
Abstract
We report the case of a 74 years-old male who underwent frozen elephant trunk due to a huge aortic arch aneurysm related to a type 1A endoleak after thoracic endovascular aortic repair where cardioplegic arrest was achieved using the Del Nido cardioplegia.
Introduction
The frozen elephant trunk (FET) procedure is a well standardized technique for the surgical treatment of aortic aneurysms/dissections involving the distal aortic arch and the proximal thoracic descending aorta.1,2 Surgical lengths are usually long, even in not-redo patients, and requires hypothermic circulatory arrest or selective cerebral perfusion (SCP). Cardioplegic arrest is usually achieved using the modified Bretshneider solution as it can protect the heart for very long periods with a single shot infusion 2 but no reports can be found about the use of Del Nido (DN) cardioplegia in these complex aortic procedures.
Hence, we report the case of a patient who underwent FET due to a huge aortic arch aneurysm related to a type 1A endoleak following thoracic endovascular aortic repair (TEVAR) where DN cardioplegia was safely used.
Case report
A 74 year-old man with Stanford type B aortic dissection underwent in 2018 to emergent TEVAR with a free-flow-provided endograft from the left carotid artery (LCA) to the celiac trunk. Left subclavian artery (LSA) was covered but any LCA-to-LSA bypass was performed, and no coils were placed. Follow-up checks confirmed a good operative result until the January 2020 when a type 1A endoleak below LSA and a significant enlargement (55 mm) of the proximal thoracic descending aorta (Figures 1(a) and (b)) were found. Surgery was planned but the patient was lost at follow-up due to Covid-19 pandemic until April 2022 when urgent hospitalization was scheduled as proximal thoracic descending aorta diameter increased from 55 mm to 76 mm (Figure 1(b)). Due to high risk of postoperative paraplegia related to the extensive endovascular covering of the whole supraceliac aorta, intracranial pressure monitoring (IPC) was used. (A) Angio-computed tomography (Angio-CT) scan showing the huge dilatation of the thoracic descending aorta and extended covering by the two previously positioned endografts, (B) the severe enlargement of the thoracic descending aorta (7733 mm) and the site of the proximal endoleak (white arrow). (C) Intraoperative view of the endoleak site (arrow). (D) Final result. (E) Trends of postoperative myocardial necrosis biomarkers, serum lactate during CPB and intraoperative central venous oxygen saturation. (HR: hours; POD: postoperative day; CPB: cardiopulmonary bypass; FF: full flow; NT: normothermic; M: minutes; XClamp: cross clamp; OCP: only cerebral perfusion; SR: systemic reperfusion; XClampRem: cross clamp removal; ICU: intensive care unit).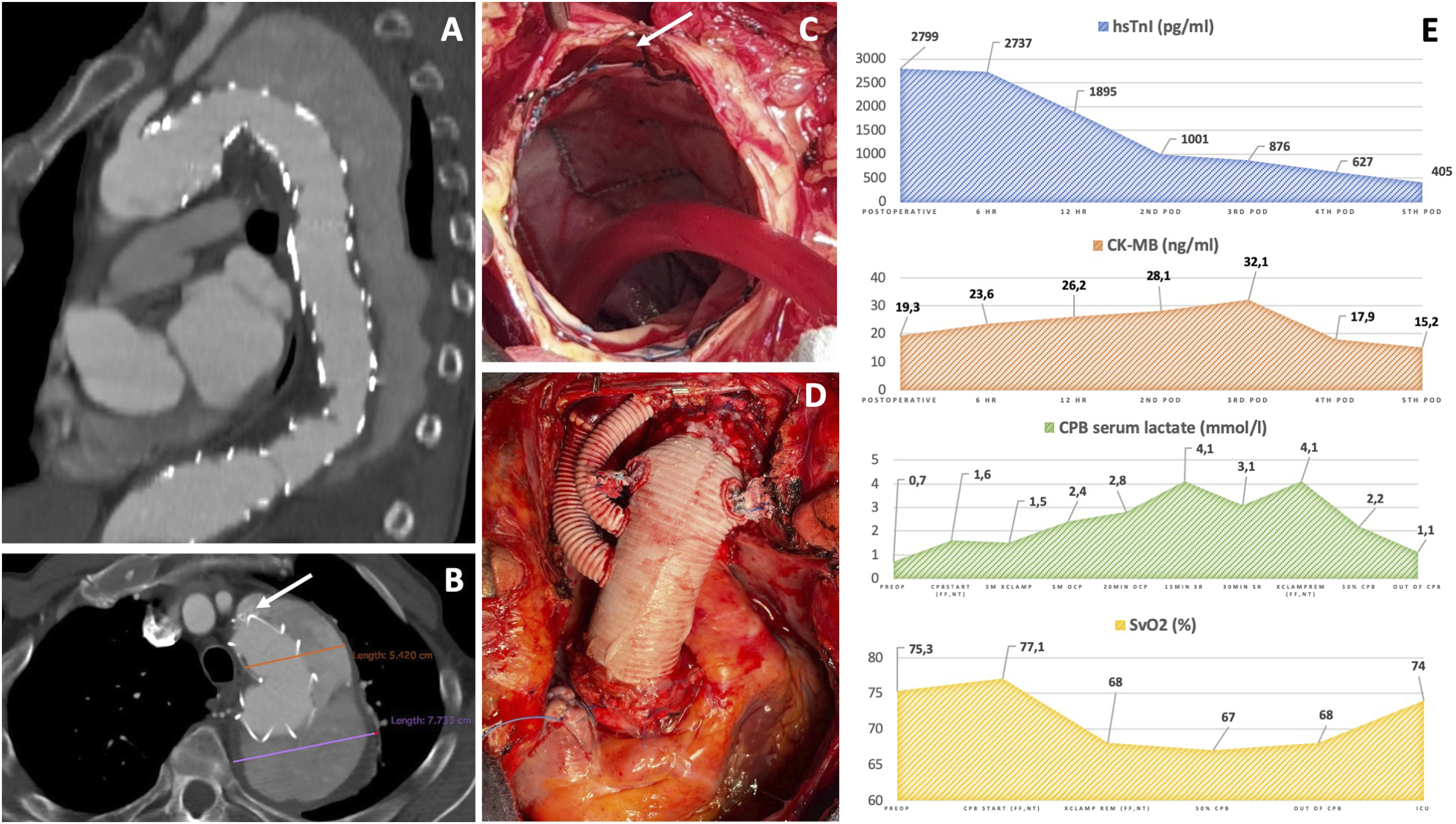
Cardiopulmonary bypass (CPB) was established through ascending aorta/right atrium cannulation and the patient was cooled up to 26°C of bladder temperature. The ascending aorta was clamped and a single shot of antegrade DN cardioplegia was administered according to the original protocol. 3 DN cardioplegia was chosen in order to reduce the amount of administered fluids and to protect the heart and, especially, the spinal cord from postoperative edema. After circulatory arrest and aortic arch opening, antegrade SCP (10 mL/kg/min) was performed according to the Kazui technique and through near infrared spectroscopy monitoring. At the opening of the aorta, the endoleak site was found below the LSA ostium (Figure 1(b)), the free-flow stents were removed and the endograft was secured to the native aortic wall with four cardinal 4/0 polypropylene stiches with Teflon support. Frozen elephant trunk was then performed using a 30 × 36 × 130 mm Evita® Open Neo (Jotec, Hechingen, Germany) graft in aortic Zone 2, and systemic perfusion was restarted through the prosthesis side branch after 39 minutes of systemic circulatory arrest. Epiaortic vessels were reimplanted during beating-heart rewarming (Figure 1(d)), excluding LSA to avoid the risk of thrombus embolization. Any electrical activity occurred during cross-clamping and no defibrillations or inotropic support were necessary to wean CPB (CPB length: 209 minutes; Cross-Clamp length: 133 minutes; SCP length: 163 minutes).
Perioperative course was uneventful. IPC monitoring was removed in the 4th postoperative day and a total drainage of 65 mL of cerebrospinal fluid was necessary to stabilize the IPC around 10 mmHg. The patient was discharged on the 9th postoperative day without any permanent neurologic dysfunctions.
Discussion
The DN cardioplegia is a crystalloid solution mixed with patient’s blood, firstly used in pediatric cardiac surgery. A single shot of 1000 mL is enough when the patient’s weight is greater than 50 kg to ensure up to 90 minutes of myocardial protection therefore it allows to perform almost all of the most common adult cardiac surgeries. Few data exist about the use of DN cardioplegia in during procedures with a prolonged cross-clamping, but D’Angelo et al. 4 suggest that, after re-administration, it can be safely used even during those surgeries with more than 3 hours of myocardial ischemia.
To date, many authors report its use during coronary artery or valves surgery4–6 but, no reports are present about complex aortic surgeries such as FET. During these procedures, aortic cross-clamping lengths are usually long, and the use of systemic hypothermic arrest imposes to not waste time, even to re-dose cardioplegia. Bretshneider cardioplegia is the ideal solution as it protects the heart up to 180 minutes with a single infusion even if, unfortunately, it has to be administered in very great amounts (2000–2500 mL). During hypothermic procedures, in chronic kidney diseases or very decompensated patients, fluid overload and severe hemodilution can be detrimental therefore could be very useful to limit as much as possible the fluid intake.
In this regard, a single shot of DN cardioplegia can protect the heart up to 120 minutes during hypothermic procedures 5 using a very lower amount of administered fluids and can avoid the use of hemofiltration during CPB to remove the cardioplegia. The use of moderate-to-severe hypothermia that requires FET procedure, indeed, can highly benefit from lowering of hemodilution, fluid overload and lactate release related to the use of Del Nido Cardioplegia; on the other hand, as reported in literature, 5 the use of hypothermia can prolong the safe period of this cardioplegia from 90 minutes up to 120 minutes, allowing to perform even concomitant aortic root procedures. DN solution, in addition, seems to be associated with a significant lower rate of ventricular fibrillations at reperfusion and a lower troponin release.5,6 This report confirms these data and suggests that DN solution can be safely used even in very complex aortic surgery: myocardial enzymes release until the 5th postoperative day, serum lactate levels during CPB and central venous O2 saturation during the operation (Figure 1E) showed a very good trend as well as biventricular function at postoperative echocardiogram that was similar to preoperative one. Further analysis on a larger population are necessary, but preliminary data are quite encouraging.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
IRB approval was not necessary. Informed consent was obtained.