
Abstract
Introduction
Intra-aortic balloon pump (IABP) insertion for diminished myocardial function is standard of care in cardiac surgery. Previous studies have suggested a possible benefit to IABP support before surgery with regards to outcomes and complications. However, there are conflicts with other studies suggesting no significant benefit. Optimal time of insertion, whether preoperative or perioperative (intra-operative and post-operative), has yet to be defined.
Methodology
A retrospective, hospital records-based chart review was conducted for patients admitted to our center from January 2015 to December 2019 for coronary bypass surgery necessitating IABP insertion. Cases were stratified according to the timing of insertion and analyzed according to surgical outcomes and complication rates.
Results
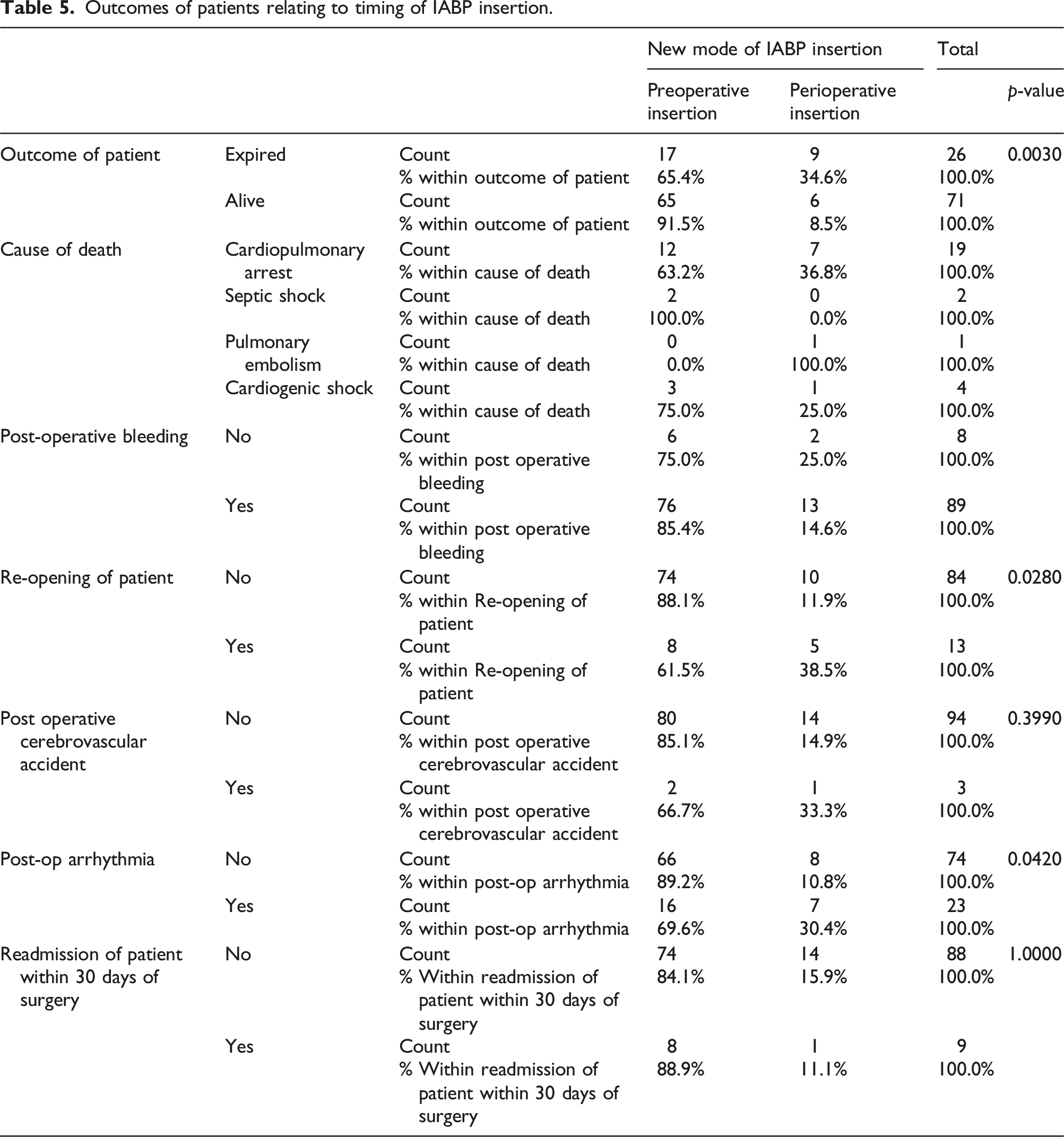
Out of 97 patients, 84.5% underwent preoperative IABP insertion while 15.5% of patients received perioperative (Intra-operative or post-operative) insertion. In-hospital mortality was significantly higher in patients with perioperative IABP insertion as compared to the preoperative group (60% vs 20.7%, p = 0.003). However, there were no significant differences between 30-day readmission rates in the two groups (9.8% vs 6.7%, p = 1.000). Length of stay was also higher in patients with preoperative insertion of IABP (p = 0.032), with no significant difference in ICU stay (p = 0.107). Perioperative IABP patients had higher rates of arrhythmias (46.7%, p = 0.042) and reopening of patient (33.3%, p = 0.028).
Conclusion
Our study shows improved mortality in patients with preoperatively inserted IABP. This may be beneficial for high-risk patients undergoing CABG surgery. Expanding the use of IABP before CABG in third world countries such as Pakistan may improve overall survival for patients.
Introduction
The intra-aortic balloon pump (IABP) is one of the most commonly used mechanical circulatory assist devices in patients undergoing coronary artery bypass grafting (CABG) with high risk of peri-operative morbidity and mortality. 1 It improves coronary blood flow, reducing left ventricular load and improving oxygen supply to the myocardium. 2 It provides critical temporary support to the left ventricle and prevents ischemic heart failure. 3 In addition to its positive impact on the cardiac tissue, IABP also possess some other technical advantages including ease of implantation, widespread availability, lower complications and greater cost-effectiveness as compared to other temporary mechanical circulatory support (TMCS) devices. 4 The main indications for IABP insertion are cardiogenic shock (CS), low-output cardiac syndromes post-open heart surgery, medically refractory ischemia or angina, left main coronary stenosis and decreased left ventricular ejection fraction. 5
Other TMCS devices to support compromised hemodynamics includes a pulsatile percutaneous ventricular assist device (the iVAC), veno-arterial extra-corporeal membrane oxygenation (ECMO), iVAC, Impella and Tandem Heart percutaneous ventricular assist device. 6 However due to technical difficulties, unavailability of expertise and high cost of other mechanical circulatory assist devices, IABP is the only mechanical circulatory assist device available and that too in only a few centres across third world countries like Pakistan. 7
Recent studies conducted in this regard showed improved surgical outcomes with peri-operative IABP insertion in patients undergoing CABG with both severe and mild left ventricular dysfunction.3,8,9 However it is not considered as a gold standard as multiple studies have shown increased complications such as increased risk of bleeding, reoperation, prolonged ventilation and ICU stay. 1 A recent meta-analysis showed improved outcomes with reduced mortality and reduction in major adverse cardiac and cerebrovascular events (MACCE) in patients undergoing CABG. 10 A recent study showed 1.6% reduction in mortality with IABP in patients undergoing CABG. 1 The 2011 American Heart Association guidelines recommended the use of IABP in patients with left main coronary artery disease, a left ventricular EF of <35% or patients who are undergoing reoperation in addition to certain well-established indications. 3 However the effect of use of IABP in the peri-operative period still remains controversial.11,12
There is very scarce data available on peri-operative usage of IABP and its outcomes especially from Indo-Pak region. 7 Two previous studies have been reported from our institute; one on the peri-operative usage of IABP in patients undergoing CABG with limited number of patients (n = 15) 13 and other on the overall usage of IABP in CS undergoing percutaneous coronary intervention. 7 Hence the importance of this study is to share our experience of IABP insertion from a low-middle income country and its overall impact on patients’ short-term peri-operative morbidity, mortality and post-operative outcomes and the how the timing of its insertion (pre-operative vs peri-operative) affected the overall patient outcome. It’s a first study of its kind from our region as none of the previous studies from our region have evaluated this aspect of IABP.
Materials and methods
This was a single center, retrospective study conducted at the Department of Cardiothoracic Surgery, Aga Khan University Hospital. Prior to this study, ERC exemption was sought. The confidentiality and anonymity of the participants was ensured and the data was coded. Researchers were responsible for the excellence and integrity of this project. All the patients undergoing CABG and IABP insertion in same hospital stay in last 5 years were included in the study from January 2015 till December 2019.
The approximate number of patients that had presented in our institute in last 5 years and had undergone CABG and had an IABP insertion were 130 patients but due to incomplete medical records 33 patients were excluded from the study. Non-probability consecutive sampling technique was used. Data was collected retrospectively by reviewing patient’s medical records and was recorded on pre-designed performa. Date and timing of IABP insertion and date of surgery and its complications were noted by reviewing patients Intensive Care Unit data sheets and daily progress notes and they were followed until the day of discharge or 30th post-operative day and if discharged from hospital, 30-day follow-up for complications was done through file review of clinic follow ups.
All the patients whose age was greater than 18 years, and all those who received IABP preoperatively, intra-operatively or post-operatively and underwent emergency or elective CABG with or without other open-heart procedures were included in the study, while those patients who received IABP and underwent percutaneous coronary intervention or those with incomplete medical records were excluded.
Statistical analysis
Retrospective, hospital-based chart review with two independent data collectors was done in order to ensure data accuracy. Cases were then stratified according to the timing of insertion and divided into two groups that is either pre-operative or peri-operative (intra-operative and post-operative) and analyzed according to surgical outcomes and complication rates. Statistical analysis was conducted using SPSS Version 23.0 and STATA Version 16.0; all statistical tests were two-tailed and p-value of <0.05 was taken to be significant. Student’s t test was used to compare means for parametric data, while Mann-Whitney U test was used for non-parametric data. Continuous variables were described with means, standard error, and 95% confidence intervals reported.
Results
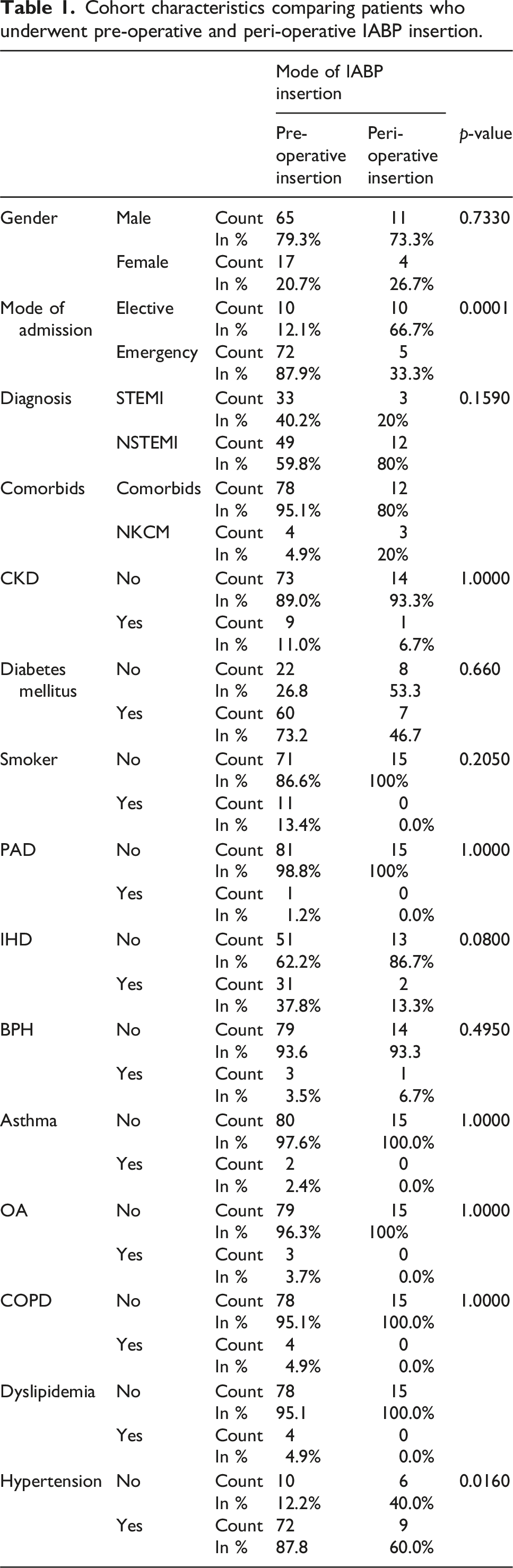
Cohort characteristics comparing patients who underwent pre-operative and peri-operative IABP insertion.
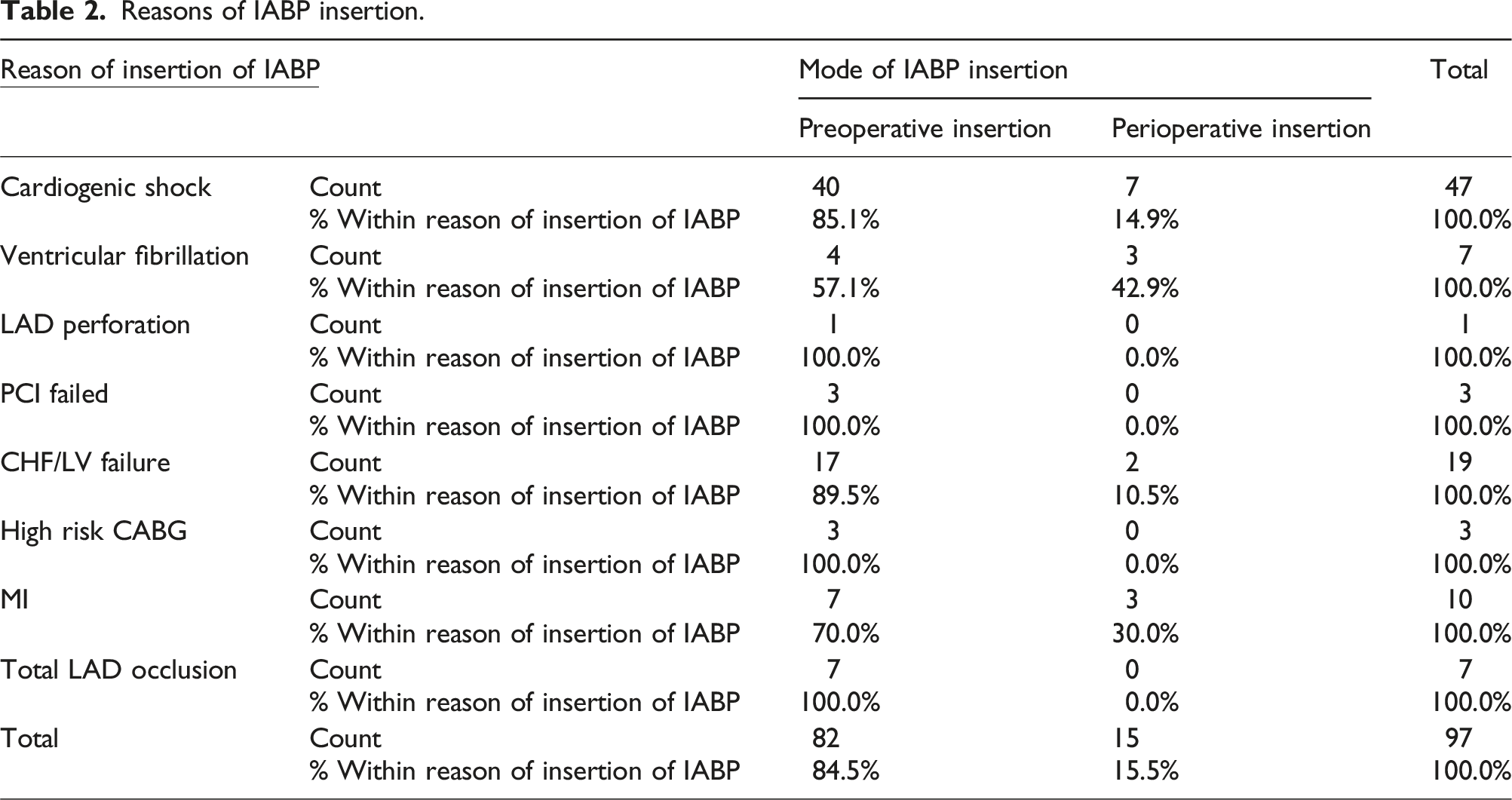
Reasons of IABP insertion.
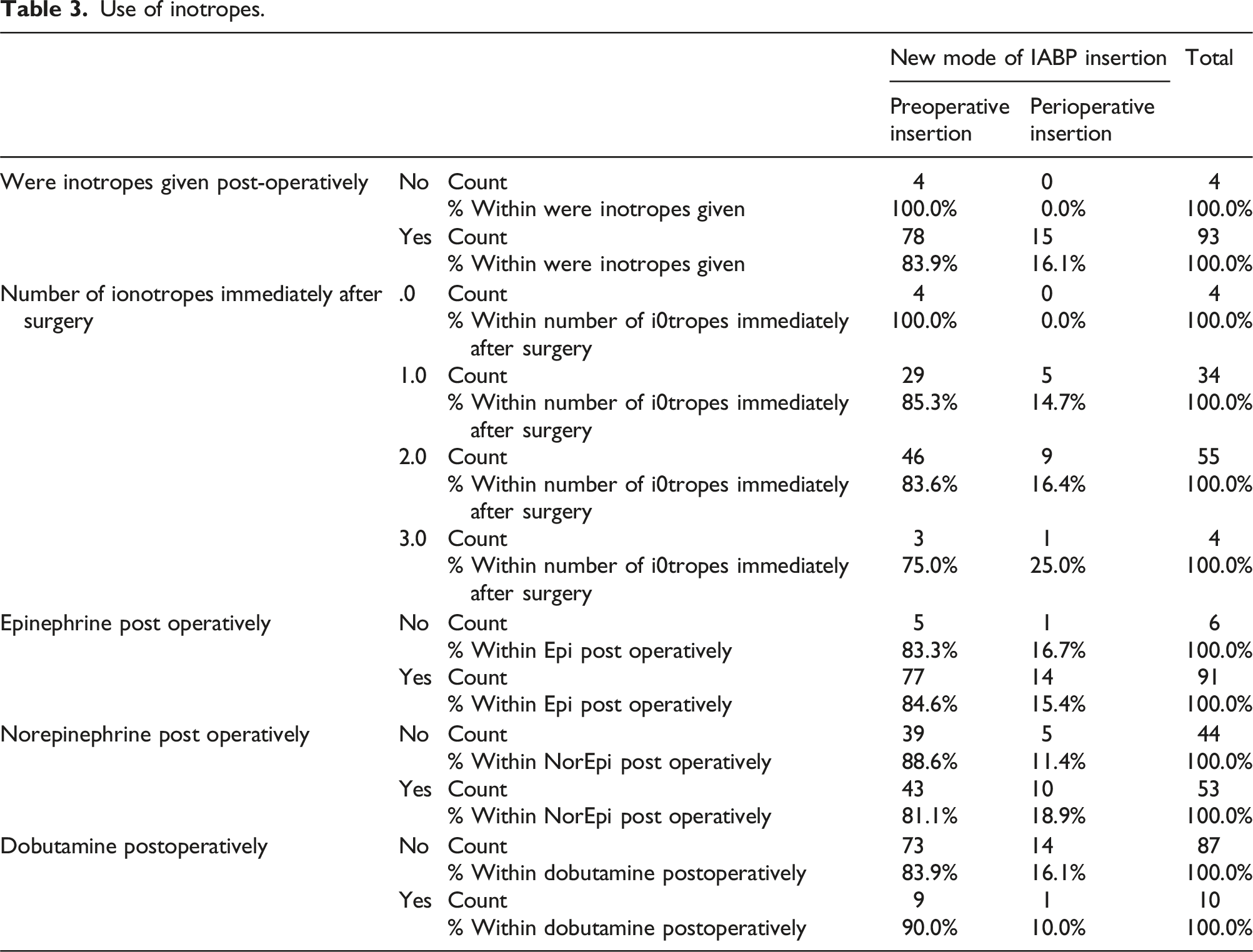
Use of inotropes.
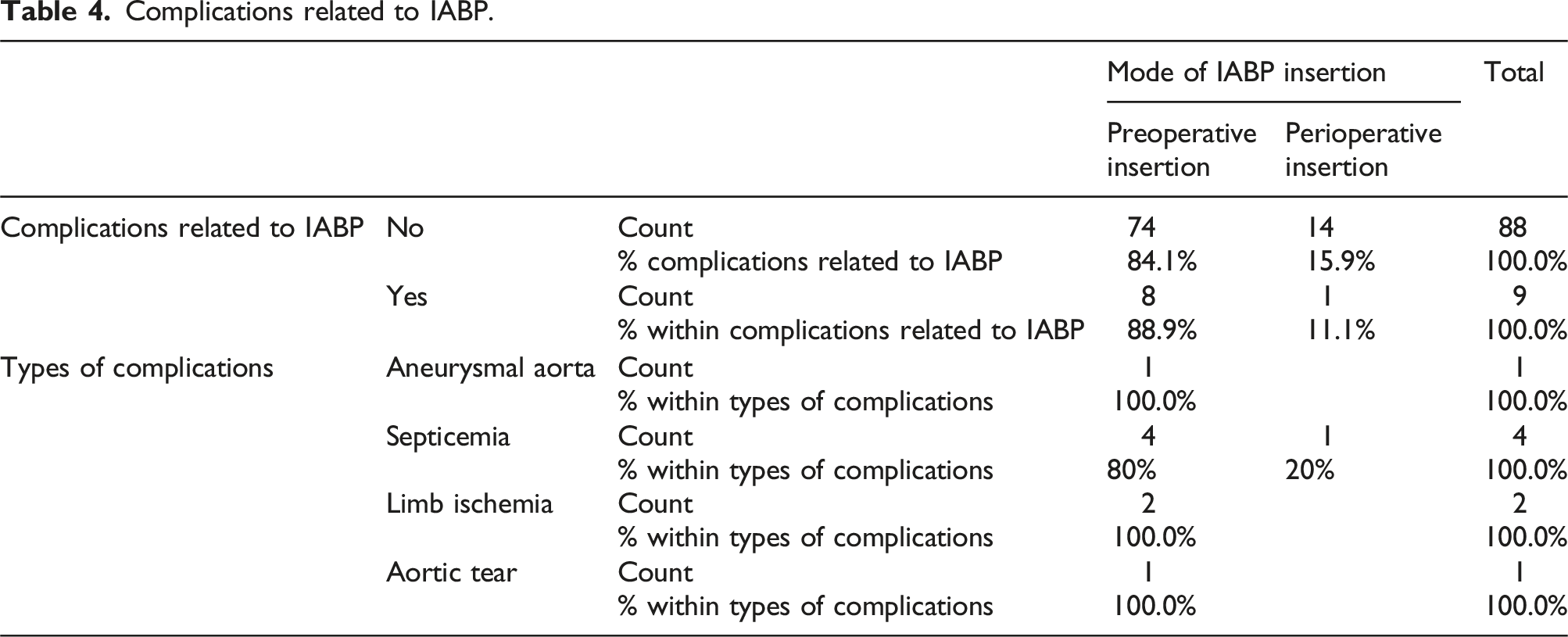
Complications related to IABP.
However, there were no significant differences between 30-day readmission rates in the two groups (9.8%, n = 8 vs 6.7%, n = 1), (p = 1.000). Length of hospital stay was higher in patients who were alive with preoperative insertion of IABP (p = 0.032), with no significant difference in ICU stay (p = 0.107) (Figure 1). Comparison of outcomes showing difference between preoperative and peri-operative insertion of IABP.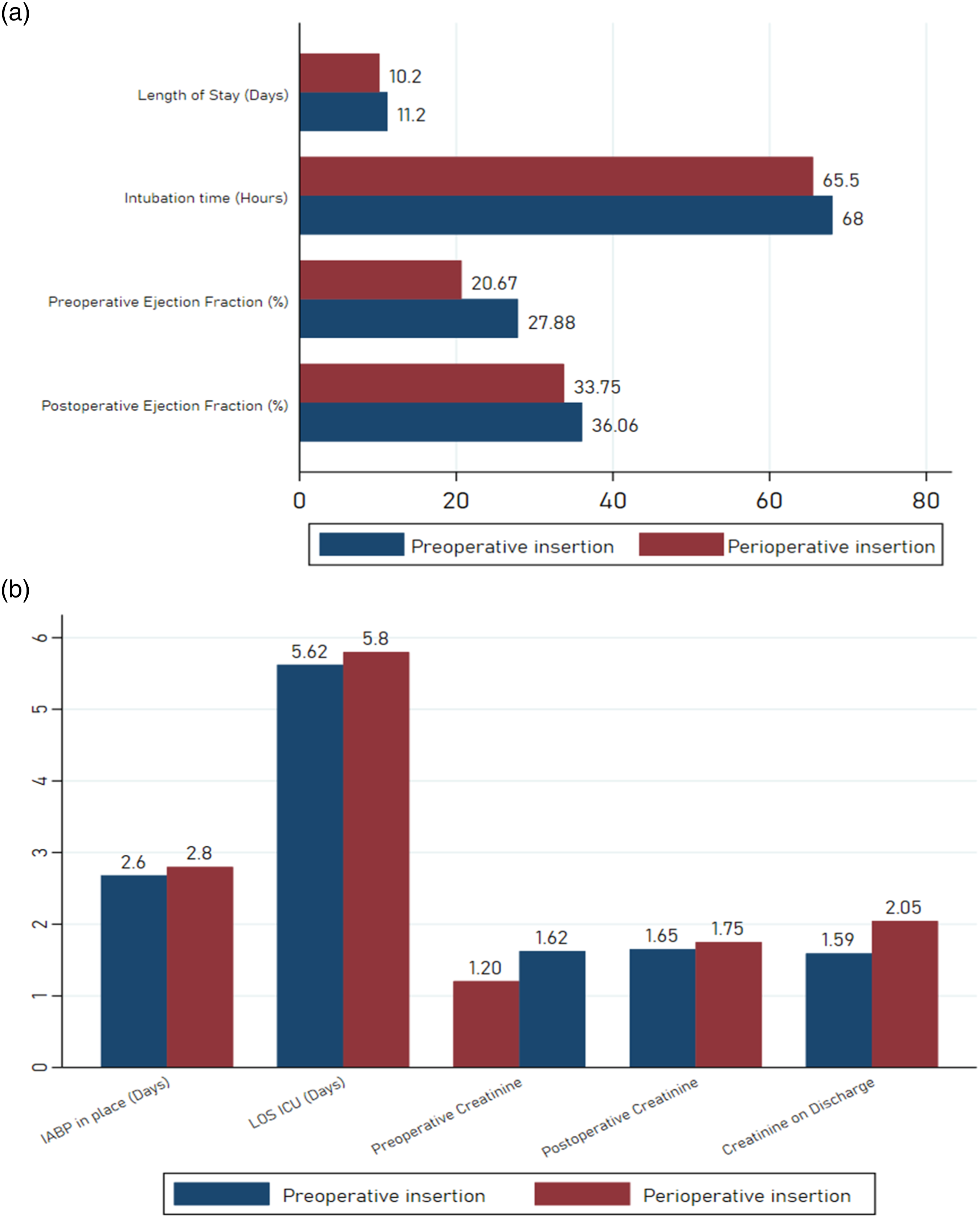
Outcomes of patients relating to timing of IABP insertion.
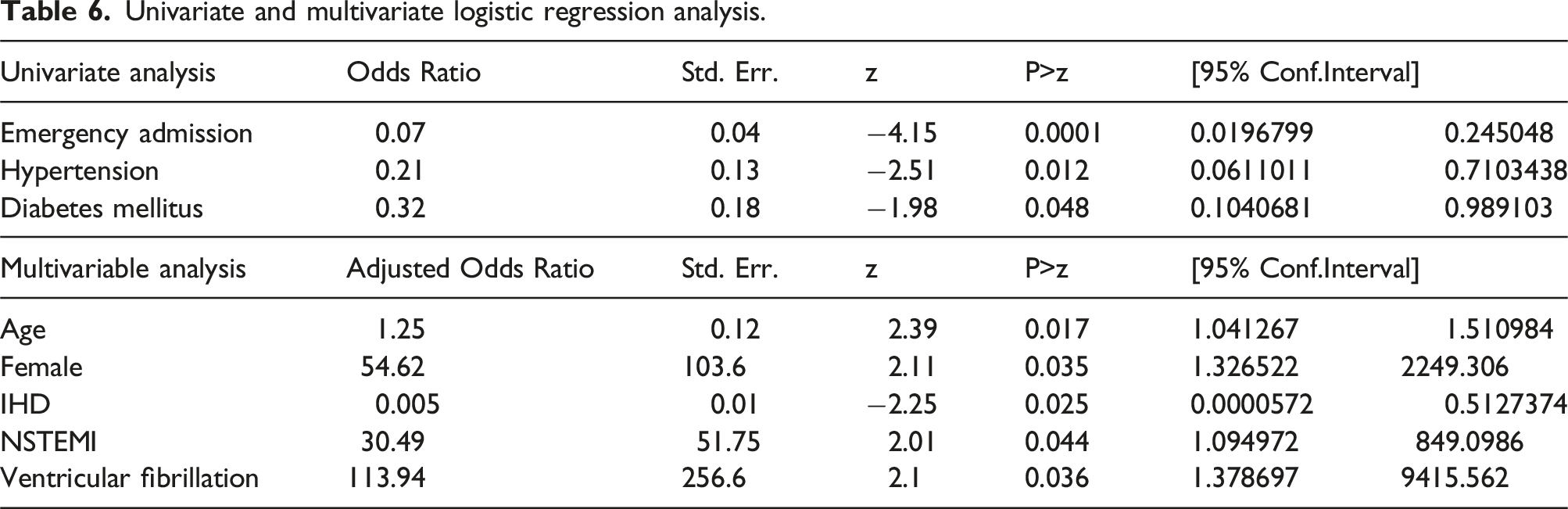
Univariate and multivariate logistic regression analysis.
Discussion
The use of IABP in patients undergoing CABG has been a matter of discussion with controversial results. Several studies have been carried out all over the globe, which highlight the advantages and disadvantages of IABP support. But very few studies have been done which emphasize on the timing of the placement of IABP support and its effect on postoperative outcomes of the patient.
In our retrospective study, we analyzed all the patients undergoing CABG with IABP placement within 5 years and concluded that out of total 97 patients, 77 of them underwent emergency CABG. Out of all the patients 84.5%, (n = 82) had preoperative insertion of IABP and 15.5%, (n = 15) had perioperative IABP insertion. In a study done by Brucu et al it was concluded that, early use of IABP in CS was associated with significant improvement in 30-day mortality regardless of the etiology of CS. 4 It was noticed in our study, about 48.5%, (n = 47) of our patients had CS due to which IABP was placed. IABP therapy is still used in cardiac surgery despite recent evidence from the IABP Shock II trial that could not prove a survival benefit of IABP in CS following myocardial infarction. 14
In terms of post-operative mortality, our study showed that the patients who had IABP inserted preoperatively had lower mortality rate as compared to those who had perioperative insertion of IABP. A 30-day mortality rate was assessed and mortality rate appeared to be higher in the perioperative group since 91.5%, (n = 65) patients with preoperative IABP insertion survived while only 8.5%, (n = 6) patients with perioperative IABP insertion survived. A recent meta-analysis by Dyub et al. 15 showed lower mortality and hospital length of stay in the preoperative group. However, in our study, the length of hospital stay was increased in the preoperative group, while the rate of readmission within 30 days and length of ICU stay was the same in both groups similar to the literature available.
About 9.3%, (n = 9) patients in our study developed complications of IABP insertion, the most important complications were septicemia (50%, n = 4), limb ischemia (25%, n = 2), aortic aneurysm (12.5%, n = 1) and aortic tear (12.5%, n = 1). However, if patients who are at higher risk of developing postoperative complications related to IABP insertion are identified early on and proper postoperative care and strict monitoring is carried out, the chances to develop complications related to IABP may be decreased. A study done in 2018, showed that the overall incidence of vascular complications ranged from 0.94% to 31.1%. 15
A recent meta-analysis reported that prophylactic IABP reduced mortality and MACCE in high-risk CABG patients. 1 MACCE noticed in our study included death due to cardio-cerebral events, cerebrovascular events (3.1%, n = 3, p = 0.399), and arrythmias (23.7%, n = 23, p = 0.042). Total mortality was 26.8%, (n = 26), out of which 73.1%, (n = 19), died due to cardiopulmonary arrest while 15.4%, (n = 4) died due to CS. In a study done in 2019, major adverse cardiac or cerebrovascular events (MACCE) occurred in 3.8% overall (including after discharge), with a 5.9% MACCE in the prophylactic IABP group. 1 Taking into consideration that the large number of patients included in our study presented with CS and more than half of patients required emergency CABG, with several comorbids, such as DM (69.1%, n = 67), HTN (83.5%, n = 81), CKD (10.3%, n = 10), IHD (34.0%, n = 33), dyslipidemia (4.1%, n = 4). Approximately, (11.4%, n = 11) were smokers, and 2.1%, (n = 2) had asthma, while 4.1%, (n = 4) had COPD. About (79.4%, n = 77) underwent emergency CABG, and about 37.1%, (n = 36) had STEMI, the expected MACCE and mortality was much higher than reported.
Reopening due to bleeding in CABG patients is one of the important post-operative complications. We noticed in our study, that about 92.7%, (n = 76) patients who had preoperative IABP insertion had only 9.8%, (n = 8) were reopened due to bleeding while in the group who had perioperative IABP insertion 86.7%, (n = 13 out of 15) were bleeding and 33.3%, (n = 5) were reopened. Although significant (p-value of 0.028), this could be due to the fact that patients who underwent emergent surgery received acute coronary syndrome protocol closer to time of surgery, than those who first underwent pre-operative IABP placement and had an urgent surgery. In a study conducted in 2019, the results showed that there were no significant differences in reoperation for bleeding in patients with IABP as compared to those without IABP. 1
Cardiac surgery patients often need inotropic support to establish hemodynamic stability and adequate oxygen supply. 16 About 7.3%, (n = 7) patients in our study, required preoperative epinephrine while 18.3%, (n = 15) required preoperative norepinephrine. On the other hand, about 95.9%, (n = 93) patients required inotropes post-operatively from which, 56.7%, (n = 55) were on dual inotropes that is epinephrine and norepinephrine, 35.1%, (n = 34) were on single inotropic support and 4.1%, (n = 4) required triple inotropic support, (epinephrine, norepinephrine and dobutamine). According to the recent literature, it has been deduced that inotropic support, IABP and adequate volume management during surgery and post-surgery period in ICU has led to better and early hemodynamic stability. 16
In regards to the aforementioned findings, our study has shed light upon the need of IABP insertion in patients undergoing CABG and its overall effect on decreasing the postoperative mortality and morbidity in high risk patients. Furthermore, prophylactic, preoperative IABP insertion in high-risk patients undergoing cardiac surgery as was preferred in our institute decreases mortality and morbidity further. Preoperative IABP insertion should be considered in high-risk patients undergoing CABG. 17 as opposed to certain studies which were carried out. Yu et al reported that preoperative IABP before CABG surgery is associated with increased in-hospital morbidity and longer postoperative ICU stay as compared to patients without IABP support. 17
Limitations
One of the major limitations of our study is a single center retrospective cohort analysis. All the patients that were selected had IABP inserted and no control group was added. Also there may be a selection bias effect as time from admission to time of surgery was not assessed as this could determine whether patients receiving IABP pre-operatively were more or less stable than the peri-operative group. The effect of IABP on postoperative morbidity and mortality was analyzed by using the use of inotropes, the postoperative complications, length of stay, reopening and the rate of readmissions, however, the timing of IABP insertion is still a questionable debate due to the fact that this retrospective study is based on a smaller scale. Hence, in order to adequately determine the effect of IABP on overall mortality and morbidity and precisely assess the timing of IABP placement in relation to outcomes, multi-centric studies need to be carried out with increased number of participants including control groups with greater follow up times.
Although half of the patients receiving IABP in the peri-operative group were electively admitted for surgery, the major limitation of this study was that we did not assessed the intra-operative complications or technical difficulties that may have led to IABP placement in the peri-operative group. This can lead to increase morbidity and mortality post-operatively in the peri-operative group.
Conclusion
Preoperative prophylactic use of IABP was related to a decline in overall short-term mortality and morbidity in high-risk patients undergoing CABG. Our study shows improved survival in patients with preoperatively inserted IABP. Complication rates were also higher in the perioperative group. This can be beneficial for high-risk patients undergoing CABG surgery in third world countries where iVACs are either unavailable or are not affordable. Expanding the use of IABP before CABG in resource-limited third world countries such as Pakistan may improve overall survival for patients. However further prospective. multi-center studies are required especially which determine the intra-operative complications that can lead to IABP insertion in the peri-operative group before it can be concluded that prophylactic IABP insertion in high risk patients have better outcomes.
Footnotes
Author contributions
Abdul Ahad Sohail: Original draft, critical review, literature search.
Areeba Samejo: Original draft, literature search, data collection.
Areeba Samejo: Original draft, literature search, data collection.
Hamza Bajwa: Original draft, literature search, data collection.
Rida Wahab: Original draft, critical review, literature search. Narmeen Asif: Original draft, critical review, literature search.
Hina Inam: Original draft, critical review, literature search.
Syed Shahabuddin: Original draft, critical review, literature search.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The ethical committee of Aga Khan University Hospital has approved this study.