
Abstract
Introduction
Conservative management is usually preferred for iatrogenic tracheal injuries. Venovenous extracorporeal membrane oxygenation (V-V ECMO) is mostly used in acute refractory hypoxemia, airway lesions are an alternative indication.
Case Report
A 51-year-old female was transferred with a large tracheal tear after plastic tracheotomy. Due to a critical ventilation situation with hypercapnia, conservative management was set and V-V ECMO was installed. With optimized tube positioning, minimal ventilation and gas transfer via V-V ECMO, a complete healing of the injury could be achieved.
Discussion
Fast diagnosis of tracheal injuries is essential; transfer to a specialized centre should be considered. In our case, organ support via ECMO was necessary due to a difficult ventilation situation with persisting hypercapnia. Thus, reduction in ventilation pressures with reduction of possible leakage and healing of the tracheal tear could be achieved.
Conclusion
Management of tracheal tears is complex; in severe cases special therapy concepts such as the use of V-V ECMO may become necessary.
Introduction
Injuries of the trachea and the bronchial system occur seldom. 1 Incidence in trauma patients with chest and neck injuries is 0.5 – 2%. 2 Various iatrogenic injury mechanisms are conceivable, such as tracheostomy, endotracheal intubation, and rigid bronchoscopy. 3 The incidence is between 0.005% for routine single-lumen endotracheal intubation or tracheostomy and 1% during emergency airway procedures.1,4 Management of such lesions, which vary greatly in location, tissue involvement, and therefore severity, 3 is complex and should be coordinated on an interdisciplinary basis. Consideration must be given to securing the airway, but also to optimizing the chances of recovery in terms of tube position, muscle tone, and avoidance of further trauma. 3 Generally, conservative management is preferred especially for iatrogenic lesions. 2
Usually, venovenous extracorporeal membrane oxygenation (V-V ECMO) is used in hypoxemic and hypercapnic respiratory failure, as well as ventilatory support as a bridge to lung transplantation. 5 Less frequently, it can be used for alternative indications including endangered airways. 6 We present the case of a patient with severe tracheal tear and difficult ventilation situation as alternative ECMO indication.
Case report
In July 2022, a 51-year-old female (1.49 m, 84 kg) was transferred with a large tracheal tear one day after plastic tracheotomy. The patient had been hospitalised for two weeks due to an acute exacerbation of COPD and pneumonia, with intubation 9 days before tracheostomy. Several comorbidities including a severe obstructive sleep apnoea with non-invasive positive pressure ventilation, coronary heart disease, obesity, and insulin-dependent diabetes mellitus were present.
On admission, the patient was sedated and hemodynamically stable. She was ventilated via right-sided single lung ventilation via a tracheal cannula 9.0 mm ID (Tracheofix®). The airway was compromised as frequent changes in tidal volume and insufficient ventilation occurred. Our first bedside bronchoscopy showed a severe laceration in the membranous portion of the trachea with a length of 4 cm, localised 5 mm above the main carina, and reaching to the distal end of the tracheostoma with a massive secretion (Figure 1(a)+(c)). Because of a tension pneumothorax, possibly due to dislocated tracheal cannula or high ventilation pressures (Pinsp 38-43 cmH2O), thoracic drains on both sides were placed. We inserted an endotracheal tube (5.5 mm ID) via the tracheal cannula to the left bronchial system. Due to the secretion from the area of the tracheal lesion, a cuffed orotracheal tube (6.5 mm ID) was placed in the right main bronchus to protect against aspiration (Figure 1(b)). Empiric antibiotic therapy with meropenem, vancomycin and caspofungin was started. In the absence of surgical and endoscopic options through the critical ventilation period a conservative approach was decided by our interdisciplinary team. (1a): CT chest with signs of a massive injury of the trachea without mediastinitis. (1b): X-ray with endotracheal tube via the tracheal cannula placed in the left bronchial system and an orotracheal tube in the right main bronchus. (1c): First bronchoscopy with a severe lesion in the membranous portion of the trachea. (1d): Follow-up bronchoscopy after 6 weeks.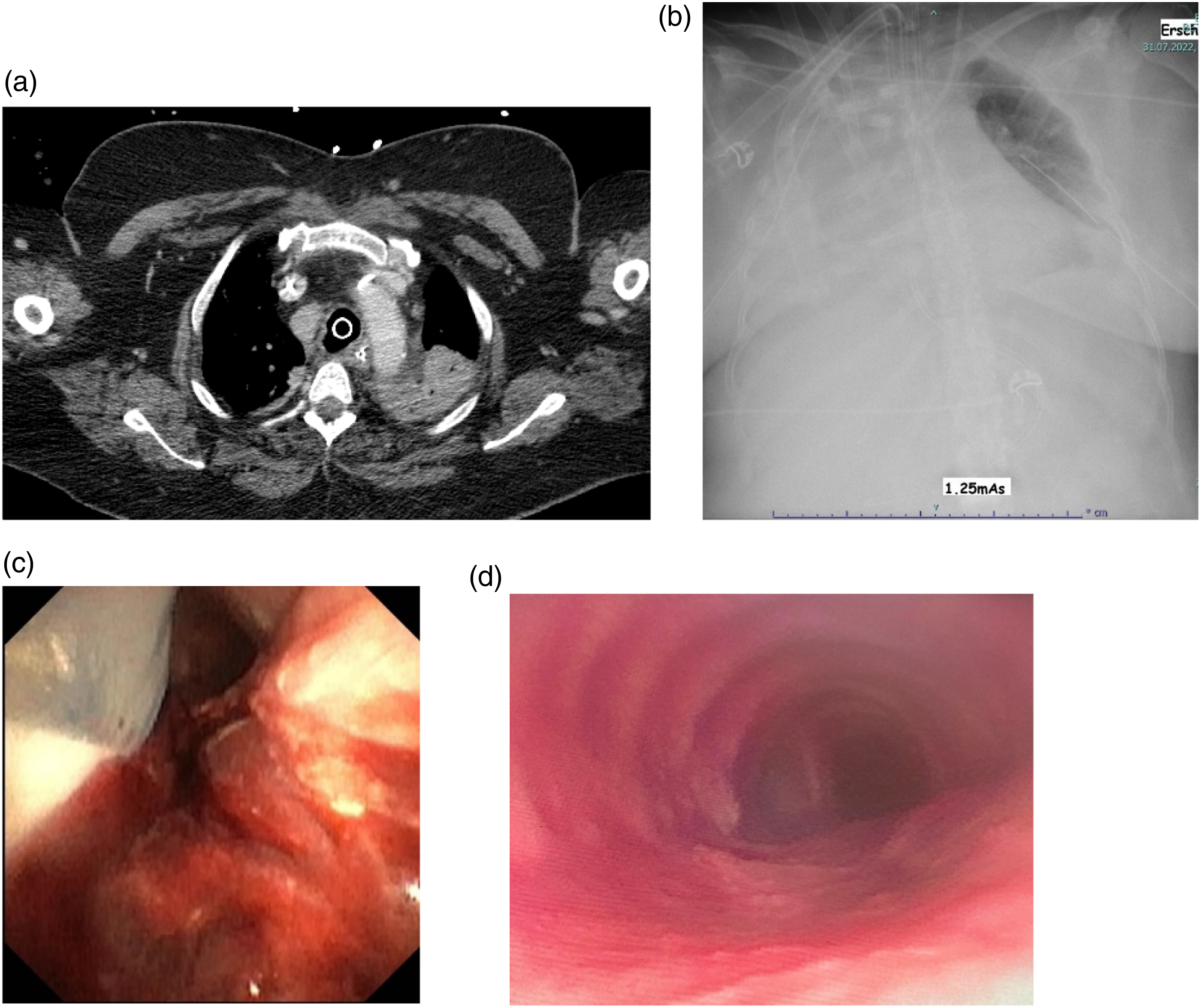
Impaired ventilation, severe hypercapnia, and high ventilation pressures remained (Pinsp 41 cmH2O, PEEP 14 cmH2O, RR 34/min, paCO2 72 mmHg, pH 7.29). Therefore, we installed V-V ECMO (29Fr right femoral and 21Fr right jugular cannula; blood flow 3,2 L/min, sweep gas flow 4 L/min) to reduce ventilation support, enable sufficient CO2 removal (Pinsp 22 cmH20, PEEP 12 cmH20, RR 10/min, paCO2 42 mmHg, pH 7.40), and gain time for healing of the tracheal tear.
Bronchoscopic checks showed increasing healing of the lesion with fibrin layers and incipient granulation tissue. After 13 days, the secretion had ceased, and the orotracheal tube could be removed. Regular changes of the tracheal cannula were performed. Due to the healing of the tracheal tear and a stable ventilation, we started ECMO weaning. After 33 days, decannulation was performed. Subsequently, spontaneous breathing phases were continuously expanded. In parallel, non-invasive ventilation was established and two weeks after ECMO decannulation the tracheal cannula was removed. A follow-up bronchoscopy six weeks after transfer to our hospital, showed a complete closing of the severe tracheal tear (Figure 1(d)). After 7 weeks, the patient was finally discharged for rehabilitation.
Discussion
Tracheal injuries are serious conditions that are associated with high mortality. 7 Rapid detection is essential. 3 Mostly the posterior membranous portion is affected. 8 In our case, the injury occurred iatrogenically after tracheostomy and patient characteristics are typical.
For most lesions, a conservative approach, or minimally invasive procedures such as endobronchial stents are performed, especially in iatrogenic injuries 3 . 7 A German case series reports five cases of conservative treatment in iatrogenic tracheal injuries. 9 In each case the cuff was inflated distal to the lesion guided by bronchoscopy and a complete healing could be achieved. In contrast, a recent review recommends a primarily surgical approach for defects greater than two centimetres. 1 In our case, we decided for a conservative approach due to unstable ventilation with severe hypercapnia in COPD and obesity. In line with the previously presented case series, there was no mediastinitis, which is one of the main concerns when surgical procedures are not performed. 9
The key benefit of organ support via ECMO is a reduction in ventilator support. Overall, there are only few case reports on the use of ECMO in iatrogenic tracheal injuries. Son et al. reported the case of a 68-years-old female with a 5cm-tracheal injury and successful conservative treatment including ECMO and maintaining self-respiration. 10 In addition, an indication may also lie in the surgical treatment of tracheal injuries. 11
To summarize, ECMO may be necessary in difficult ventilation situations due to tracheal injuries. The advantages are a significant reduction in ventilation pressures with reduction of possible leakage and optimal oxygenation. Thus, in our case, complete healing of a severe iatrogenic tracheal tear was achieved.
Conclusion
Tracheal lesions are life-threatening conditions that occur rarely. Based on the available literature, it is often difficult to derive a clear approach due to the varying injury severity and comorbidities. Therefore, patients should be referred to specialized centres and all procedures including V-V ECMO should be determined on an interdisciplinary basis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
All authors revised the article and approved the current version to be published
Informed Consent
Written informed consent was obtained from the patient for publication of data and images. According to the ethics committee of the University of Heidelberg ethics vote was not necessary.