arterial line was bifurcated into one branch for systemic perfusion, and another branch was connected to the superior vena caval drainage tube in order to prepare for mRCP during HCA (Figure 1(a)).
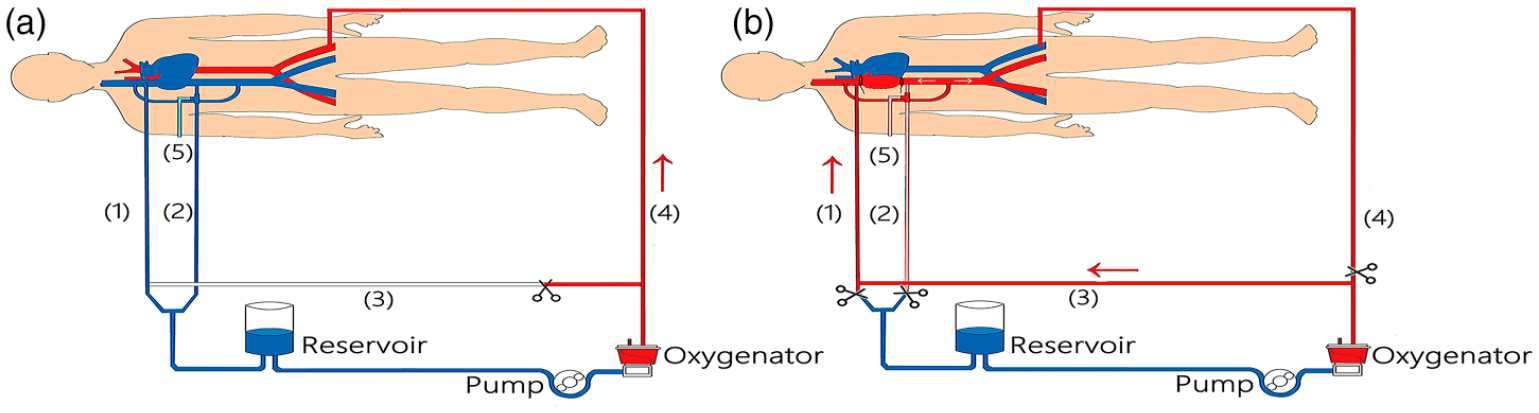
Schematic of the cardiopulmonary bypass and its connection with the body. (a) Before and after modified retrograde cerebral perfusion (mRCP), venous blood returns from the (1) superior vena cava and (2) inferior vena cava to the blood reservoir, then it is pumped into the oxygenator and then back to the artery via the (4) arterial tube. Inferior vena cava pressure is monitored via a (5) side opening of cannulation. The communicating branch between the arterial line and superior vena caval drainage tube is clamped. (b) During mRCP, the branch for systemic perfusion and the distal ends of both superior and inferior vena caval drainage tubes are cross-clamped, and the (3) communicating branch between the arterial line and superior vena cava drainage tube is opened. The oxygenated blood is routed as in RCP, while the other part of the blood comes to the lower body via the communicating branch between superior and inferior venae cavae in order to perfuse the vital organs in the lower body.
After sternotomy and systemic heparinization, cardiopulmonary bypass was set up by placing a cannula in the femoral artery, and single cannulae were inserted into the superior and inferior venae cavae. During bypass, the communicating branch between the arterial line and superior vena caval drainage tube was clamped. After achieving moderate hypothermia (nasopharyngeal temperature, 25°C; rectal temperature, 27°C), the pump was stopped, and both the superior and inferior venae cavae were snared with bands around the cannulae. The branch for systemic perfusion and the distal end of the superior vena caval drainage tube were cross-clamped, but the communicating branch between the arterial line and superior vena caval drainage tube was opened, then the pump was restarted as in RCP. In the mRCP, however, the distal end of the inferior vena caval drainage tube was cross-clamped to prevent blood in the inferior vena cava from flowing into the reservoir (Figure 1(b), Video). A small-bore drainage tube was inserted through the descending aorta to drain blood flowing back from collaterals in order to ensure a clear surgical field during distal anastomosis.
Results
During mRCP, retrograde perfusion flow was maintained at 3.8 ± 1.8 mL min−1 kg−1 to keep central venous pressure at 21 ± 2 mmHg (Figure 2), and regional oxygen saturation(rSO2) decreased by less than 10% of baseline. Pressure in the inferior vena cava, which was measured via the side opening of the cannula, increased to 11 ± 3 mmHg.
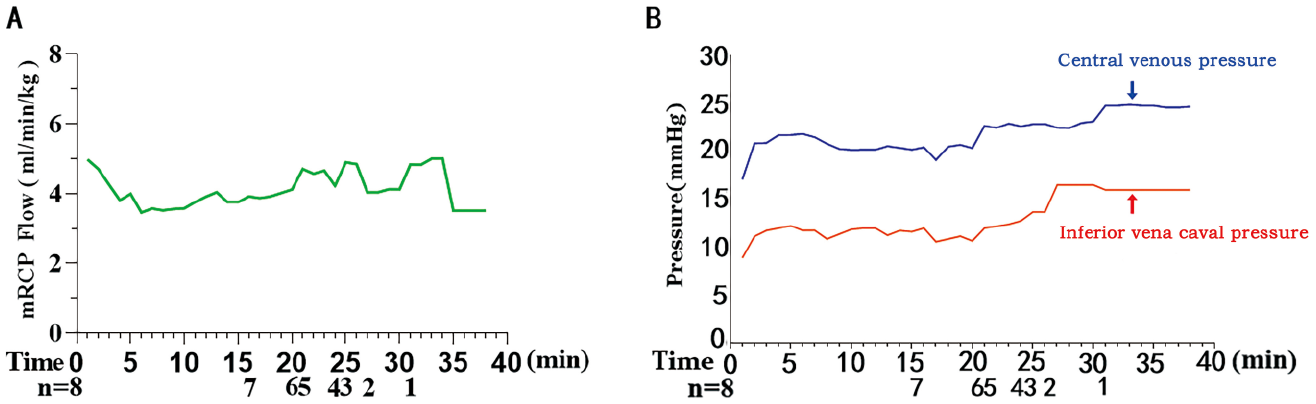
Blood flow and pressure during modified retrograde cerebral perfusion. (a) Blood flow rate. (b) Pressures in the central line and inferior vena cava.
Blood flow in the brain, liver, and kidney was observed during mRCP (Figure 3). Removal of the cross-clamp of the distal end of the inferior vena caval drainage tube eliminated blood flow in the liver and kidney, while cerebral blood flow decreased from 21.5 to 16 cm sec−1.
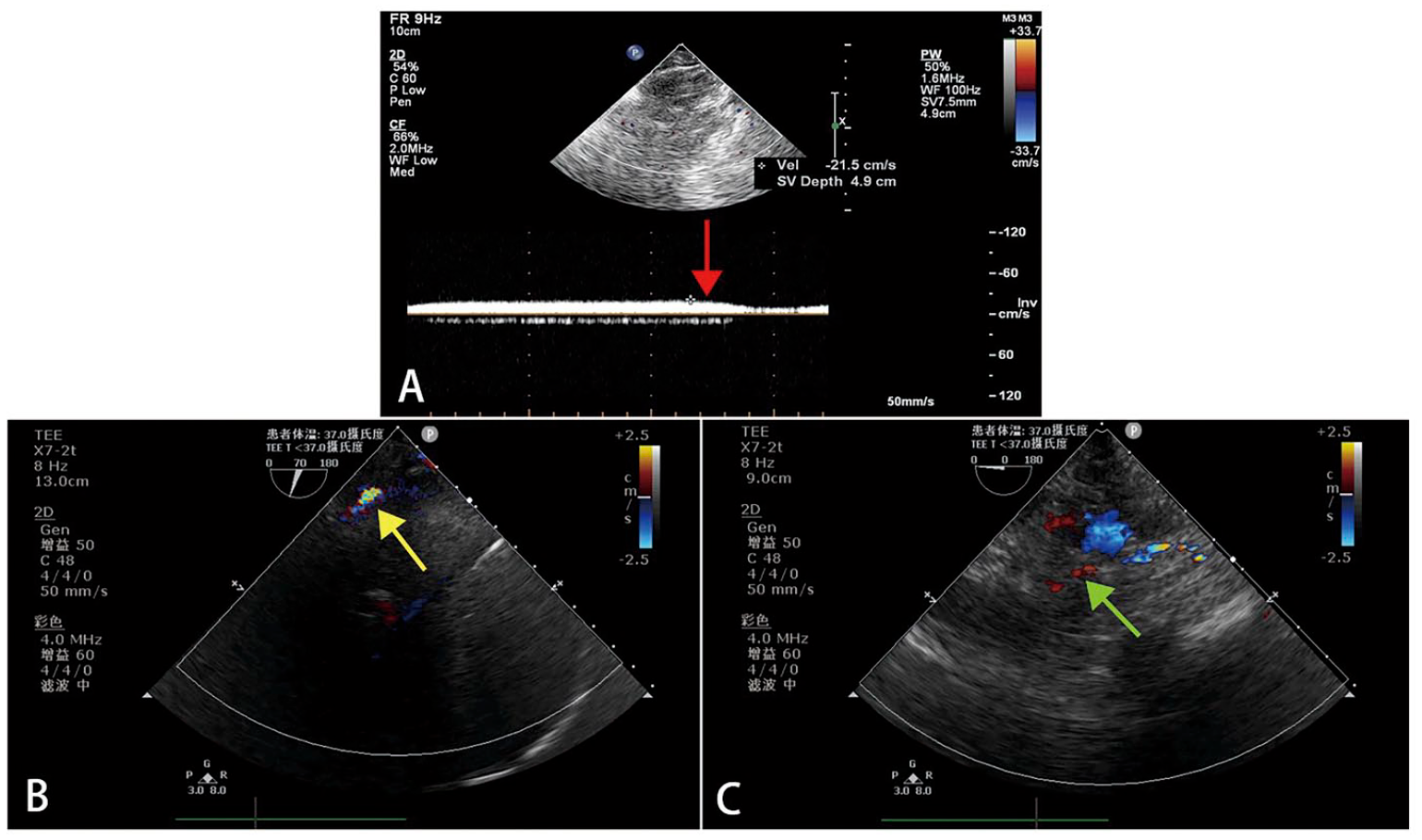
Observation of blood flow to the brain and visceral organs during mRCP. (a) Cerebral blood flow was 21.5 cm/sec based on transcranial Doppler ultrasonography during mRCP, and it decreased to 16 cm/sec after the distal end of the inferior vena caval drainage tube was unclamped (red arrow). (b–c) Blood flow was observed in the (b) hepatic vein (yellow arrow) and (c) renal artery (green arrow) using transesophageal echocardiography. mRCP, modified retrograde cerebral perfusion
Desaturated blood was observed in the aorta throughout mRCP, and a flexible sucker was inserted into the descending aorta to drain blood back into the reservoir. After end-to-end anastomoses between the graft and descending aorta, mRCP was stopped, and the communicating branch between the arterial line and superior vena caval drainage tube was cross-clamped again. Then the clamps on the arterial line as well as distal ends of the superior and inferior vena caval drainage tubes were removed, which restarted systemic perfusion from the femoral artery.
The mRCP procedure lasted an average of 24 ± 7 min, and intubation lasted an average of 15 ± 8 h. All patients recovered uneventfully and none suffered neurological complications, paraplegia, or liver dysfunction. Only one patient had mild acute kidney injury. All were discharged an average of 7.5 ± 1.4 days after surgery.
Discussion
After the widespread use of anterograde or retrograde cerebral perfusion to protect the brain during aortic arch replacement surgery, researchers have focused on how to minimize ischemic injury to the lower body during the operation. We reported that anterograde cerebral perfusion combined with retrograde inferior vena caval perfusion provides continuous blood flow to the brain, abdominal viscera, and spinal cord during HCA.2–4 However, this technique requires cross-clamping three arterial branches of the aortic arch, which is unnecessary during HRS. Another option is total venous retrograde perfusion,5,6 but this is unsafe for hemiarch surgery because it can lead to severe fluid retention and decreased rSO2. 7
Here, we describe a modification of RCP for total body perfusion. Blood from the upper body enters the lower body via the azygos, hemiazygos, and pericardiophrenic veins. In our patients, pressure in the inferior vena cava increased within 1 min after the inferior vena cava was tethered and the end of its drainage tube was cross-clamped. This pressure remained stable at 11 mmHg while blood flowed into the liver and kidney. These observations suggest that mRCP can effectively perfuse the lower body. We believe that this technique may be useful in various types of surgery involving prolonged clamping of the inferior vena cava.
Conventional RCP is thought to provide adequate blood to the brain only if the central venous pressure reaches approximately 31 mmHg, which is higher than the maximal safe limit of 25 mmHg. 8 Our experience is that removing the drainage cross-clamp of the inferior vena caval tube sharply reduces both central venous pressure and cerebral blood flow. This presumably reflects the shunting of cerebral blood flow via communicating branches between the superior and inferior venae cavae. This may explain, at least partly, why conventional RCP cools neurocytes but does not provide them with oxygen. In our modified procedure, rSO2 remained within the normal range throughout arrest, and no postoperative neurologic complications occurred, even though nasopharyngeal temperature was maintained at 25°C. These findings suggest that mRCP provides substantial blood flow to the brain.
The mRCP technique differs from total-body retrograde perfusion because the blood level in the reservoir remains stable. None of the eight patients that we treated suffered fluid retention or injury to vital organs, suggesting that mRCP is safe.
Conclusions
Our experience with this case series suggests that the mRCP procedure may provide more blood flow to the brain and lower body than conventional RCP during HCA in HRS. Further studies are needed to test whether the new technique is safe during total aortic arch surgery, and whether it improves surgical outcomes.
Footnotes
Appendix
Acknowledgements
We thank A. Chapin Rodríguez (Creaducate Consulting GmbH, Munich, Germany) for linguistic assistance.
Author contributions
XY, JL, and LD conceived and designed the study as well as drafted the manuscript. XJY and XLL helped conduct the study, XLL helped collect data, and ZCT prepared the video. LD revised the manuscript with input from all authors. The final version was approved by all authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the “1.3.5 Project for Disciplines of Excellence” (ZY2016101) at West China Hospital, Sichuan University
Ethics approval
The study protocol and informed consent form were reviewed and approved by the Ethics Committee of West China Hospital (No.2018(24)).
Consent for publication
Approximately 1 day before surgery, each participant was informed of the study design and purpose, interventions, and assessments. All participants provided written informed consent before enrolment.
Availability of data and material
The data used and analyzed during the current study are available from the corresponding author upon reasonable request.