
Abstract
Background
Postcardiotomy extracorporeal membrane oxygenation (ECMO) in pediatric patients can be affected by the place of initiation, either in the operating room (OR) or the pediatric cardiac intensive care unit (PCICU). This study aimed to characterize and compare patients who had postcardiotomy ECMO initiation in the OR or PCICU and evaluate risk factors for hospital mortality.
Methods
This retrospective study included 103 patients who required postcardiotomy ECMO support after the repair of congenital cardiac lesions from 2010 to 2022. Patients were grouped according to the place of ECMO insertion into two groups. Group 1 (n = 69) had ECMO insertion in the OR, and Group 2 (n = 34) had ECMO insertion in the PCICU.
Results
Cardiac arrest occurred significantly more often in patients with ECMO insertion in the PCICU (21 (61.76%) vs. 13 (18.84%); p < 0.001). Pre-ECMO lactate levels, pH, VIS, base deficit, and PaO2 did not differ between the groups. Re-exploration for bleeding was significantly higher in Group 1 (32 (46.38%) vs. 8 (23.53%); p = 0.03). Cannula repositioning (4 (11.76%) v. 2 (2.90%); p = 0.09) and mechanical ventilation time were nonsignificantly higher in Group 2 (19.5 (10–31) vs. 11 (5–25) days; p = 0.07). No difference in mortality was found between groups (42 (60.87%) vs. 23 (67.65%), p = 0.50). By multivariable analysis, elevated lactate on ECMO and low pH before ECMO were associated with mortality.
Conclusions
ECMO insertion in the OR has a comparable mortality rate to PCICU insertion. Pre-ECMO low pH and high lactate during ECMO could predict mortality.
Introduction
Extracorporeal membrane oxygenation (ECMO) is widely used to support patients with congenital heart disease (CHD) and has become a solution for cardiorespiratory insufficiency when conventional therapies fail. 1 In the postoperative period following the repair of CHD, ECMO may be required for many reasons, including failure to separate the patients from cardiopulmonary bypass (CPB) or progressive hemodynamic deterioration with cardiogenic shock or cardiac arrest. 2 Despite recent advances in ECMO technology, the mortality rate in pediatric patients is still high. 3 The Extracorporeal Life Support Organization (ELSO) registry reported survival to hospital discharge in 42% of neonatal cardiac ECMO, 41% in neonatal ECMO for cardiopulmonary resuscitation (E-CPR), 51% in pediatric cardiac ECMO, and 41% in pediatric E-CPR. 4
ECMO remains the most commonly used mechanical cardiopulmonary support in infants and young children in the immediate postoperative period. Factors affecting hospital mortality and morbidity in patients with CHD supported with ECMO vary widely in the literature. This variation could be attributed to the heterogeneity of the population, different ECMO indications and techniques, and the timing of ECMO initiation. 5 It is controversial whether ECMO initiation in the operating room (OR) or pediatric cardiac intensive care unit (PCICU) will affect hospital mortality. ECMO initiation in the PCICU could occur in the context of cardiac arrest or cardiogenic shock and, consequently, a higher mortality risk. On the other hand, ECMO insertion in the operating room may indicate severe cardiac dysfunction. 6 Elmahrouk and associates found that ECMO connection in the OR was associated with a nonsignificantly higher survival (49%) than ICU ECMO (40%). 7 Other studies reported that early ECMO support for myocardial failure before the commencement of prolonged cardiogenic shock was crucial for better outcomes in patients with severe cardiac failure after congenital cardiac surgery.8,9 Therefore, this study aimed to characterize patients with postcardiotomy ECMO initiation in the OR or PCICU, compare the outcomes between these two groups, and evaluate risk factors for hospital mortality.
Patients and methods
Design and Setting
This research is a retrospective study conducted in the PCICU of Prince Sultan Cardiac Centre-Riyadh. All congenital heart disease patients admitted to the PCICU who required ECMO support between January 2010 and January 2022 were enrolled in the study. The data were collected from electronic and paper medical records. The case notes of 122 patients were reviewed. Out of these 122 patients, we excluded 19 patients: 7 had incomplete medical records, and 12 were excluded because they had no prior cardiac surgery. One hundred and three patients were included in the study. All patients included required ECMO support postcardiac surgery for congenital lesions due to low cardiac output syndrome. The place of ECMO insertion was either in the PCICU or OR. Patients were grouped according to the place of ECMO insertion into two groups. Group 1 (n = 69) had ECMO insertion in the OR, and Group 2 (n = 34) had ECMO insertion in the PCICU.
The study was approved by the Scientific Research Center of the Prince Sultan Military Medical City (IRB approval number: 1665).
Study variables and outcomes
The study variables included patients’ demographics, associated syndromes, the Risk Adjustment for Congenital Heart Surgery (RACHS) category, cardiac arrest, highest lactate, lowest PH, base deficit, highest creatinine, lowest PaO2, and highest vasoactive inotropic score (VIS). Operative variables included bypass and ischemic times and the number of bypass runs. The biochemical parameters were reported before and during ECMO support. The primary outcome was hospital mortality. Secondary outcomes were hospital complications, ECMO-related complications, duration of PCICU, and hospital stay.
ECMO technique
The indication for ECMO in these patients was failure to wean from cardiopulmonary bypass due to low cardiac output syndrome. All patients received central veno-arterial ECMO support. According to protocol procedures, the type, size, and site of the cannula depend on weight, age, and indication of ECMO. Pump flow was started initially at 100 mL/kg/min and adjusted to maintain adequate perfusion; a higher flow of up to 200 mL/kg/min may be needed for patients with single ventricle physiology. Inotropes were kept at a minimum and adjusted as needed. Afterload-reducing agents are often utilized to improve cardiac performance in patients with high blood pressure. Before cannulation, a dose of 50–100 units/kg heparin was given. Activated clotting time (ACT) was performed within 5 min of initiation of ECMO and every 60 min until target ACT was achieved and bleeding was controlled (chest tube drainage less than 5 mL/kg/h). Anticoagulation was achieved by continuous heparin infusion, maintaining an ACT between 180 and 200 s with heparin infusion according to the protocol. ACT levels were monitored two hourly for the first 12 h; then, the follow-up was with partial thromboplastin time (PTT) according to the protocol. Heparin reversal was performed to achieve the target ACT on ECMO for patients who had ECMO insertion because of failure of separation from cardiopulmonary bypass. Hemoglobin was kept at 12 g/dl, and the platelet count was over 100,000/mm3. The left heart was decompressed via a left atrial cannula inserted through one of the pulmonary veins in all patients.
Ventilation was adjusted at a low setting to maintain oxygenation of blood generated by native cardiac output and to prevent lung atelectasis. Head ultrasound was performed on alternate days for patients with open fontanels to exclude intracranial hemorrhage. The target temperature was between 35.5 and 37°C. Diuretics were given to promote diuresis when urine output was below 2–3 ml/kg/hr. In persistently oliguric or anuric patients, slow continuous ultrafiltration or peritoneal dialysis was used to remove extra volume. In patients with renal failure, dialysis was preferred. Nutrition was commenced 24–48 h after the institution of ECMO. The enteral route was preferred unless the food was poorly absorbed. In this case, total parenteral nutrition was started alternatively. Broad-spectrum prophylactic antibiotics, usually ceftazidime and vancomycin, were prescribed, and the dose was adjusted as necessary.
Statistical analysis
Qualitative data are presented as numbers and percentages and were compared with the chi-squared or Fisher exact test when appropriate. Quantitative data are presented as the mean and standard deviation or median (25th −75th percentiles), according to the normality distribution tested with the Shapiro‒Wilk test. Quantitative data were compared with the t test or Wilcoxon test when appropriate. Repeated measures were compared between the two groups with random effect regression. Survival was plotted using a Kaplan‒Meier curve and compared with the log-rank test. Stepwise logistic regression with forward selection was used to identify the risk factors for hospital mortality. Significant variables in the univariable analysis were introduced into the multivariable models, and a p value of 0.05 or less was required to retain the variables in the final model. Stata 17 was used for all analyses (Stata Corp- College Station, TX, USA).
Results
Baseline and operative data
The study included 17 (24.64%) neonates and 33 (47.83%) infants in Group 1 vs 8 (23.53%) and 15 (44.12%) in Group 2, respectively. There were no differences in age groups, sex, gestational age, weight, height, or syndromes between groups. RACHS score categories were significantly higher in Group 1. ECMO insertion in the operating room was due to failure of separation from cardiopulmonary bypass in 56 patients (81.16%) and sudden cardiac arrest after separation from cardiopulmonary bypass and heparin reversal in 13 patients (18.84%). ECMO insertion in the PCICU was indicated for low cardiac output in 13 patients (38.24%) and for cardiac arrest in 21 patients (61.76%). The median time to ECMO insertion in the PCICU was 24 h (25th- 75th percentiles: 6–123 h).
Comparison of preoperative and operative data between patients who received ECMO in the operating room (Group 1) and those who received ECMO in the pediatric cardiac intensive care unit (Group 2).
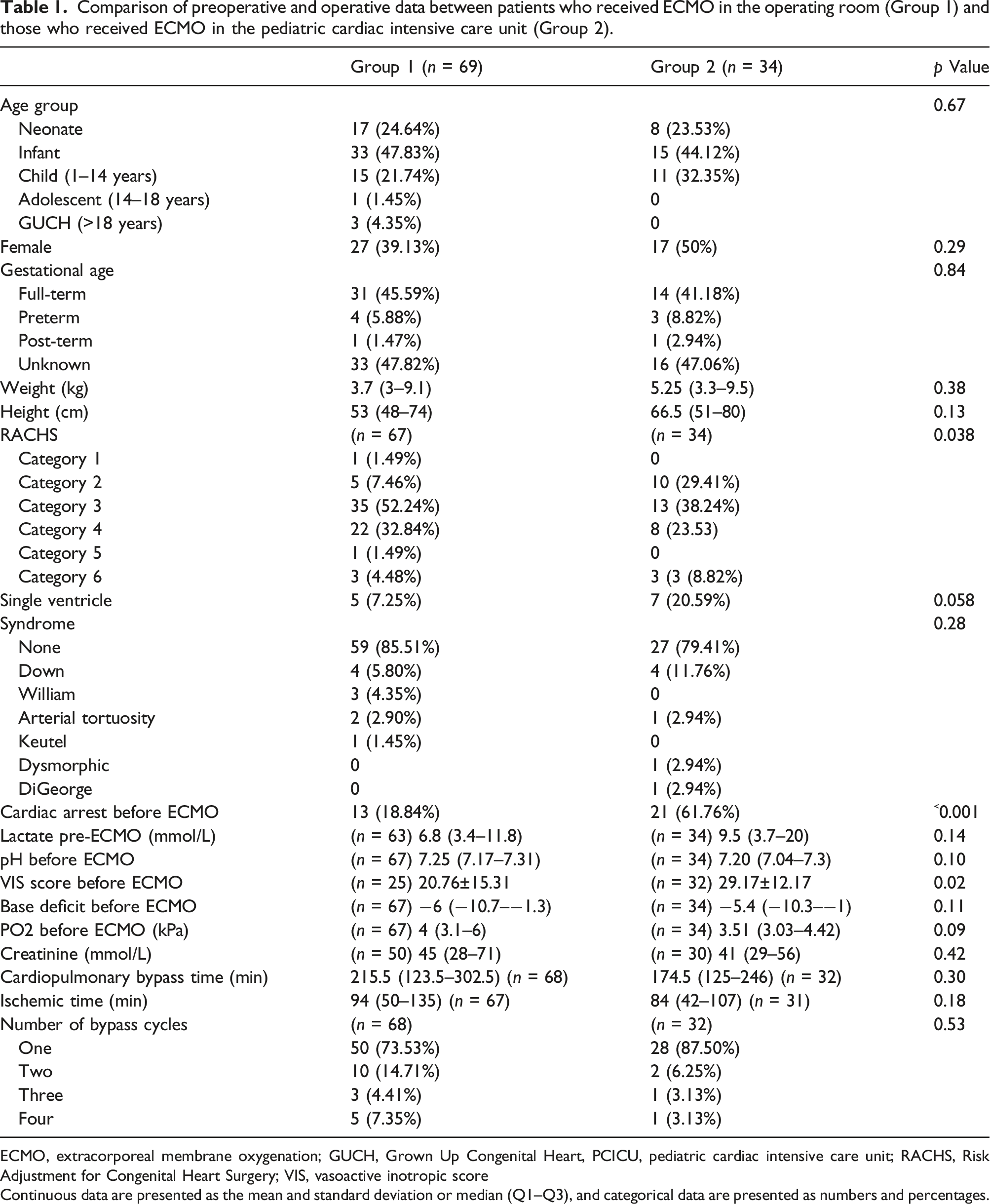
ECMO, extracorporeal membrane oxygenation; GUCH, Grown Up Congenital Heart, PCICU, pediatric cardiac intensive care unit; RACHS, Risk Adjustment for Congenital Heart Surgery; VIS, vasoactive inotropic score
Continuous data are presented as the mean and standard deviation or median (Q1–Q3), and categorical data are presented as numbers and percentages.
Outcomes
Comparison of extracorporeal membrane oxygenation (ECMO) and postoperative data between patients who had ECMO in the operating room (Group 1) vs. pediatric cardiac intensive care unit (Group 2).
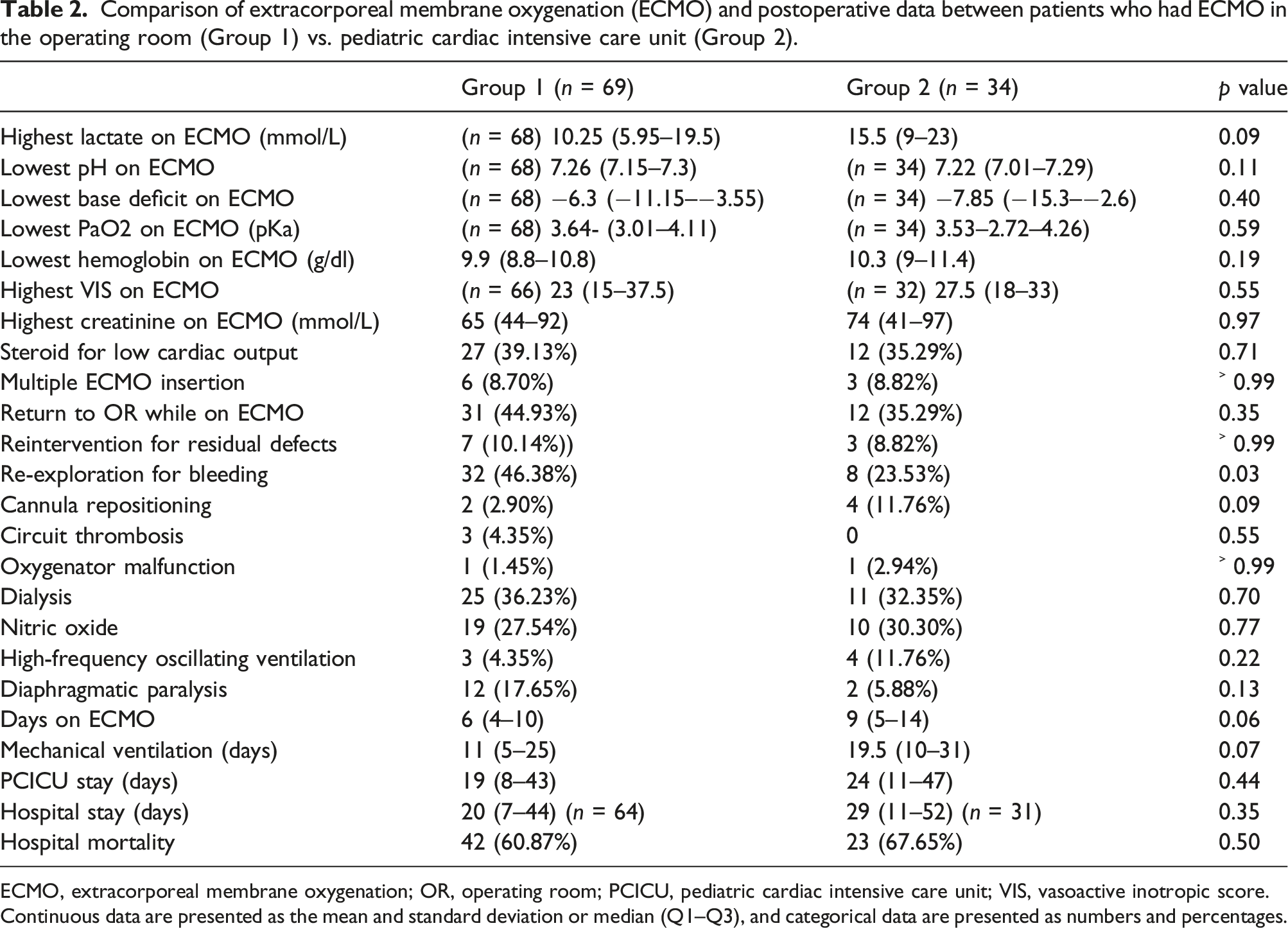
ECMO, extracorporeal membrane oxygenation; OR, operating room; PCICU, pediatric cardiac intensive care unit; VIS, vasoactive inotropic score.
Continuous data are presented as the mean and standard deviation or median (Q1–Q3), and categorical data are presented as numbers and percentages.
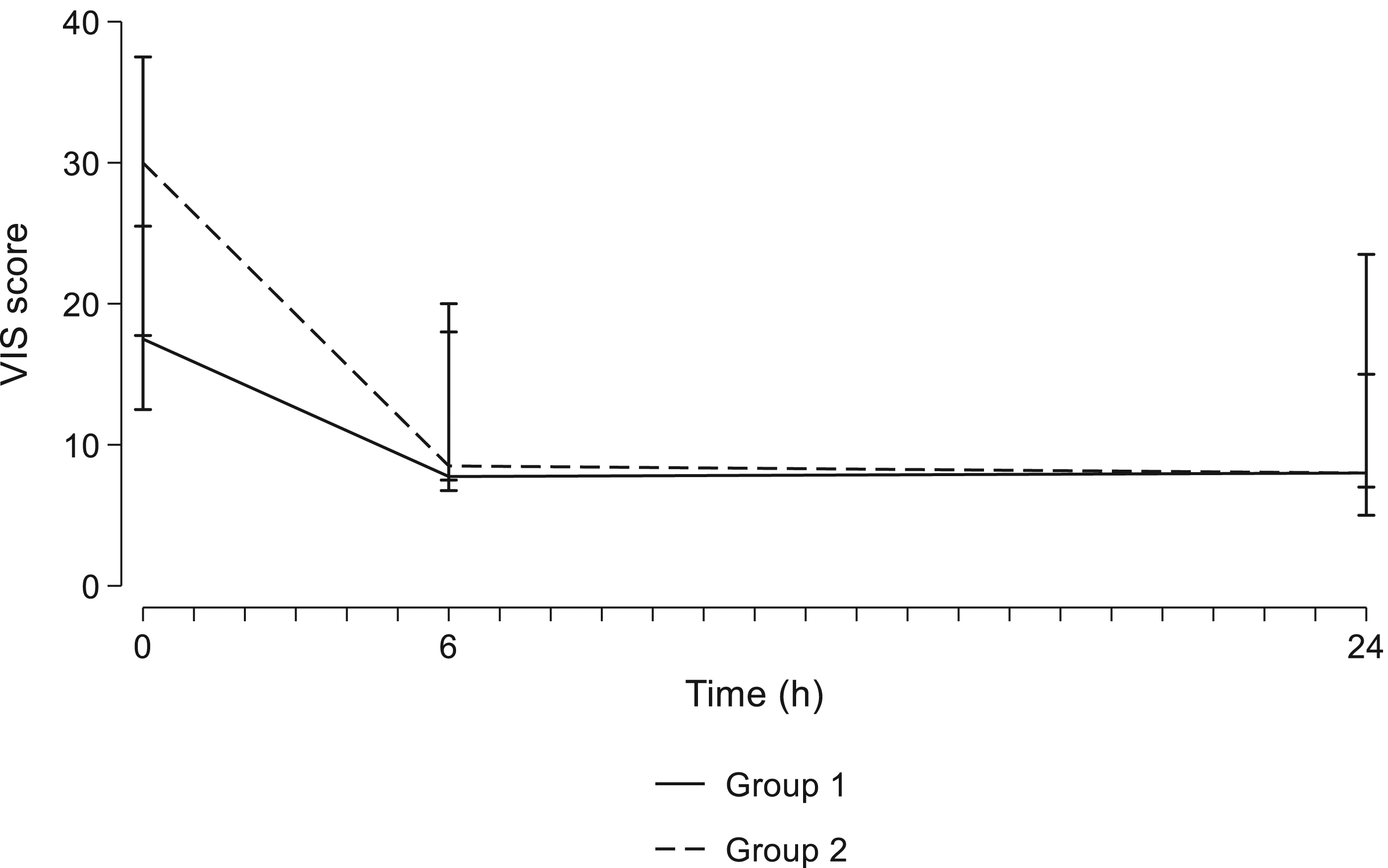
There was no difference in the change in lactate levels between the groups (β: 0.88 (95% CI: −1.22–2.98); p = 0.413). (Figure 1) There was no significant change in VIS score between groups (β: 4.78 (95% CI: −0.21–9.76); p = 0.06) (Figure 2). Changes in lactate levels for patients who had extracorporeal membrane oxygenation in the operating room (Group 1) or pediatric cardiac intensive care unit (Group 2). (Values are presented as the median, and the bar is the interquartile range.) Changes in the vasoactive inotropic score (VIS) for patients who had extracorporeal membrane oxygenation in the operating room (Group 1) or intensive care unit (Group 2). (Values are presented as the median, and the bar is the interquartile range.)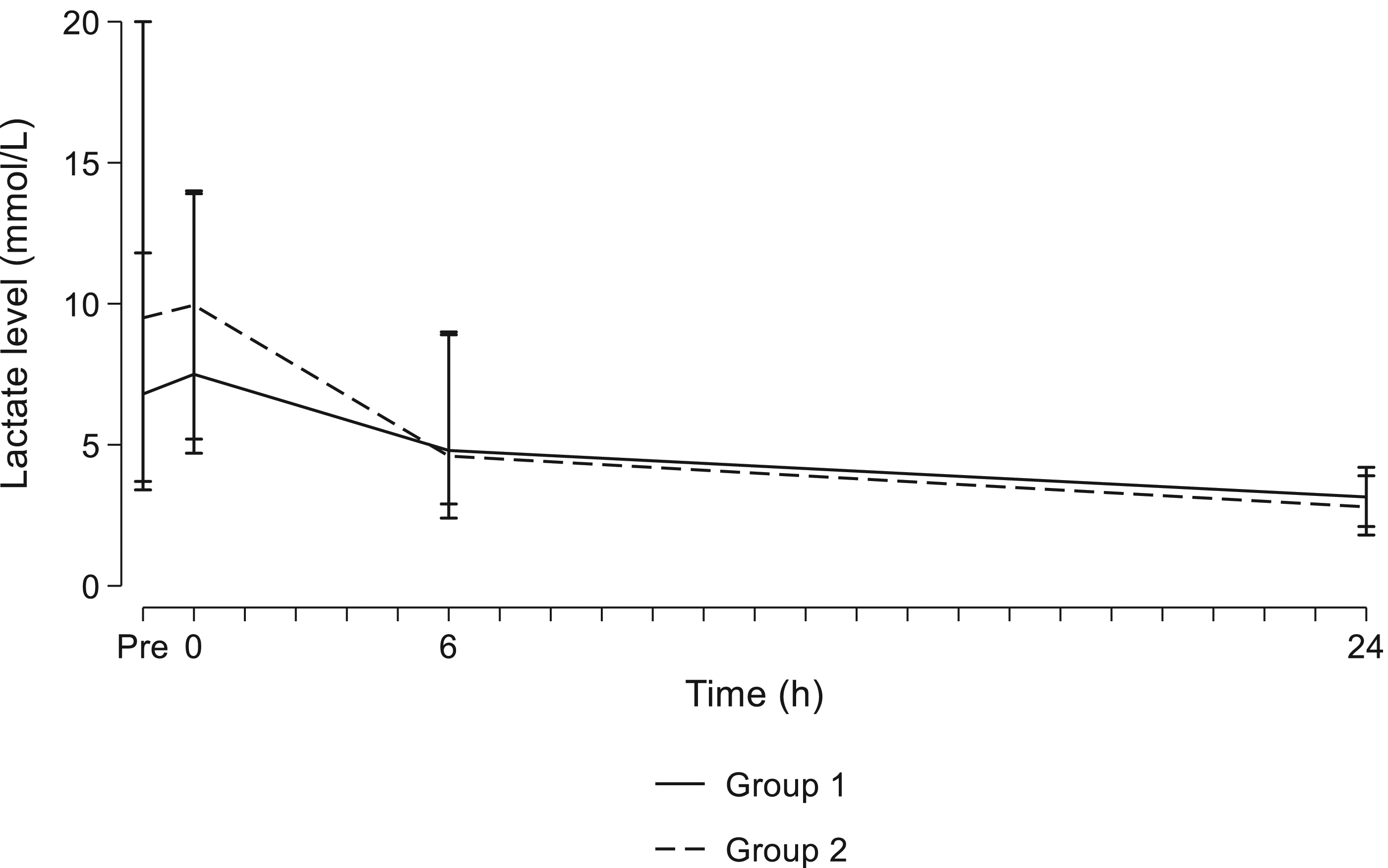
Survival at 3 months was 38% in Group 1 vs 31% in Group 2 (log-rank p = 0.678) (Figure 3). Kaplan‒Meier survival estimates comparing patients who had extracorporeal membrane oxygenation (ECMO) insertion in the operating room (Group 1) vs. pediatric cardiac intensive care unit (Group 2).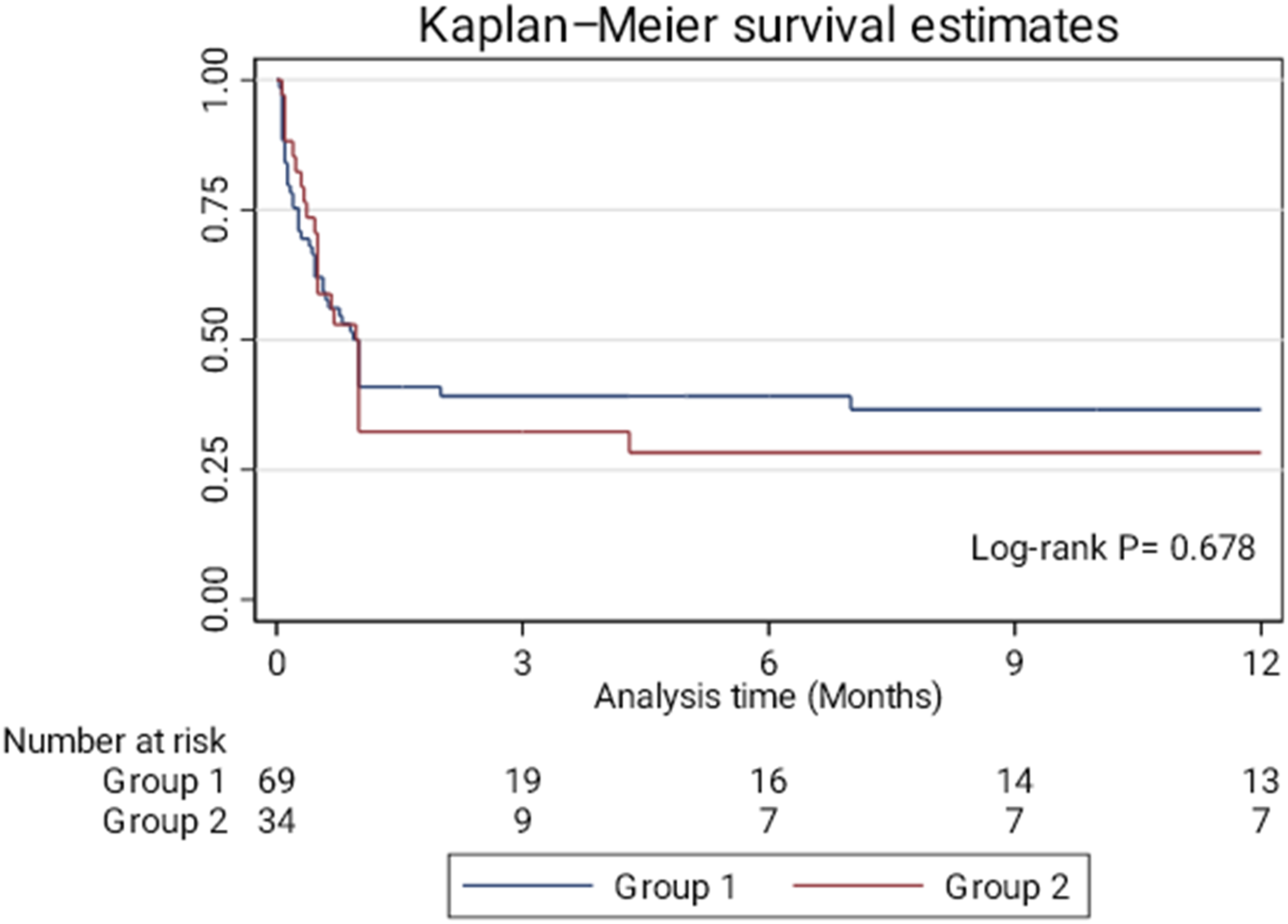
Factors affecting mortality
Multivariable logistic regression for factors affecting hospital mortality.

CI, confidence interval; ECMO, extracorporeal membrane oxygenation; PCICU, pediatric cardiac intensive care unit; OR, odds ratio; VIS, vasoactive inotropic score.
Discussion
ECMO in patients with congenital heart disease is still associated with high morbidity and mortality rates. Several studies have demonstrated variable risk factors predicting mortality in those patients. Early ECMO insertion before end-organ damage could be associated with better outcomes. 10 The effect of ECMO initiation in the OR compared to the PCICU on hospital mortality has not been thoroughly evaluated. This study characterized patients who had ECMO insertion in the OR or PCICU after the repair of congenital cardiac lesions. Additionally, we compared the outcomes in those patients and assessed factors affecting hospital mortality. ECMO insertion in the OR has the potential advantage of rapid insertion because of the availability of the surgical team and the equipment. Additionally, insertion in OR mostly occurs before clinical deterioration and cardiac arrest and is a continuation of the cardiopulmonary bypass. ECMO insertion in the OR before heparin reversal and hemostasis could increase the risk of bleeding. Pizarro and colleagues reported that ECMO initiation outside the OR was a risk factor for mortality after Norwood palliation. 11 We reported a significantly higher prevalence of cardiac arrest in patients who had ECMO insertion in the PCICU. Re-exploration for bleeding was higher in patients who had ECMO in the OR, with no difference in mortality between groups. The lack of difference in hospital mortality between the place of ECMO initiation in our study could be explained by early insertion before clinical deterioration and the availability of the equipment and trained personnel in the PCICU. Timely ECMO initiation can be demonstrated in both groups by the absence of differences in the biochemical parameters between groups.
ECMO support can be used to support children in all age groups. 12 This study’s most common age groups were neonates and infants, with no difference in age groups between patients who had ECMO insertion in the OR and PCICU. Additionally, age group was not a predictor of mortality in our cohort. The survival rate was lower in neonatal ECMO compared to other age groups, according to the ESLO report (42% vs. 52%, respectively). 13 However, this report included patients with diagnoses other than postcardiotomy cardiogenic shock. In our series, the mortality rate among neonates was 72%, 56% in infants, and 62% in older children. Morris and associates found that neonates and male sex were risk factors for mortality. 14
We did not report demographic, clinical, or disease-related factors associated with hospital mortality. This study included 13 patients with a single ventricle, with a nonsignificantly higher prevalence in patients with ECMO initiation in the PCICU (p = 0.07). Alsoufi et al. reported in their 100 postoperative pediatric ECMO series that survival was 32% in patients with single ventricles. 15 Several studies reported worse outcomes in patients with single ventricles supported with ECMO.5,16–19 Several other risk factors were reported to increase hospital mortality, including total anomalous venous connection, 20 residual lesions, 21 long bypass times,22,23 low birth weight, 24 and prematurity. 25
In this study, pre-ECMO low pH and high lactate levels during ECMO predicted mortality. Several biochemicals were found to be significant predictors of mortality in pediatric postcardiotomy ECMO, including pre-ECMO parameters. 26 Walter and associates reported elevated creatinine and blood urea nitrogen on ECMO as risk factors for mortality. 22 In Kolovos et al.’s study on 74 pediatric patients who received postcardiotomy ECMO, high lactate 48 h after ECMO initiation predicted mortality, 26 and Polimenakos reported that high lactate 24 h after ECMO initiation was an independent risk factor for mortality. 27 Alsoufi and colleagues found that delayed lactate normalization predicted mortality in postcardiotomy pediatric ECMO. 15 Similar to our study, Howard and associates found that pre-ECMO low pH (<7.17) was a risk factor for mortality. 25 In their study on 47 children with veno-arterial ECMO, Chen and colleagues found that a high lactate level 12–24 h after ECMO insertion was an independent predictor of mortality, and the cutoff point was 48.6 mg/dl. They also found that venous pH, HCO3, CO2, base excess, and O2 saturation did not affect mortality. 28 Our study demonstrated that biochemical parameters before and during ECMO were more prevalent in predicting hospital mortality than clinical, pathological, and demographic factors. Moreover, timely ECMO initiation in a well-prepared PCICU yielded comparable results to ECMO initiation in the OR.
Study limitations
The study is limited by the retrospective design with its known biases, and the difference between groups could be related to patient-specific variables or even to unmeasured variables. However, ECMO is not a frequent procedure, and the study duration is over 10 years; therefore, prospective randomized studies on ECMO patients are difficult. The study is also limited by the single-center experience. The characteristics of our patients and the center facilities could make our results not generalizable to all centers.
Conclusions
Poscardiotomy ECMO support in congenital cardiac lesions is still associated with high mortality rates. Mortality in patients with ECMO initiation in the OR was comparable to those who had PCICU ECMO. Pre-ECMO low pH and high lactate during ECMO could predict hospital mortality.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.