
Abstract
Objectives
The optimal method for monitoring of anticoagulation in patients on extracorporeal life support (ECLS) is unknown. The objective of this study was to assess the relationship between anti-factor Xa level (anti-Xa; IU/mL) and activated partial thromboplastin time (aPTT; seconds) for monitoring intravenous unfractionated heparin anticoagulation in adult ECLS patients.
Methods
Charts of all adult patients cannulated for ECLS from 2015 through 2017 were reviewed and laboratory and heparin infusion data were extracted for analysis. Time matched pairs of anti-Xa and aPTT were considered concordant if both laboratory values were within the same clinically utilized range. A hierarchical logistic regression model was used to determine factors associated with discordance while accounting for patient level effects.
Results
A total of 1016 paired anti-Xa and aPTT values from 65 patients were evaluated. 500 (49.2%) paired samples were discordant with a degree of variability on linear regression (r 2 = 0.315). The aPTT fell into a higher therapeutic range compared to the anti-Xa in 31.6% and lower in 17.3%. Logistic regression demonstrated that discordance was independently associated with time from initiation of ECLS (OR 1.17 per day, p < 0.001), average heparin infusion rate (OR 1.25 per U/kg/hr, p < 0.001), and INR (OR 3.22, p < 0.001).
Conclusions
Nearly half of all aPTT and anti-Xa values were in discordant ranges and discordance is more likely as the time on ECLS and the INR level increase. The use of either assay in isolation to guide heparin anticoagulation may lead to misestimation of the degree of anticoagulation in complex ECLS patients.
Introduction
Extracorporeal life support (ECLS) is a temporary circulatory support technique for refractory cardiac, respiratory, or cardiopulmonary failure. Although greater experience and advances in technology have led to an increase in the use of ECLS, morbidity and mortality remain high.1–7 Much of the risk to patients can be attributed to the severity and complexity of the underlying disease process, but approximately 50% of patients experience hemorrhagic or thrombotic complications while receiving ECLS. 4 ECLS is thrombogenic secondary to the inflammatory cascade induced as blood comes into contact with non-epithelialized artificial surfaces of the circuit and experiences sheer stress from pump flow. 5 Because of the shift to a hypercoagulable state, the Extracorporeal Life Support Organization (ELSO) recommends anticoagulation therapy to minimize clot formation in the ECLS circuit. 8 Therein lies a delicate balance between ensuring adequate inhibition of platelet and coagulation factor activation to prevent circuit clot and maintaining sufficient endogenous procoagulant activity for hemostasis. The challenge to establish and maintain this balance results in the considerable burden of hemorrhagic and thrombotic complications.
Unfractionated heparin infusions are commonly used in ECLS patients, but the optimal method for titration and monitoring of heparin anticoagulation is unknown. ELSO guidelines suggest the use of multiple concurrent monitoring modalities but leave the specifics of titration strategies to the individual institution to determine. 8 Surveys of ECLS centers have shown that the activated clotting time (ACT) and activated partial thromboplastin time (aPTT) are used most often, but titration and monitoring practices vary widely among centers.9–11 The anti-factor Xa (anti-Xa) level assay serves as a direct measure of heparin effect and is often used in conjunction with the ACT or aPTT in ECLS patients.9–11 While there exists no consensus regarding the clinical superiority of anti-Xa versus aPTT assays for heparin titration, several studies in non-ECLS patients have demonstrated that aPTT and anti-Xa values are often discordant.12,13 Titration of heparin using anti-Xa are sometimes favored due to the biologic and pre-analytic factors which can influence the aPTT independent of the effects of heparin.14,15 The objective of this study was to assess the relationship between anti-factor Xa level and aPTT for monitoring intravenous unfractionated heparin anticoagulation in adult ECLS patients. We hypothesized that there would be a high degree of variability and discordance between assays.
Patients and methods
A-subjects
The University of Virginia Institutional Review Board approved this study and waived individual consent (IRB# 23,305). Patient data was reviewed from the University of Virginia institution’s adult ECLS data repository between 1 January 2015, and 31 October 2017. All patients were managed according to institutional ECLS guidelines which specify management of anticoagulation, circuit monitoring, and safety checks. Patients were excluded from this study if they received ECLS for less than 24 h, did not receive a continuous heparin infusion, were anticoagulated with bivalirudin, or underwent multiple separate ECLS runs. Laboratory and heparin infusion data from electronic health records were extracted for all patients who met criteria for analysis. Patient demographic data and details of ECLS were collected from the data set.
B-anticoagulation titration
At the time of cannulation, all patients received a bolus of unfractionated heparin. The heparin bolus dose was dependent on the patient’s risk for bleeding, as determined by the cannulating surgeon, or presence of active bleeding. Those at risk for bleeding received a heparin bolus of 25 units/kg and those not at risk received a bolus of 50 units/kg. ACT monitoring was used during cannulation to monitor anticoagulant effect. Additional bolus doses were given if the ACT failed to increase >160 s in bleeding patients and >200 s in non-bleeding patients. Per institutional guidelines a continuous heparin infusion was initiated post cannulation when the ACT level was <200 s, there was no clinical evidence of bleeding, and deemed clinically safe by the ECLS physician. Two heparin titration guidelines for ECLS dependent on a patient’s risk for bleeding were used. Those considered at high relative risk for bleeding or who had evidence of active bleeding were started on a low continuous infusion of heparin of 3 units/kg/h. When deemed clinically safe by the ECLS physician, the infusion was titrated per institutional guidelines to a maintain the anti-Xa level between 0.3 and 0.5 international units per milliliter (IU/mL). Those not considered at risk of bleeding were started at a heparin infusion of 7 units/kg/h and titrated per the guideline to achieve an anti-Xa level of 0.5–0.7 IU/mL. The aPTT was checked in tandem with the anti-Xa but did not influence titration given the bedside nurse driven anti-Xa based nomogram. During the first 48 h of ECLS, blood samples were sent for laboratory analysis every 4 hours and then changed to every 6 hours thereafter once stable on support. Laboratory data included date and time stamped aPTT, anti-Xa, international normalized ratio (INR), fibrinogen, antithrombin III function, hemoglobin, and hematocrit. Extracted heparin infusion data included instantaneous weight-based heparin infusion rate for every time point while on ECLS. The cumulative average heparin infusion rate was calculated as the total heparin infused divided by the hours since initiation of ECLS.
C-evaluation of concordance
Concordance and discordance were defined according to the institutionally established, clinically utilized goal ranges for aPTT and anti-Xa. Simultaneously drawn aPTT and anti-Xa pairs were considered concordant if both laboratory values fell within the same respective clinically utilized range: the subtherapeutic range was <50 s for the aPTT and <0.3 IU/mL for the anti-Xa; the therapeutic range for high bleeding risk patients was 50–70 s for the aPTT and 0.3–0.5 IU/mL for the anti-Xa; the therapeutic range for low or normal bleeding risk patients was 70–90 s for the aPTT and 0.5–0.7 IU/mL for the anti-Xa; and the supratherapeutic range was >90 s for the aPTT and >0.7 IU/mL for the anti-Xa. Paired lab draws were considered discordant if laboratory values fell into different clinically utilized ranges. Discordance was further classified as to whether the aPTT fell into a range which indicated a greater degree of anticoagulation compared to that indicated by the anti-Xa (aPTT > anti-Xa) or vice versa (anti-Xa > aPTT). The number and percent of concordant and discordant pairs were determined. We used hierarchical logistic regression models to determine factors associated with discordance while accounting for patient level effects. Fixed patient effects included age, sex, body surface area, type of ECLS (venoarterial vs venovenous), and whether the patient had an implantable ventricular assist device. Repeated measures included average heparin infusion rate, fibrinogen level (mg/dL), international normalized ratio, and time from ECLS initiation to laboratory blood draw.
D-statistical analysis
For reported demographics and outcomes, continuous variables were expressed as mean with standard deviation if normally distributed or as median with interquartile range if non-normally distributed. Normality was universally assessed with the Shapiro-Wilk test given the number of observations were always below 2000. Associations between continuous variables were assessed with the nonparametric Wilcoxon signed-rank test. Categorical measures were expressed as frequencies and percentages and analyzed with χ2 or Fisher exact test as appropriate. Bivariate linear regression analysis was used to assess the relationship between heparin infusion rate and both aPTT and anti-Xa as well as between aPTT and anti-Xa. The coefficient of determination (r 2 ) was calculated to estimate the proportion of variation in aPTT or anti-Xa attributable to the heparin infusion rate as well as the proportion of variation in aPTT that could be attributed to anti-Xa. We reported odds ratios with 95% confidence intervals for the parameter estimates generated from our hierarchical logistic regression model. Statistical significance was established at p < 0.05. Analysis was performed with SAS version 9.4 (SAS Institute, Cary, NC).
Results
A-study population and patient characteristics
Patient characteristics.
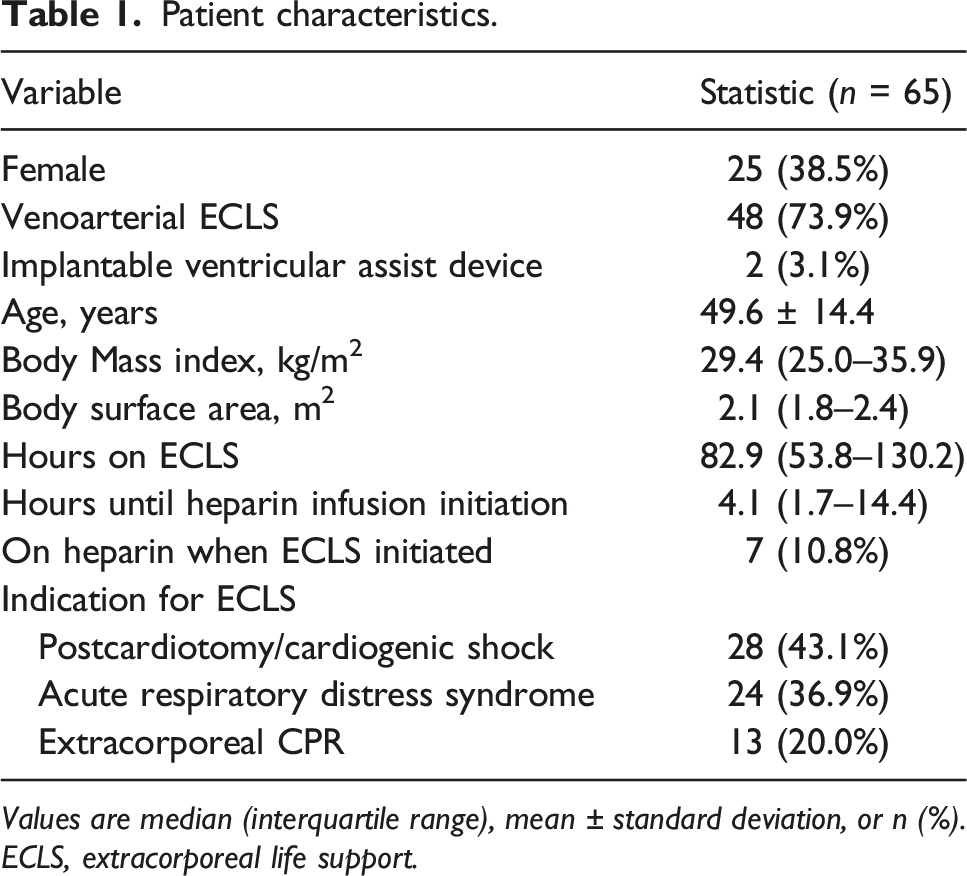
Values are median (interquartile range), mean ± standard deviation, or n (%). ECLS, extracorporeal life support.
B-anticoagulation monitoring
Heparin laboratory monitoring during extracorporeal life support.
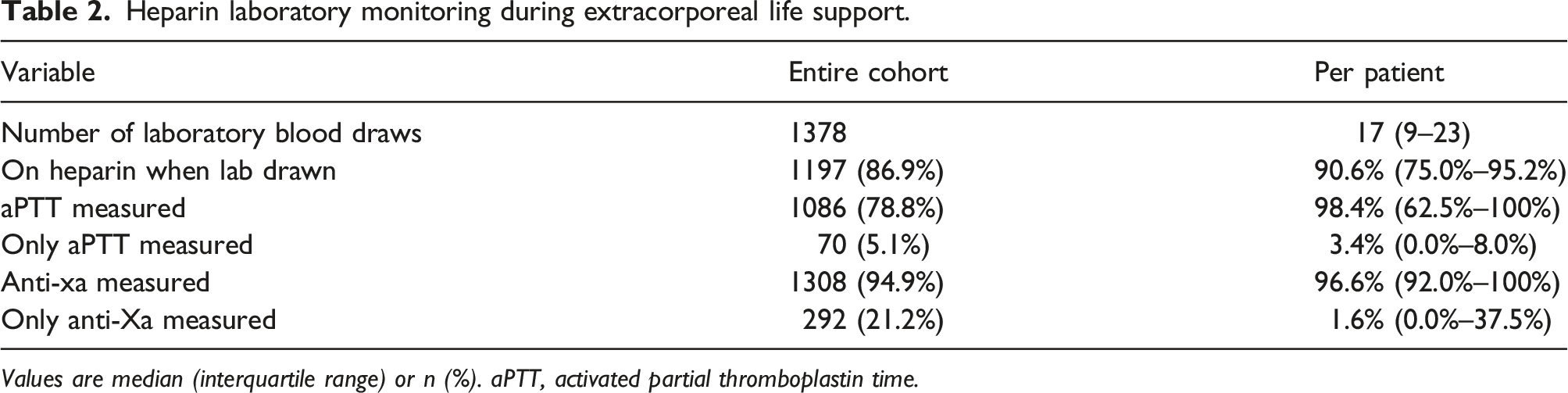
Values are median (interquartile range) or n (%). aPTT, activated partial thromboplastin time.
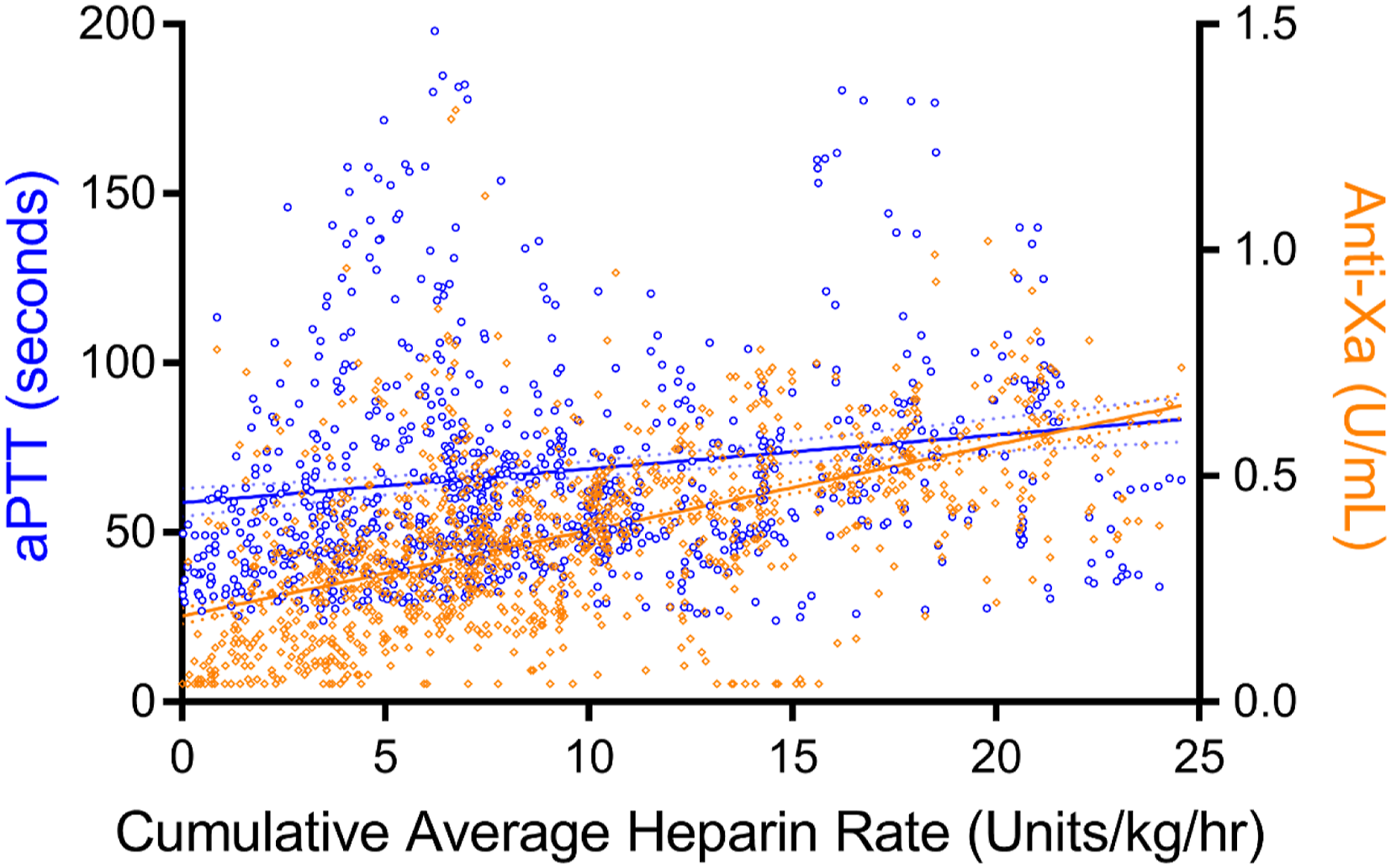
Plots and linear regressions of aPTT and anti-Xa lab values versus average heparin infusion rate. (Blue = aPTT, linear regression line with 95% CI, r2 = 0.025; Orange = anti-Xa, linear regression line with 95% CI, r2 = 0.298).
C-aPTT and anti-Xa concordance
Simultaneous measurements of aPTT and anti-Xa were performed in 73.7% samples with a median of 12 per patient (IQR 7–21 per patient). Among the 1016 paired samples, 500 (49.2%) were discordant with a median of 42.9% of samples per patient (IQR, 18.7%–67.7%). The aPTT fell into a range which indicated a greater degree of anti-coagulation compared to that indicated by the anti-Xa in 323 (31.8%) paired samples with a median of 20.7% (IQR, 0.0%–58.5%) of samples per patient. The anti-Xa fell into a range which indicated a greater degree of anti-coagulation compared to that indicated by the aPTT in 177 (17.4%) paired samples with a median of 0.0% (IQR, 0.0%–20.0%) of samples per patient (Figure 2). Linear regression analysis of the relationship between aPTT and anti-Xa among paired samples demonstrated an r
2
of 0.315. Plot of paired aPTT and anti-Xa lab values. (Dotted lines = limits of clinically utilized laboratory ranges; unshaded area = aPTT and anti-Xa indicate concordant clinical management; blue shaded area = aPTT indicates greater degree of anticoagulation compared to that indicated by anti-Xa; orange shaded area = anti-Xa indicates greater degree of anticoagulation compared to that indicated by aPTT).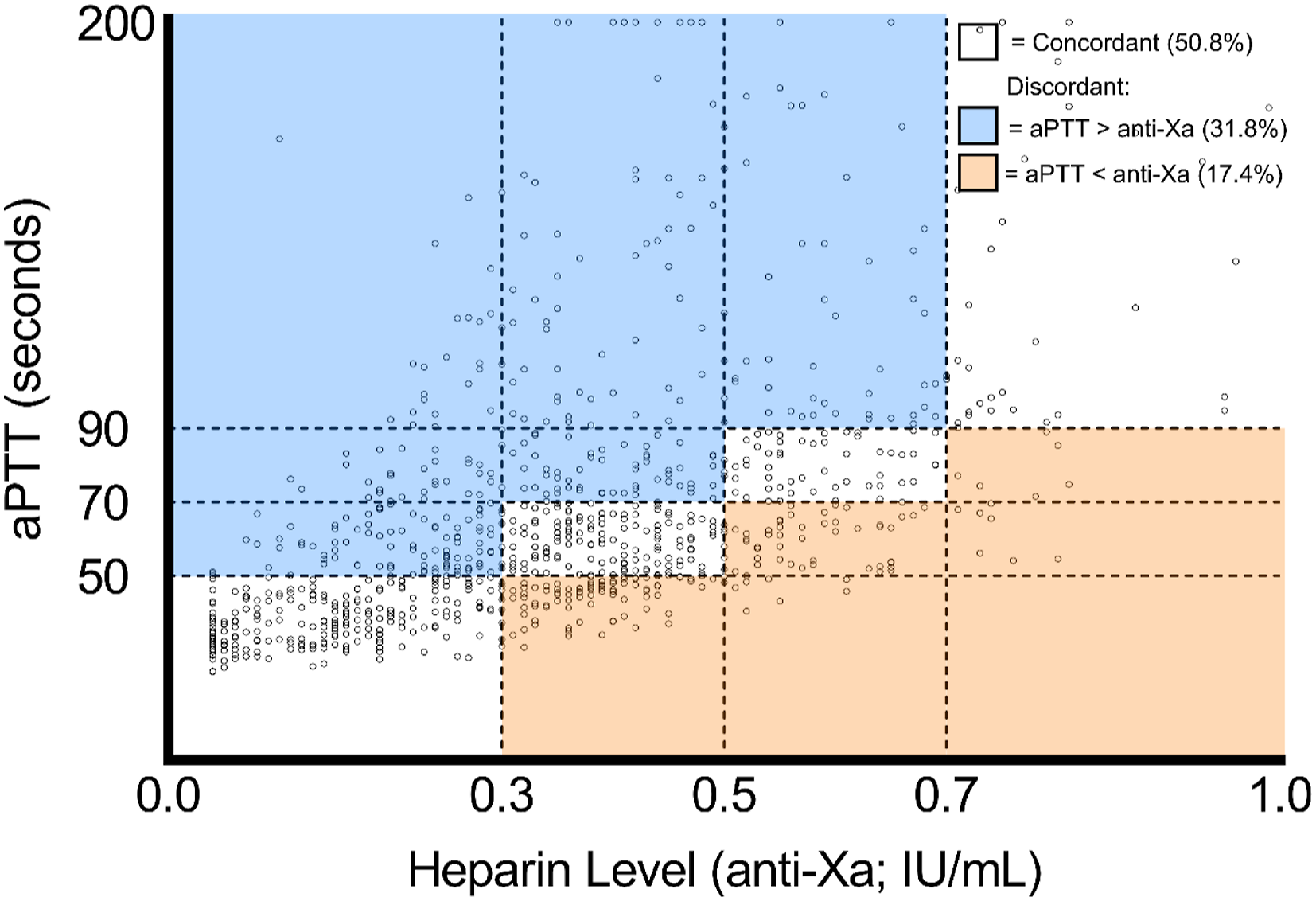
D-risk factors for discordance
The hierarchical multiple logistic regression model controlling for age, sex, body surface area (BSA, m2), Fibrinogen, INR, type of ECLS, and implanted ventricular assist device demonstrated that the odds of discordance increased by a factor of 1.17 for every day since the initiation of ECLS (95% CI 1.09–1.26, p<0.001). The discordance over time was plotted as the percent discordance of paired lab values over discretized periods of time from ECLS initiation in Figure 3. This demonstrated an increase in percent discordance over the first days after ECLS initiation followed by a shift late in prolonged ECLS runs in the proportion of discordance from being mostly when the aPTT indicates a greater degree of anticoagulation to a greater proportion being attributed to the opposite. Percent discordance of paired lab draws within discretized periods of time since ECLS initiation. (Black circles = percent any discordance; blue cross = percent discordance in which aPTT indicates greater degree of anticoagulation compared to that indicated by anti-Xa; orange cross = percent discordance in which anti-Xa indicates greater degree of anticoagulation compared to that indicated by aPTT).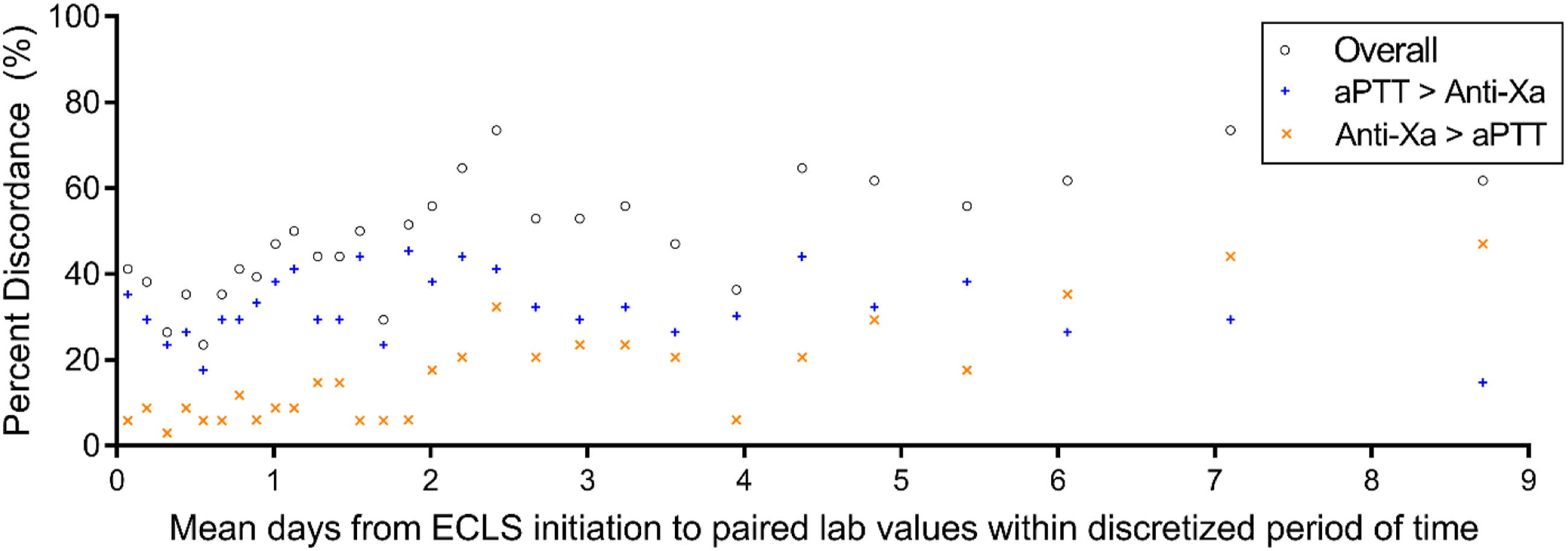
Risk factors for discordance among paired laboratory values.
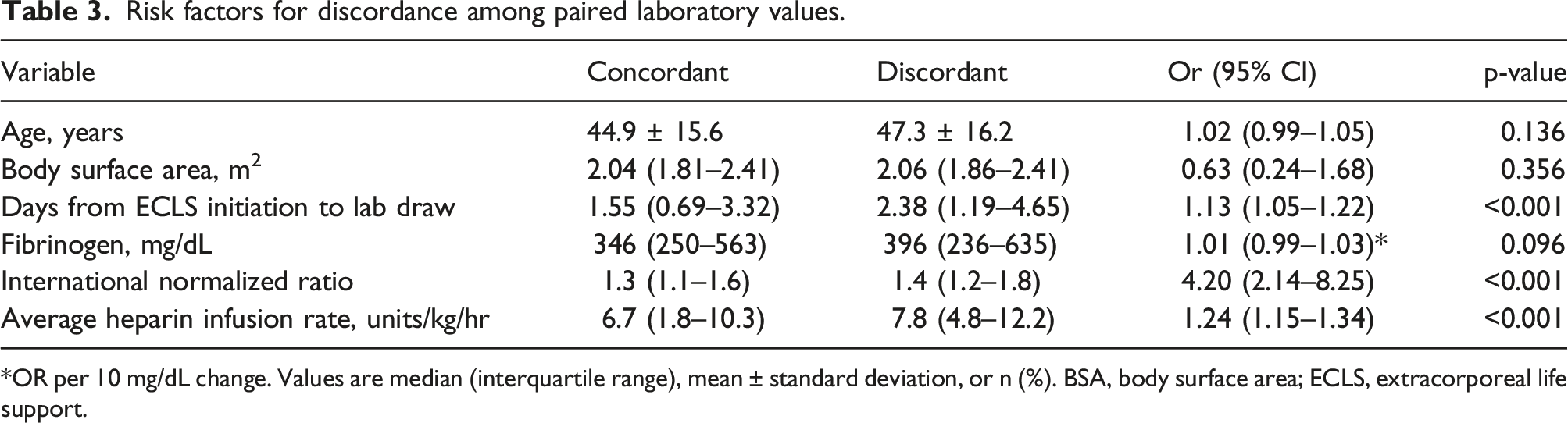
*OR per 10 mg/dL change. Values are median (interquartile range), mean ± standard deviation, or n (%). BSA, body surface area; ECLS, extracorporeal life support.
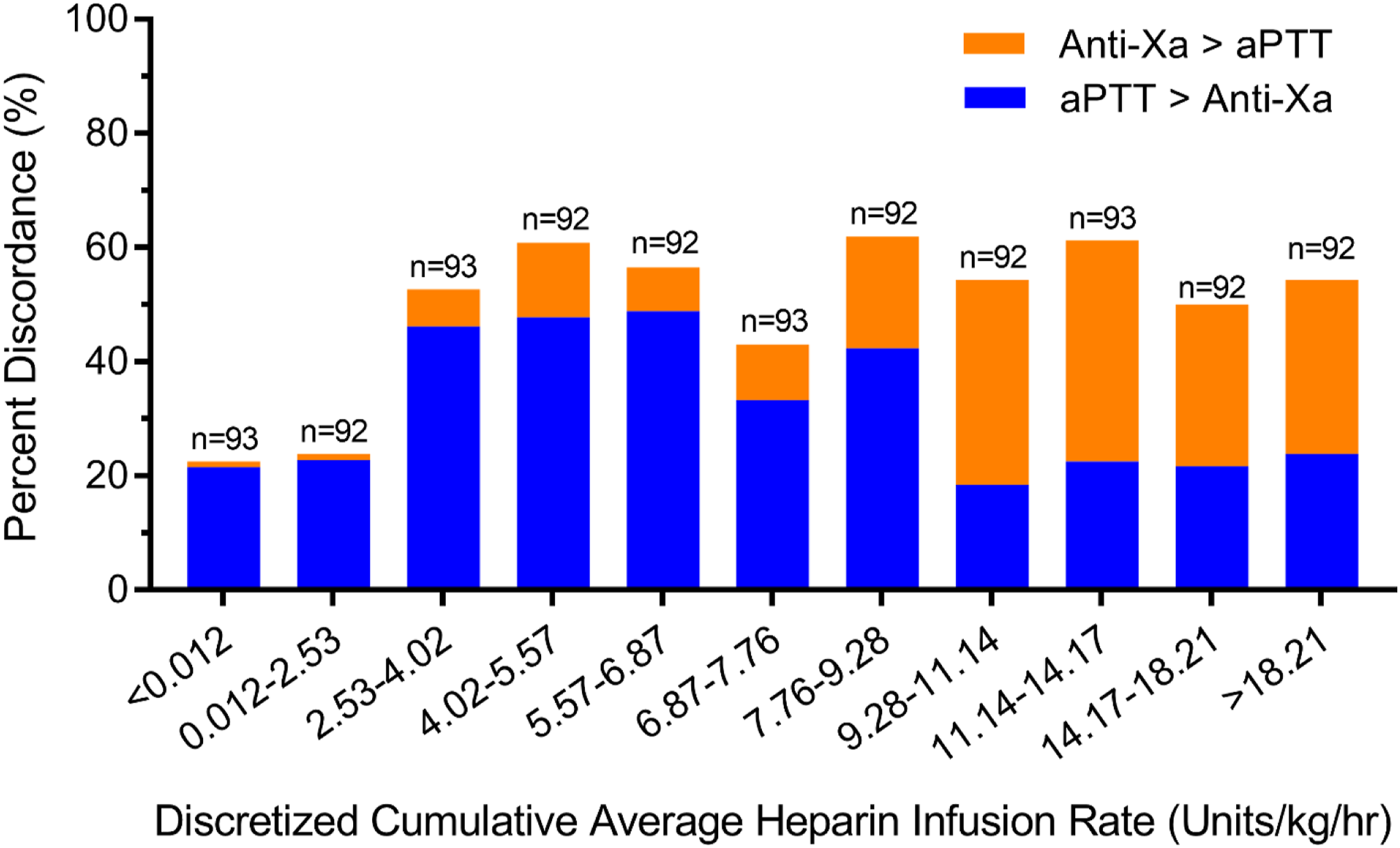
Percent discordance of paired lab draws within discretized ranges of cumulative average heparin infusion rate (U/kg/hr). (Full bar = percent any discordance; blue = proportion of discordance in which aPTT indicates greater degree of anticoagulation compared to that indicated by anti-Xa; orange = proportion of discordance in which anti-Xa indicates greater degree of anticoagulation compared to that indicated by aPTT).
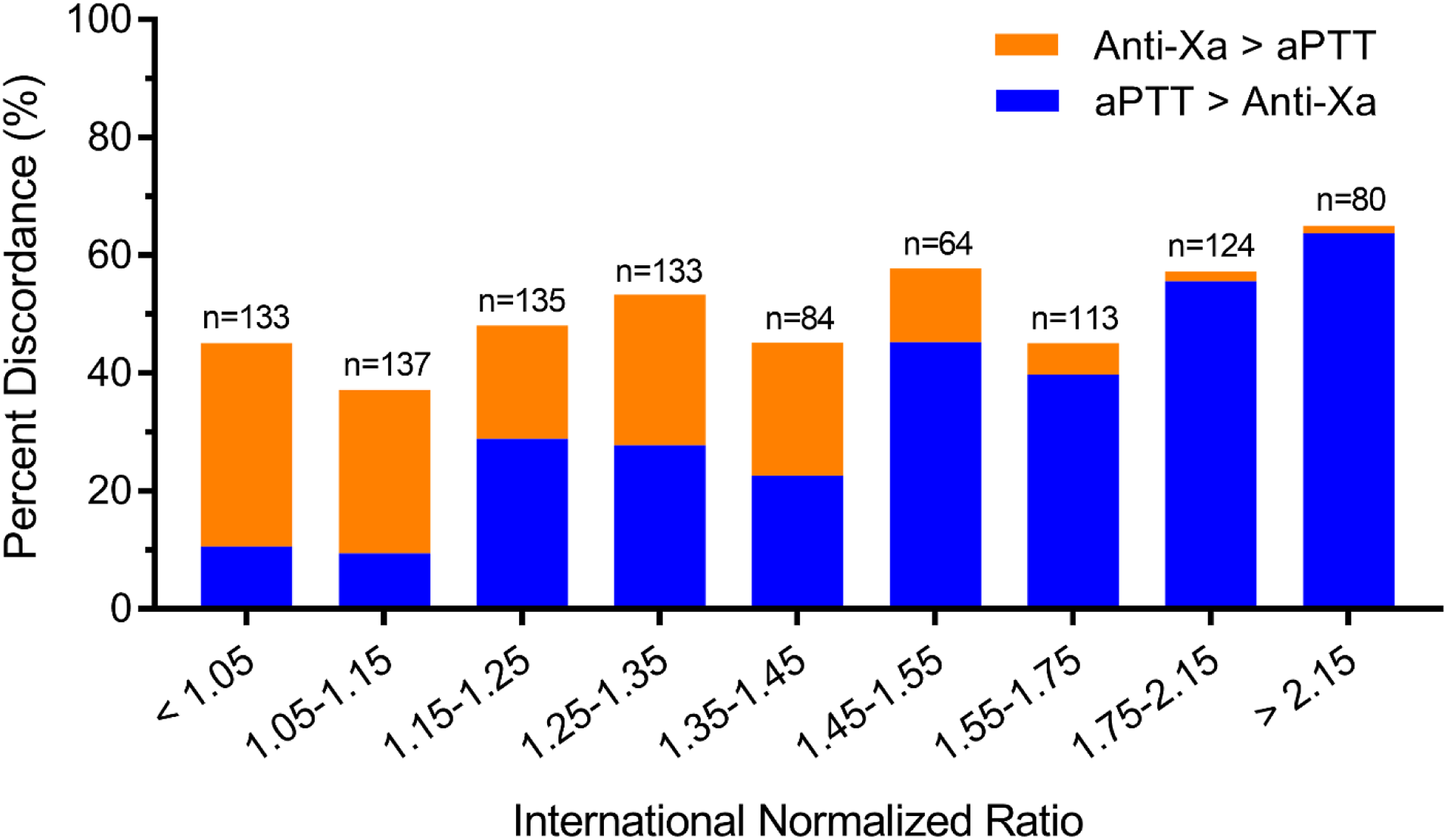
Percent discordance of paired lab draws within discretized INR ranges. (Full bar = percent any discordance; blue = proportion of discordance in which aPTT indicates greater degree of anticoagulation compared to that indicated by anti-Xa; orange = proportion of discordance in which anti-Xa indicates greater degree of anticoagulation compared to that indicated by aPTT).
Discussion
This observational study examined the extent and risk factors for discordance between aPTT and anti-XA in over 1000 samples from 65 ECLS patients anticoagulated with an unfractionated heparin infusion and titrated based on anti-Xa level. Anti-Xa and aPTT were discordant in half of simultaneously drawn measurements with the aPTT indicating a greater degree of anticoagulation compared to the anti-Xa most commonly. Neither aPTT nor anti-Xa correlated well with the average heparin infusion rate and correlation between tests was also low. The odds of discordance increased the longer patients were on ECLS. Furthermore, as the time on ECLS and the average heparin infusion rate increased, the proportion of discordance shifted from mostly the aPTT over-estimating the degree of anticoagulation to mostly the anti-Xa over-estimating the degree of anticoagulation. Finally, a higher INR (INR >1.45) level was associated with the greatest odds of discordance with a shift from a majority of discordance being attributed to the anti-Xa over-estimating the degree of anticoagulation at normal and mildly elevated INRs (INR<1.45) to a majority being attributed to the aPTT over-estimating the degree of anticoagulation at elevated INRs.
Anticoagulation management in ECLS patients requires clinicians to balance the need to prevent circuit thrombosis and clinical thromboembolic events with the risk of causing serious bleeding events, both of which carry an increased risk of morbidity and mortality. 11 There is a paucity of adult ECLS data on appropriate anticoagulation titration in this physiologically complex patient population. These data are consistent with existing evidence that demonstrate discordance between anti-Xa and aPTT in the left ventricular assist device population as well as in the overall population of patients requiring therapeutic anticoagulation.12,13,16–20 The poor correlation between aPTT and anti-Xa have been posited to be related to the administration of blood products, liver disease, coagulation factor deficiencies, and the elevation of factor VIII as an acute phase reactant.13,18 This demonstrates that an elevated INR and the associated vitamin K dependent factor deficiencies increase the likelihood of discordance as the aPTT increases along with the INR while the anti-Xa remains unchanged.13,21 One may conclude that this most common pattern of discordance corresponds to the aPTT over-estimating the degree of anticoagulation and therefore titrating based on aPTT may lead to heparin underdosing and the associated increased risk of thromboembolism. However, the inverse perspective in which titrating heparin based on an anti-Xa which under-estimates the degree of anticoagulation could lead to the overdosing of heparin and an increased risk of bleeding. The data suggest that both scenarios are plausible at different times and in different physiologic states, so titrating heparin based on either test in isolation could lead to bleeding or thromboembolic complications. If the tests are discordant, titration based on anti-Xa may lead to over-anticoagulation soon after heparin initiation or when the INR is elevated when the aPTT will better capture the greater degree of intrinsic anticoagulation due to factors unrelated to heparin administration. Further investigation incorporating the analysis of bleeding and thromboembolic outcomes will be required to more definitively determine in which circumstances one laboratory test should guide therapy over the other, but data already exist which demonstrate that the use of more comprehensive monitoring protocols improve bleeding outcomes. 22 The additional use of thromboelastography and thromboelastometry may be uneconomical, but has potential benefit.23,24
As a retrospective study designed to evaluate discordance between anti-Xa and aPTT when using an anti-Xa based heparin titration protocol, we were unable to establish the advantage of heparin titration based on one test compared to the other. Also, the study is limited to the laboratory values collected as part of our ECLS management protocols, so we were unable to evaluate the influence of labs which were infrequently or never drawn such as antithrombin III levels or specific coagulation factors. Additionally, the data analyzed was from 2015 to 2017. The technologies used during the study period remain the same in the present day, however we do recognize the age of the data as a limitation. Finally, although the heparin infusion rate was included in analysis, we did not incorporate heparin bolus doses, which may have influenced discordance soon after they were given with ECLS initiation. Despite these limitations, our results offer insight into the prevalence and risk factors for discordance between anti-Xa and aPTT.
In summary, nearly half of paired lab values were discordant, typically with aPTT indicating a greater degree of anti-coagulation as compared to anti-Xa. These tests are complementary with the anti-Xa representing a better estimate of the degree of heparinization and the aPTT informing on the coagulation status underlying heparinization. The use of either assay in isolation to guide management may lead to the misestimation of the patient’s true anticoagulation status. The high rate of discordance represents the need to develop management protocols which utilize multiple assays to guide anticoagulation therapy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The National Institutes of Health supported research in this publication under award numbers T32 HL007849 (JJD, JPB, and WZC).
Classifications
Adult; Extracorporeal membrane oxygenation; Blood, coagulation/anticoagulation