
Abstract
Background
Current medical simulators for extracorporeal membrane oxygenation (ECMO) are expensive and rely on low-fidelity methodologies. This creates a challenge that demands a new approach to eliminate high costs and integrate with critical care environments, especially in light of the scarce resources and supplies available after the COVID-19 pandemic.
Methods
To address this challenge, we examined the current state-of-the-art medical simulators and collaborated closely with Hamad Medical Corporation (HMC), the primary healthcare provider in Qatar, to establish criteria for advancing the cutting-edge ECMO simulation. This article presents a comprehensive ambulatory high-realism and cost-effective ECMO simulator.
Results
Over the past 3 years, we have surveyed relevant literature, gathered data, and continuously developed a prototype of the system modules and the accompanying tablet application. By doing so, we have successfully addressed the issue of cost and fidelity in ECMO simulation, providing an effective tool for medical professionals to improve their understanding and treatment of patients requiring ECMO support.
Conclusions
This paper will focus on presenting an overall ambulatory ECMO simulator, detailing the various sub-systems and emphasizing the modular casing of the physical components and the simulated patient monitor.
Introduction
Among the procedures employed in the critical care unit, extracorporeal membrane oxygenation (ECMO) is considered one of the most intricate techniques. 1 The procedure involves providing cardiopulmonary support to patients with critical lung or heart conditions as they recover. 2 The reliance on ECMO for survival means it must operate continuously with minimal errors. Unfortunately, ECMO is often plagued by problems, such as technical deficiencies of the devices or mistakes made by clinical care staff who may be inexperienced with the procedure.3,4 To mitigate these risks, ECMO practitioners must possess the necessary scientific knowledge, mental preparedness, and personal attributes to handle critical situations. 5
Simulation-based training (SBT) has been employed to train ECMO personnel since ECMO is regarded as a high-risk procedure. 6 Most ECMO centers that utilize SBT rely on Anderson’s simulation model, which entails an ECMO circuit containing red fluid and a distinct mechanism for adjusting circuit volume and introducing air via a syringe. 7 The circuit is manually manipulated during the simulation session to simulate emergency scenarios, such as hypovolemia, which can be replicated by draining fluid from the circuit.
ECMO simulators provide a realistic training environment for healthcare professionals to develop the knowledge and skills necessary to operate the ECMO system. 8 Several ECMO simulators are available, including physical models, computer-based simulators, and hybrid simulators. Physical models are the most basic type of ECMO simulator and physically represent the ECMO system. Computer-based simulators are more advanced and use software to simulate the function of the ECMO system. Hybrid simulators combine physical and computer-based components to create a more realistic training environment.
While using real ECMO circuits and simulators has some benefits, it also has significant drawbacks. Low-fidelity simulations can undermine the intended scenario rather than enhance it. 9 Many important ECMO parameters cannot be monitored or replicated unless intricate modifications are made, or real blood is employed. To overcome these limitations, some consumer ECMO simulators use a wireless screen to showcase significant parameters. However, a discrepancy exists between the true parameters displayed on the ECMO machine and those displayed on the simulated screens. Furthermore, replaceable ECMO pieces, for instance, the oxygenator, are costly, making them difficult or impossible to substitute with continuous SBT.
The primary goal of high-fidelity training activities is to create an immersive experience for learners, preventing adverse learning outcomes and forming the basis for successful SBT. However, implementing high-realism systems and configurations can be costly, demanding a substantial budgetary investment, especially considering the existing ECMO SBT techniques.
The proposed ECMO training framework presents several advantages, including reduced maintenance costs and expenses and enhanced customizability and expandability. The developed modular ECMO not only bears a physical resemblance to the actual machine but also emulates its functionality, replicating common emergency scenarios encountered during ECMO machine usage. This breakthrough has the potential to significantly support the effectiveness of new ECMO SBT programs, further enhancing the learning experience for their participants.
A self-contained and modular ECMO simulator is developed to overcome many obstacles, eliminating the need for an actual ECMO machine or its expensive circuit parts. The objective is to establish an ECMO environment where instructors can supervise, and learners can interact with.10,11 The initial investigation has concentrated on replicating the distinctive visual indicator of blood oxygenation color shift in ECMO simulation. The color shift was achieved by utilizing thermochromic ink, which changes its color shade based on temperature, to mimic the color alteration of blood as it undergoes oxygenation and filters out carbon dioxide. 12 To employ thermochromic ink in ECMO SBT, a control system for heating and cooling is necessary.
The primary objective of this paper is to present a comprehensive ambulatory ECMO simulator, which will be achieved by providing a detailed overview of its various sub-systems. The emphasis will be on the modular casing of the physical components and the simulated patient monitor. The paper will also highlight the significance of these sub-systems, their functions, and how they work together in the broader ECMO simulation. Overall, this paper seeks to provide a comprehensive understanding of the ambulatory ECMO simulator, including its design and functionality, which will be of value to medical professionals and researchers in the field.
The rest of this article is structured as follows: Section 2 summarizes previous research in the field. Section 3 details the design of the ECMO module, while Section 4 provides an overview of the latest results. Finally, Section 5 concludes the article with a summary of the findings.
Related works
To comprehend the intricacy of the technique and the interaction between ECMO settings and the patient, healthcare providers need hands-on experience with ECMO. The medical team must cooperate in an emergency to perform well-practiced swift interventions, known as SBT, to save patients. 1 Unfortunately, there is no standard simulation protocol for ECMO; hence training facilities use different simulation technologies and approaches. 1
The recognition of ECMO, particularly in light of the COVID-19 pandemic, has increased the demand for training in ECMO SBT.2,3 To meet this demand, training experts have utilized available equipment and practices to create as realistic SBT scenarios as possible, leading to the development of standard simulation practices in the literature.4,5
ECMO training-based simulators
In recent years, simulated ECMO circuits have become increasingly available, offering accessible and do-it-yourself solutions for replicating complex ECMO procedures for patients.6,13 Advanced options, such as the Orpheus perfusion simulator, have emerged, which leverage the intersection of medical sciences and engineering. The Orpheus simulator utilizes a simulated ECMO circuit and a modified mannequin to replicate the heart, arterial, and venous systems. 14 Additionally, the NIJMEGEN ECMO simulator is a mobile option that can emulate typical parameters and is controlled wirelessly. 15 Other cost-effective mannequin simulators, such as the one developed by Puslecki et al.16,7 allow for pressure simulation and cannulation training.
Several commercial products have entered the ECMO SBT market, including EigenFlow and Parallel Simulator, which can manage standard circuit parameters and reproduce situations with real-time wireless control.17,18 Furthermore, products like the Medos Deltastream HC heater/cooler and the ParaTherm heater/cooler for intensive care units or patient transportation offer accurate temperature management for patients. 17
Han et al. 19 described the development and clinical use of an ambulatory ECMO system designed to support patients with severe respiratory or cardiac failure who require prolonged ECMO support. The authors discussed the system’s technical specifications and design, including miniaturized components and a portable control unit. They also described the preclinical testing of the system in animal models and the subsequent clinical trials in human patients. The authors reported successful outcomes in the clinical use of the ambulatory ECMO system, with no significant complications or adverse events reported. The development of a mobile ECMO system represents a promising advancement in the field of ECMO therapy and can potentially improve outcomes for critically ill patients. Because of its portability, this instrument could be used for ECMO simulation.
Limitation/gap found in the literature
Despite the aforementioned advancements, limitations exist, such as the dependence on expendable and costly parts, such as oxygenators, heat exchangers, and pumps, which are needed for proper SBT but are often prioritized for actual patients in an emergency. Furthermore, manually regulating the ECMO circuit might disrupt the desired suspense of disbelief. The need for real blood for simulation also damages the equipment, preventing the effective visualization of ECMO’s primary oxygenation function.
Additionally, one of the limitations of ECMO simulators is their inability to simulate all possible scenarios that healthcare professionals may encounter when operating the ECMO machine. ECMO simulators are limited by their programmed scenarios and may not allow healthcare professionals to practice managing rare or complex scenarios. Additionally, ECMO simulators do not replicate the emotional and psychological stress that healthcare professionals may experience. Using ECMO simulators may provide healthcare professionals with the necessary technical skills to operate the ECMO system. Still, it does not prepare them for the emotional and psychological challenges of managing a critically ill patient. Another limitation of ECMO simulators is their inability to replicate the patient-specific variability that healthcare professionals may encounter when caring for a patient on ECMO. Each patient is unique, and their response to ECMO may vary depending on their underlying condition, age, and comorbidities. ECMO simulators may not provide a realistic simulation of patient-specific variability and may not prepare healthcare professionals for the challenges of managing a patient on ECMO.
This paper presents a new ECMO simulator emphasizing blood modeling that promotes realism and cost-effectiveness. The simulator uses a thermochromic ink-enabled heater-cooler module controlled by a tablet application to recreate oxygenation, hypoxemia, and recirculation, enabling pioneering simulation fidelity at a low cost. Additionally, the major physical part of the system is mounted on a trolley with wheels to allow for mobility which offers several advantages. Mobile ECMO simulators can be easily transported to different locations, making them accessible to healthcare facilities in remote or underserved areas. Furthermore, mobile ECMO simulators can be customized to meet the specific needs of healthcare facilities, allowing for tailored training scenarios. A patient monitor simulator was also introduced to simulate real-life scenarios and provide realistic training sessions.
ECMO modules
The field of ECMO training is broad and complex, encompassing many criteria, characteristics, and situations that must be considered in the design of a training system. The concept for this project originated at Hamad Medical Corporation’s (HMC) intensive care unit, which provided vital insight into the limitations that led to the simulator’s design and deployment. In accordance with their needs, we utilized our engineering knowledge to design the system and included additional modules that were not initially necessary. Several self-imposed constraints, including modularity and wireless communications, were considered to streamline the options and make the solution more accessible.
This research aims to address the challenges currently facing state-of-the-art ECMO simulators by developing a complete simulation and training system that includes both the patient and the ECMO equipment utilized by HMC. The mock machine closely resembles the genuine equipment on the outside, but its internal hardware components were designed to replicate ECMO’s functionality and emergency scenarios. The simulated ECMO machine’s hardware is fully adjustable, allowing complete control. A user-friendly system and an ECMO instructor tablet application were created to facilitate manual management and the development of customized practice situations. Furthermore, thermochromic ink can be utilized instead of animal blood, which changes color in response to temperature changes, providing a suitable imitation of blood circulation, oxygenation, and de-oxygenation. Using thermochromic ink will increase the flexibility and cost-effectiveness of the system while also providing a long shelf life.
Patient unit
In the domain of simulators, the patient unit assumes a preeminent position owing to its incorporation of various critical components such as the primary thermochromic loop control, de-oxygenation module, shattering module, bleeding module, and cooling unit. The bleeding module imitates the common occurrence of patient bleeding, known as hypovolemia, during ECMO support. Patient bleeding refers to fluid depletion within the circuit, causing the patient to experience bleeding through the chest bladder and vibrations in the tubes connecting them to the ECMO machine. To replicate this bleeding effect, a pump controls the movement of colored water from a separate tank into a designated bleeding bag, often connected to the patient’s bladder. The contemporary patient unit is outfitted with an advanced valve system that can be minutely manipulated to execute a specialized mode referred to as flushing. The primary function of the flushing mode is to automatically purge all thermochromic ink tubes and connections with water to prevent staining of the thermochromic ink powder within the liquid system, which may diminish the efficacy of subsequent simulation runs and result in obstructions. Utilizing the instructor application, the flushing mode can be initiated with a few simple directives. Previously, flushing was performed manually, requiring the disassembly and cleaning of the entire liquid system, which was both time-consuming and cumbersome. The valves in the system operate in a specific manner during regular operation. More details regarding the unit’s technical specifications can be found in. 20
A control board has been developed to regulate the patient unit’s thermochromic loop and other simulation modules. This board is responsible for receiving instructions from the instructor application and communicating them to each module via a central local database. Reading control values from the local database through the instructor application is a critical control board function.
To ensure that the control board can manage any additional modules that may be incorporated in the future, it has been designed with the following specifications: • A circuit for regulating power to the simulation modules. • A microcontroller with a clock speed of at least 50 MHz has been employed to analyze the database expeditiously and instantaneously communicate directives to the modules. • A Wi-Fi module has been integrated to connect to the local database.
The patient unit possessed a substantial framework with components affixed to an acrylic sheet, rendering it immobile. To overcome this hindrance, a novel solution was proposed, entailing the enclosure of the patient unit within a cart fashioned from transparent acrylic. Figure 1 depicts the 3D-printed rendition of the bespoke trolley housing the patient unit. The custom-built trolley accommodates all subsystems in a modular fashion. The patient and bleeding units are ensconced within individual acrylic boxes, complete with quick connect/disconnect liquid fittings and electrical plugs. The modular strategy facilitates prompt upgrades or maintenance of individual modules. Also, it enables the seamless integration of future modules to the existing patient unit without necessitating a complete overhaul of the patient unit trolley. Additional wheel casters can be added to enhance the portability of the other module boxes. The 3D model of the modular trolley.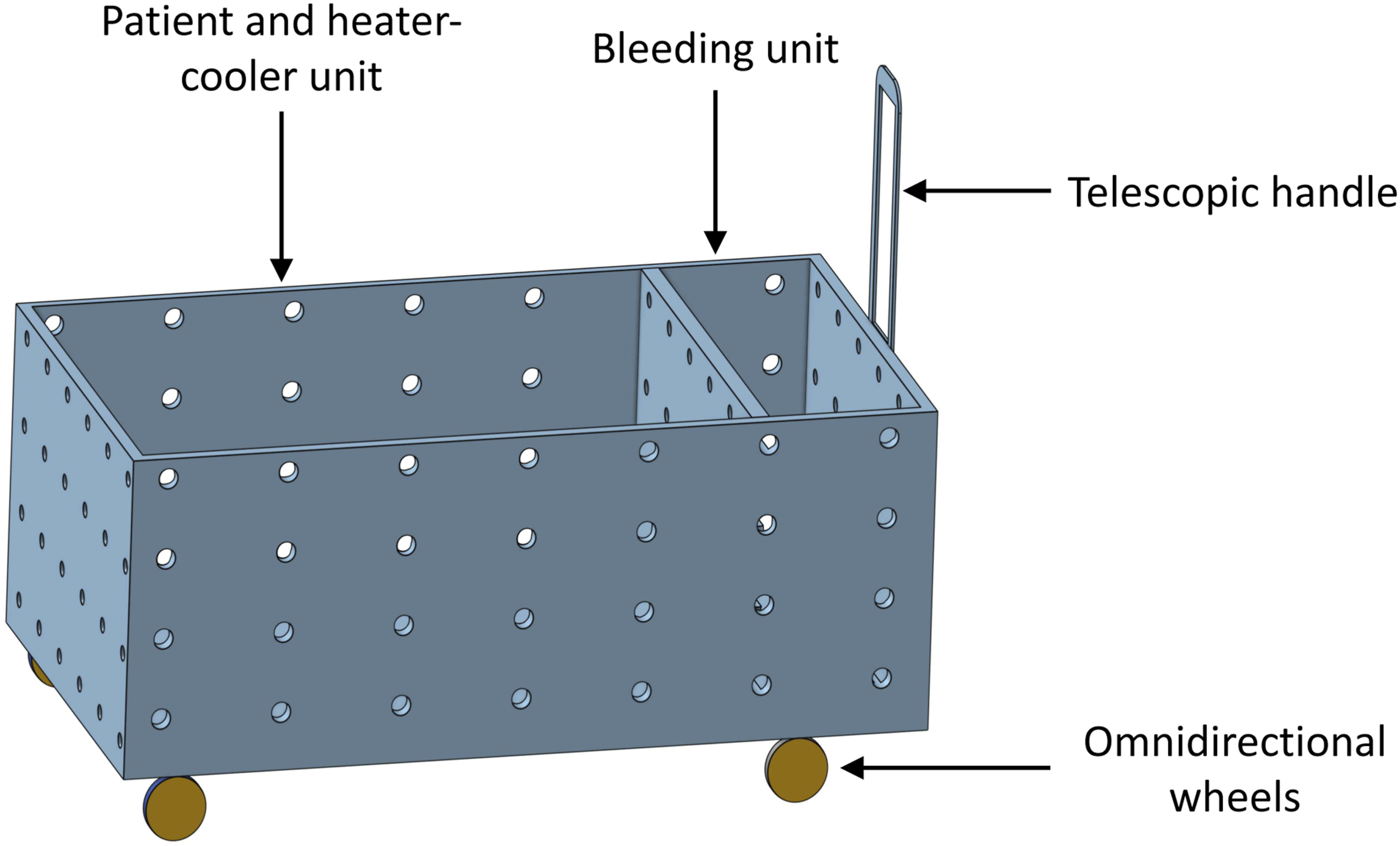
The new patient unit has been designed to require the fewest connections during its initial setup. Specifically, all connections have been routed inside the module boxes, with only a few external links necessary to establish connections between the modules or other units. This design approach reduces the complexity of the unit’s installation process and minimizes the potential for connection errors or malfunctions. Furthermore, this approach may lead to a more compact unit that is easier to transport and relocate as needed. However, there are potential trade-offs to consider, including increased difficulty in diagnosing and repairing internal connection failures and challenges in re-configuring or expanding the unit’s internal connections in the future.
Heater-cooler unit
The thermochromic loop plays a pivotal role in indicating the oxygenation status of blood that passes through the ECMO machine’s mock oxygenator. To achieve this, the heater-cooler unit heats the thermochromic loop, causing it to change color from a dark to a light red hue. This alteration in color represents the conversion of deoxygenated blood to oxygenated blood, providing a visual indicator of the oxygenation process. It requires a constant supply of cold water to regulate its temperature to enable the thermochromic ink to transition between colors accurately. This is essential for the ink to switch from a pale to a dark red color. Therefore, an external water cooler must be connected to the thermochromic ink loop’s patient unit. This setup presents a challenge as the patient unit requires external water and an external refrigerator to function correctly. To address this limitation, the research team has developed a compact water-cooling device that can be incorporated into the patient room, thus eliminating the need for an external refrigerator. Incorporating this water-cooling device enhances the patient unit’s portability, making it more efficient for use in various settings.
The heater-cooler unit was designed to overcome several challenges, including high flow rates and the heating impact that results from the heater side. To arrive at the optimal design, a trial-and-error process was employed. Initially, a preliminary experiment was conducted, utilizing three thermoelectric modules and two aluminum cases to house the cold water/coolant and the wasted heat from the thermoelectric. However, due to the mentioned challenges, three thermoelectric modules and an additional aluminum block were integrated into the design.
The final design features six thermoelectric modules surrounding an aluminum case that houses the cold water. Two aluminum cases are positioned on both sides of the rigid aluminum case to regulate the heat generated by the thermoelectric modules. This innovative sandwich approach was deemed necessary to address the challenges of high flow rates and heat transfer. The heater-cooler unit’s final design effectively balances the heating and cooling processes, ensuring the unit functions optimally. Further elaboration on the heater-cooler unit’s design and testing is found in. 21
Mock oxygenator
The oxygenator constitutes a crucial component of the simulation system. Its simulated counterpart facilitates the internal connection of various tubes within the main loop while presenting other physical cues under the instructor application’s control. Previously, the simulated oxygenator was entirely 3D-printed, including its internal tube connections, thereby giving rise to persistent leakage and color variation in the material due to the direct chemical interaction with the thermochromic ink. The newly devised design overcomes the aforementioned leakage issue. Additional unit information can be found in. 22
Tablet applications
The simulation system has been meticulously designed to cater to the needs of both learners and instructors. Two innovative software components have been developed to support the educational aspect: the instructor and the assessment tablet application.
Instructor application
The instructor application provides real-time monitoring of simulation modules and the ability to create customized training scenarios. The simulation modules communicate with the instructor application through the local network and CouchDB server, enabling them to save, load, and modify parameter values within the ECMO training system and synchronize parameters between the modules and the instructor application. More comprehensive information can be found in. 23
The sequence manager in the instructor application allows ECMO instructors to create numerous personalized emergency training scenarios. A sequence is a timeline incorporating software simulation modules, categorized into two types: generic and emergency. Generic modules serve as the foundational components of an ECMO scenario, while emergency modules replicate real ECMO circuit complications. The following are the emergency scenarios: 1. Hypovolemia: Simulates fluid loss in the ECMO circuit, leading to decreased blood volume and potential bleeding complications. 2. Line shattering: Mimics line shattering for a certain amount of time. 3. Power Failure: Imitates a power outage, requiring an appropriate response to maintain patient support and safety. 4. Oxygenator Failure: Mimics the failure of the oxygenator, resulting in inadequate blood oxygenation and potentially respiratory distress. 5. Air Embolism: Replicates the introduction of air into the circuit, which can obstruct blood flow and cause serious adverse effects.
Assessment application
An innovative tablet program for instruction and evaluation has been created, called the assessment application. The program offers a simple way to assess ECMO trainees’ work and provide them with targeted feedback, which speeds up the learning process. Further elaboration can be found in. 24
Simulated patient monitor
Patient’s vital signs data, such as heart rate, blood pressure, temperature, and SPO2, are essential health indicators. Hospitals and clinics use multi-function monitors to measure, record, distribute, and display this data to ensure high-quality patient care. These monitors have large capacities and can continuously and accurately monitor patients’ vital signs. Moreover, a simulated patient monitor is often included in ECMO training programs to create a more realistic experience. The simulated monitor functions similarly to an accurate patient monitor and displays data that can be used to train healthcare professionals to monitor and interpret the vital signs data of their patients. Thus, patient monitors are crucial for providing high-quality care in hospitals and clinics. Including simulated patient monitors in training programs can enhance the learning experience for healthcare professionals and improve their ability to monitor and interpret the vital signs data of their patients.
The simulated patient monitor has been designed to replicate the functionality of an actual monitoring device. This device can collect and display essential vital signs data, including heart rate, blood pressure (intrusive and non-intrusive), body temperature, respiration rate, oxygenation saturation, and the bispectral index system (BIS). The simulation was created using Processing Java, which offers the flexibility to use programming languages such as Java or Python to create visuals. The final version of this simulated patient monitor has been designed to run on raspberry pi 4B+ (RPi). It can be connected to a separate monitor to display the vital signs data the device collects. Figure 2 visually represents how the instructor application can manage the patient monitor. Overview of regulating the patient monitor process via the instructor application.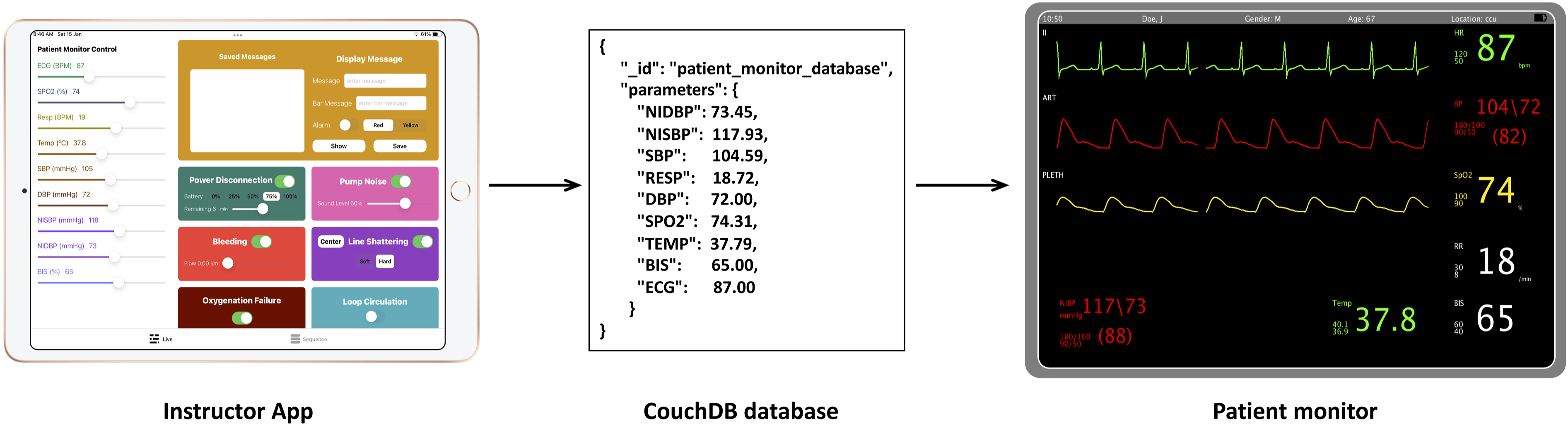
Results and discussion
In this study, we thoroughly tested each sub-system of our experimental setup individually before conducting tests at HMC. This approach allowed us to ensure that each system component functions correctly and identify potential issues before proceeding to more complex tests. Additionally, we conducted tests at HMC to assess the system’s performance under realistic operating conditions with the supervision of a senior consultant intensivist.
The study conducted at HMC was to evaluate the training program through a questionnaire. Nineteen clinicians with varying levels of experience tested the authenticity of the thermochromic ink, and the results were favorable, with participants, on average, rating the outcome as highly realistic. The average responsiveness rating of the instructor application with the simulation modules was 4.7 out of 5 (1: Not responsive at all - 5: Very responsive), while the live control panel intuitiveness scored an average of 4.8 out of 5 (1: Not intuitive at all - 5: Very intuitive). These scores demonstrate the successful precision in controlling simulation modules to generate effective physical cues and the ease of managing them through the instructor apps. More details about the HMC testing can be found in.23,25
The main focus in designing and implementing the simulator is cost efficiency, necessitating balancing equipment quality and expenses. The current cost structure for developing the simulator is categorized into mechanical components, electrical components, and 3D-printing equipment. Notably, automatic features encompass pumps, valves, and heat exchangers, while electrical components consist of microcontrollers, sensors, and amplifiers. These combined costs of the prototype amount to 4450 USD, significantly below the price of a single HLS oxygenator, which is 5500 USD. It should be emphasized that the genuine oxygenator is replaced regularly owing to contamination concerns; consequently, the ECMO simulator is substantially less expensive than a real ECMO machine.
Patient unit
Transparent acrylic sheets with an 8mm thickness were utilized in constructing the case. The sheets were cut with a laser cutter and attached with brackets and screws to guarantee effective maintenance. Figure 3 (a) displays a top view of the patient unit, with all sections labeled accordingly. To add more simulation modules to the patient unit, one only needs to connect a simulation module to the patient unit and attach control wires to the main control board. This modular setup allows instructors to add simulation modules with minimal cost and effort. Figure 3 (a) also exhibits the cooler unit responsible for cooling down the thermoelectric ink to facilitate color change when necessary. Moreover, Figure 3 (b) shows the side view of the patient unit. Figure 3 (c) illustrates the fast connect/disconnect fitting that can connect to the rest of the simulation modules found on the side of the patient unit. The patient unit’s modular enclosure has been equipped with wheels to facilitate its mobility. The primary control board was created to provide two major functions to the modules: power and connection to the local database. The primary control board is displayed in Figure 4 (a). Patient unit modular casing implementation showing the (a) top, (b) side view, and (c) quick discount segment. The modular casing showing the (a) patient unit main-board and (b) overview of an enhanced version of the heater-cooler prototype.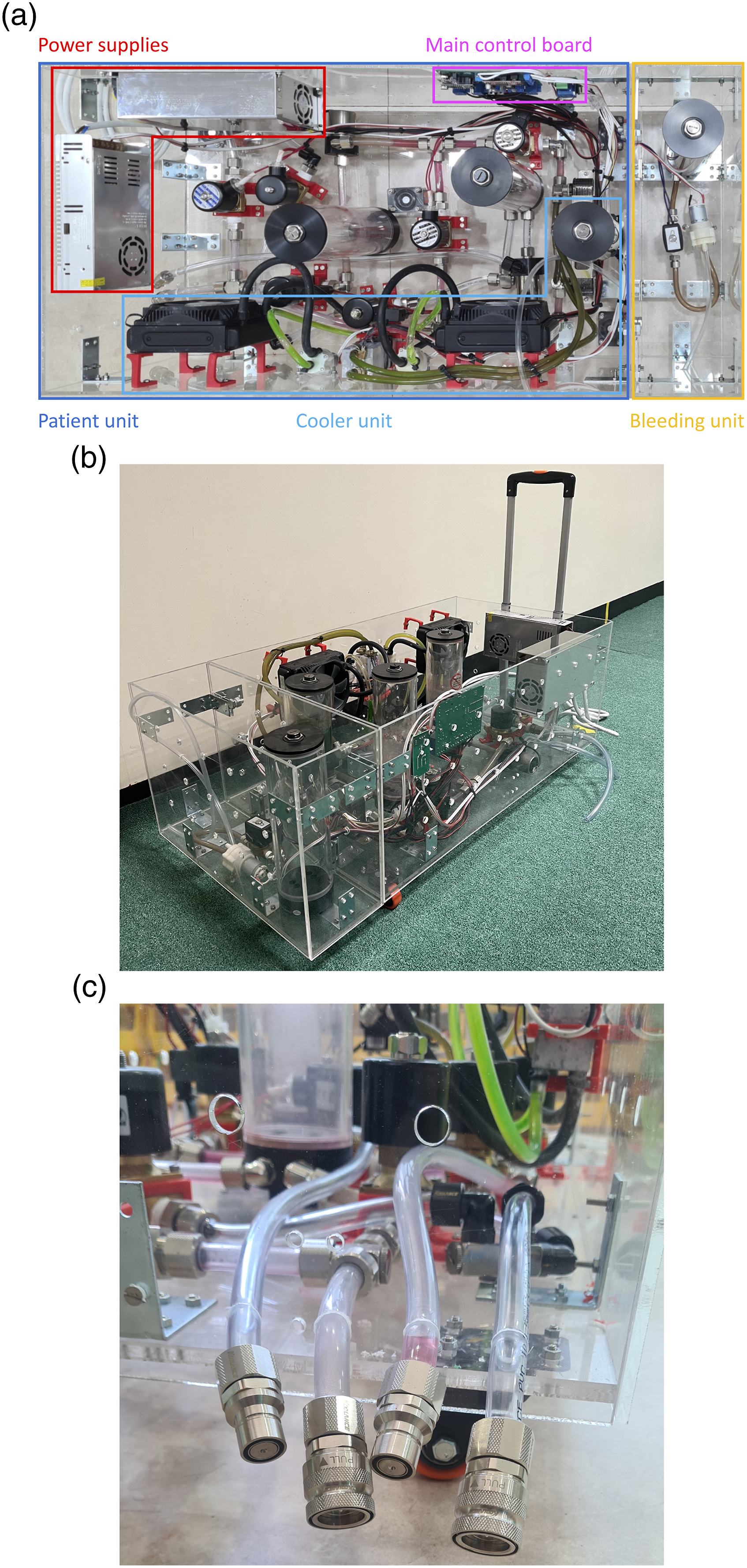

Heater-cooler unit
The tank for thermochromic ink holds bright ink while simulating. The ink will turn dark red when it enters the cooler unit. In Figure 4 (b), the ink is transferred to the heater unit to switch to bright red. The green liquid is used as a coolant by the cooler unit. Incorporating non-linear terms like flow rate and heat transfer, the bypass technique is implemented, and three valves are installed at each heat exchanger to establish a loop bypass. The bypass allows the isolation of the heater and cooler units from one another, thus reducing the impact of heat transfer on each loop. This will result in a faster response time for the prototype to change color. Additionally, a tank containing dark ink is included in the system, allowing for speedier oxygenation and de-oxygenation scenarios. Consequently, various scenarios can be obtained in a shorter time frame.
Several factors must be watched to test and verify the prototype, including the temperature of each tank, the flow rate of each pump, and the noticeable color change. Furthermore, the practical test is described as follows: • Full integration with the patient module. • Reliable wireless communication with instructor application. • Achieve the temperature change (ΔT) for the thermochromic ink within a specified time frame.
Following that, two situations for testing the prototype are defined: (1) oxygenation and (2) de-oxygenation.
Oxygenation scenario
In the process of simulating an oxygenation scenario, the dark thermochromic ink, which represents deoxygenated blood, is directed towards the heater unit. The heater unit plays a vital role in enhancing the potency of the thermochromic ink by increasing its temperature. This increased temperature amplifies the intensity of the thermochromic ink, thus making it appear brighter in color. The next step in this process is directing the deoxygenated blood, now dark-colored due to the presence of the dark thermochromic ink, towards the oxygenator. The oxygenator is responsible for saturating the blood with oxygen, transforming it into a bright color representing oxygenated blood.
In order to achieve the ideal temperature for the thermochromic ink, it may take up to 3 minutes for the temperature to reach 37°C. This time may vary depending on the specific system used and other variables that may affect the heating process. The temperature of the thermochromic ink must be carefully monitored to ensure that it does not overheat, which could lead to undesirable effects on the simulation results.
De-oxygenation scenario
The de-oxygenation situation will occur without the heater module (i.e., oxygenator). As a result, all of the pipes will acquire a deep red hue. The temperature of the thermochromic ink must be reduced to 25°C. As a result, improving the cooling unit can reduce the temperature to 25°C (i.e., from 37°C) in 4 to 6 min.
Mock oxygenator
A new version was created to resolve the leakage problem in the previous mock oxygenator design. The new design encloses small PVC tubes through which the thermochromic ink will flow inside the oxygenator rather than using 3D-printed tubes. The PVC tubes are accurately held to prevent any visible effects on the oxygenator’s realism, appearance, and feel. Furthermore, the new design uses steel screws for assembling the oxygenator instead of glue to establish internal connections, making the printed circuit board (PCB) accessible for maintenance or upgrades. The PCB is designed to be mounted inside the oxygenator to keep the LED matrix away from the thermochromic ink tubes.
The mock oxygenator must install two simulation modules to reproduce real-life situations in the ECMO training exercise. To elaborate, the oxygenator blood clotting and the oxygenator sounds are two real-world situations. • Oxygenator blood clotting: The physical effect of light can mimic blood clotting by independently manipulating the LEDs in an LED array and putting them behind a 3D-printed element. The designed PCB is executed and placed inside the oxygenator, with LEDs facing the top. A microcontroller linked remotely to the local network and the modeling system’s database controls the LED array. • Oxygenator noise: The noise from the HLS Advance 5.0 oxygenator was recorded using a high-definition recorder to replicate oxygenator noise. The captured tune was noise-filtered, enhanced with special software, and saved to a private digital SD card. The SD card is put into an MP3 device, also managed by the same microcontroller that controls the LED matrix.
Figure 5 (a) depicts the metal casing that houses the mock oxygenator and the CARDIOHELP interface display. Figure 5 (b) also depicts the mock oxygenator, version 3, during a bench test at Qatar University while linked to the modeling system. The test was performed at various loop pressures and speeds for an extended time to ensure no failures during modeling and training exercises. The test findings were promising, and the mock oxygenator effectively circumvented the loop from the patient unit to the heater unit with zero fluid loss. Implementation of the mock oxygenator showing the (a) metal case and (b) 3D-printed replica.
Simulated patient monitor
The instructor application is enhanced to provide additional functionality, which includes the ability to manage the vital signs parameters of the simulated patient monitor. To elaborate, the users can control the device’s vital signs data through the instructor application. CouchDB is the back-end database facilitating communication between the instructor application and the patient monitor. Utilizing this database allows the instructor application to retrieve and send data to the patient monitor in real time, allowing for seamless device management, shown in Figure 2. In summary, the instructor application has been upgraded to enable users to control the vital signs parameters of the simulated patient monitor, with CouchDB acting as the communication medium between the two devices.
To provide more details about the design, the frequency at which the graphs are displayed is controlled by the heart rate data collected over a 6-s interval. This information is then used to display the waveform, as shown in Figure 6. The simulated monitor can also produce audio sounds to indicate the average heart rate range or any emergency situation when the heart rate is below or above the normal range. This design comprehensively monitors a patient’s vital signs, with visual and audio cues to help medical professionals promptly detect and respond to potential issues. A senior consultant intensivist thoroughly oversaw the simulated patient’s tests. The frequency change of the waveforms depends on the heart rate with (a) 120 HR and (b) 70 HR.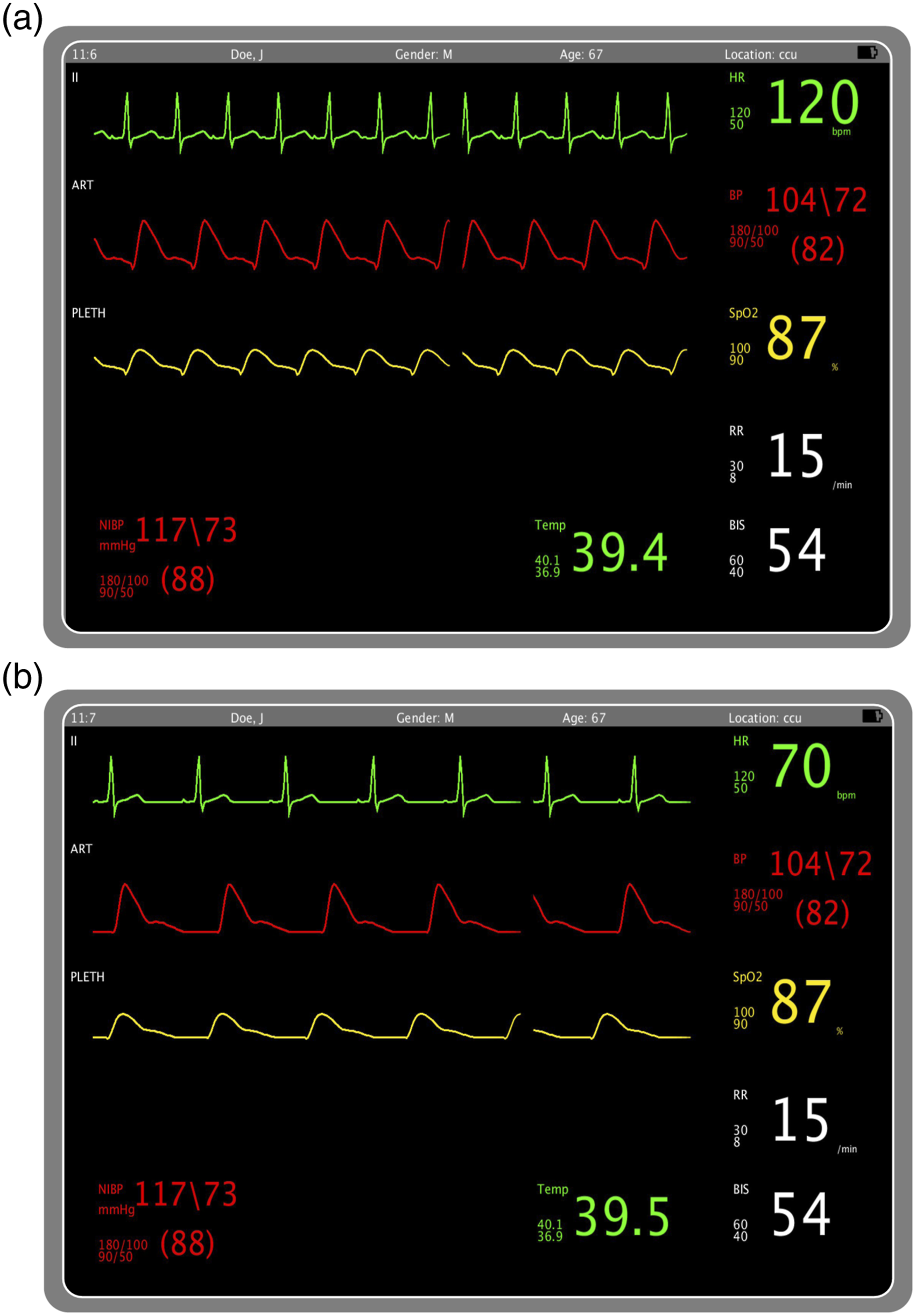
Future directions
When considering the implementation of devices like the ambulatory ECMO simulator in a clinical setting, there may be limitations that should be addressed in future work. Some prominent concerns include the limited availability of space for conducting training sessions, making it challenging to perform comprehensive simulations within a healthcare facility’s busy and restricted environment. Additionally, the availability of personnel to actively participate in these training sessions is a significant consideration, as medical professionals often have demanding schedules, making coordination difficult. Given these significant considerations, there is a greater need to address the challenges associated with implementing the ambulatory ECMO simulator in clinical settings.
Conclusion
In conclusion, current medical simulators for ECMO are limited by high costs and low-fidelity methodologies. A new approach is required to overcome this challenge and integrate with critical care environments, particularly in the aftermath of the COVID-19 pandemic, where resources and supplies are scarce. This study planned to advance the cutting edge of ECMO simulation and establish criteria for a cost-effective, high-realism ambulatory ECMO simulator. The research team spent 3 years gathering data, reviewing the literature, and continuously developing the prototype of the system modules and the accompanying tablet application. As a result, they successfully addressed the issues of cost and fidelity in ECMO simulation, offering a practical tool for medical professionals to enhance their knowledge and support of patients requiring ECMO therapy. This paper presents a comprehensive ambulatory ECMO simulator, detailing the modular casing of the physical components and the simulated patient monitor’s many sub-systems.
Future work entails designing a cannulation system to provide a high-fidelity human circulatory emulator to supplement the ECMO machine model and instructor application. To incorporate the cannulation simulator into the instructor application, all sensor data must be sent to the application to allow the instructor to remotely monitor the learners’ progress and be able to simulate multiple procedural emergencies, including seizures, heart attacks, and lung failures.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was supported by the Qatar University Internal Grant No. M-CTP-CENG-2020-1.