
Abstract
Introduction
Acute peripheral and coronary artery embolism are common complications of diabetes mellitus and greatly affect the clinical outcome of patients with diabetes; however, there are few reports about the symptoms and prognosis of patients with acute myocardial infarction (AMI) and concurrent acute lower extremity arterial embolism (ALEAE).
Case presentation
A 44-year-old man with a history of 4 years of type 1 diabetes was admitted to hospital after suddenly experiencing severe pain in his right lower limb and feeling tightness in the left anterior chest area. Ultrasonography revealed distal occlusion of the right superficial femoral artery, and an electrocardiogram showed acute anterior interstitial myocardial infarction. After conservative treatment for 2 days, the patient had severe necrosis of the lower limbs and secondary injury of multiple organs. Haemodialysis and heparin anticoagulant therapy were performed before amputation. Twelve days after the operation, the patient's condition was stable, and he was transferred out of the intensive care unit.
Conclusions
If patients with ALEAE miss the opportunity for early treatment, even with AMI, emergency amputation under general anaesthesia is the right strategy to save lives.
Keywords
Introduction
The most devastating complications of diabetes mellitus (DM) are microvascular and macrovascular lesions that clinically encompass cardiovascular disease (CVD), retinopathy, nephropathy and neuropathy. 1 Peripheral and coronary artery embolism (CE) disease frequently manifests in individuals with diabetes. 2 Revascularisation or thrombectomy procedures performed at the embolised site can potentially lead to distal embolisation. However, spontaneous co-occurrence of acute myocardial infarction (AMI) and acute lower extremity arterial embolism (ALEAE) has been reported only rarely. This study presents a case of a patient with AMI and ALEAE who underwent amputation under general anaesthesia.
Case presentation
Preoperative and postoperative laboratory tests.
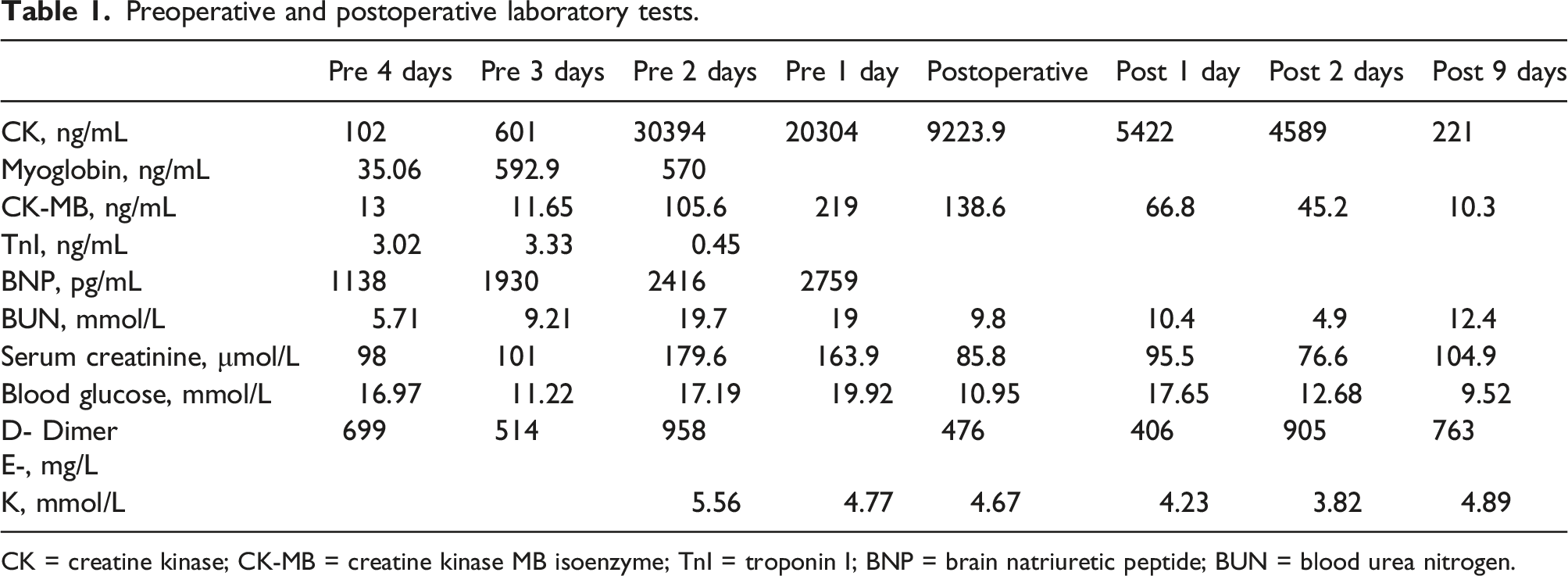
CK = creatine kinase; CK-MB = creatine kinase MB isoenzyme; TnI = troponin I; BNP = brain natriuretic peptide; BUN = blood urea nitrogen.
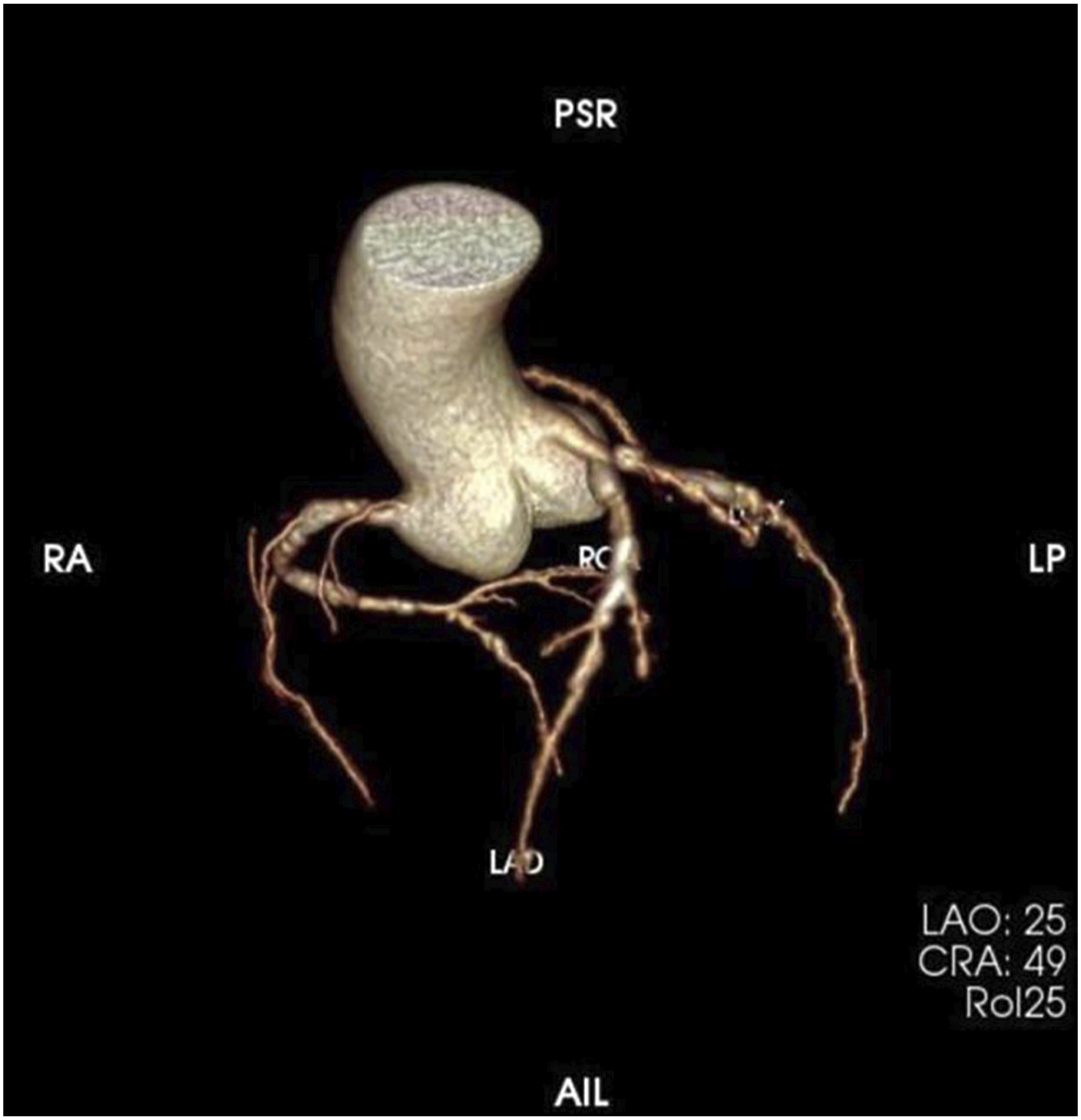
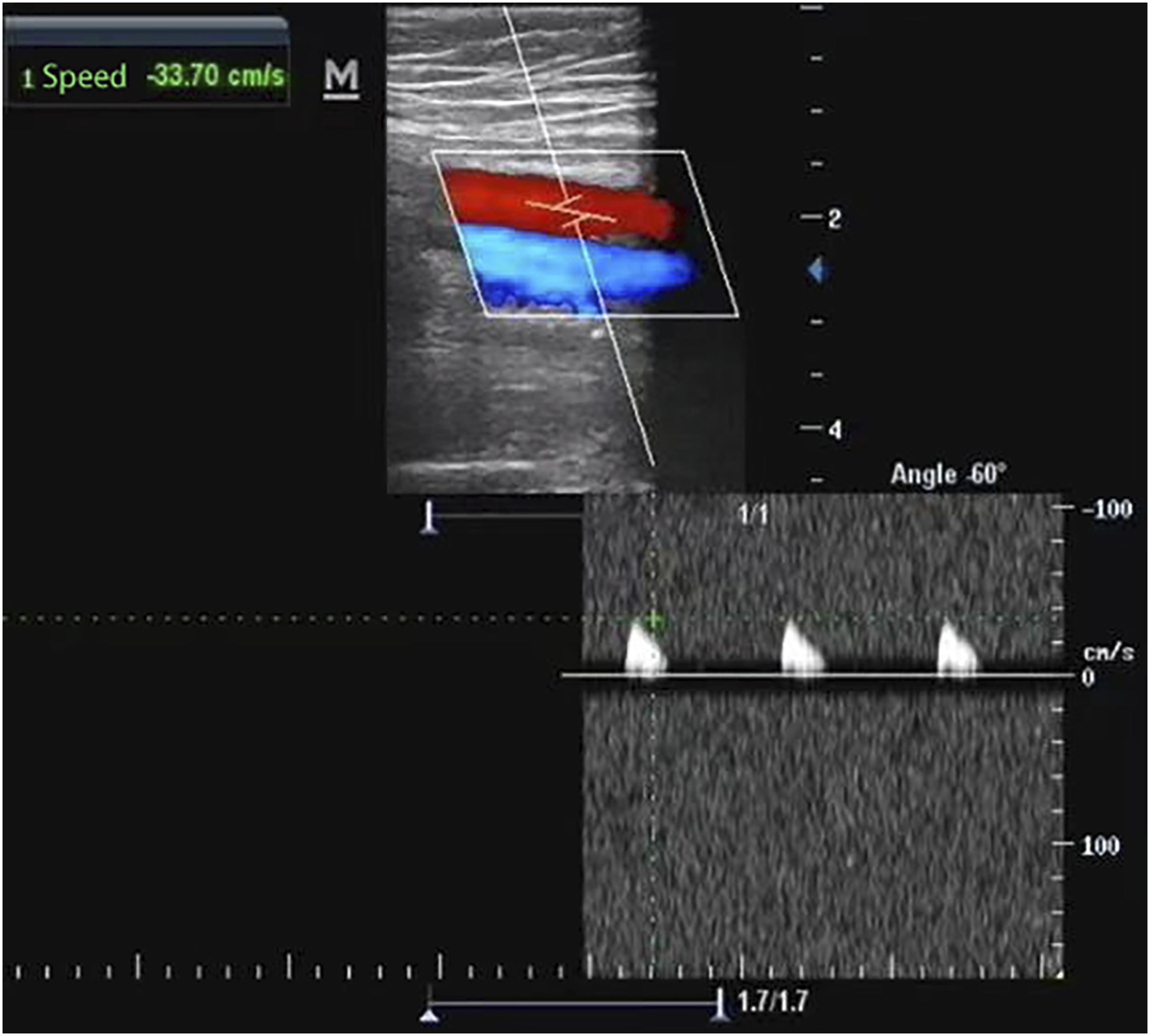
The patient was immediately transferred to the authors’ hospital for further treatment. A chest computed tomography (CT) scan showed suspicious infection of both lungs, interstitial lesions and bilateral pleural effusion. An ECG showed acute anterior interstitial myocardial infarction (Figure 1). The level of serum creatine kinase elevated to 30,394 U/L, and CRE increased to 177.4 μmol/L. The CT angiography showed that there were significant stenoses located at the left anterior descending artery and left circumflex artery (Figure 2). The skin colour of the anterior tibia of the patient's right leg was significantly darker than that of the contralateral limb, accompanied by severe pain and the disappearance of pulsation of the dorsal foot artery (Figure 3). The lower limb vascular ultrasound of the patient's right leg revealed an embolism in the middle segment of the right superficial femoral artery, characterised by diminished blood flow velocity in the right common femoral artery. Additionally, there was a complete absence of detectable flow in both the right anterior and posterior tibial arteries, as well as in any of the crural arteries (Figure 4). The affected lower extremities exhibited severe skeletal muscle necrosis. ECG manifestation showing the acute anterior interstitial myocardial infarction. Preoperative coronary computed tomography angiography. The angiography showed that there were significant stenoses in the left anterior descending artery and left circumflex artery. Lower extremity and amputation with arterial embolism. Lower extremity vascular ultrasound shows blood stream state.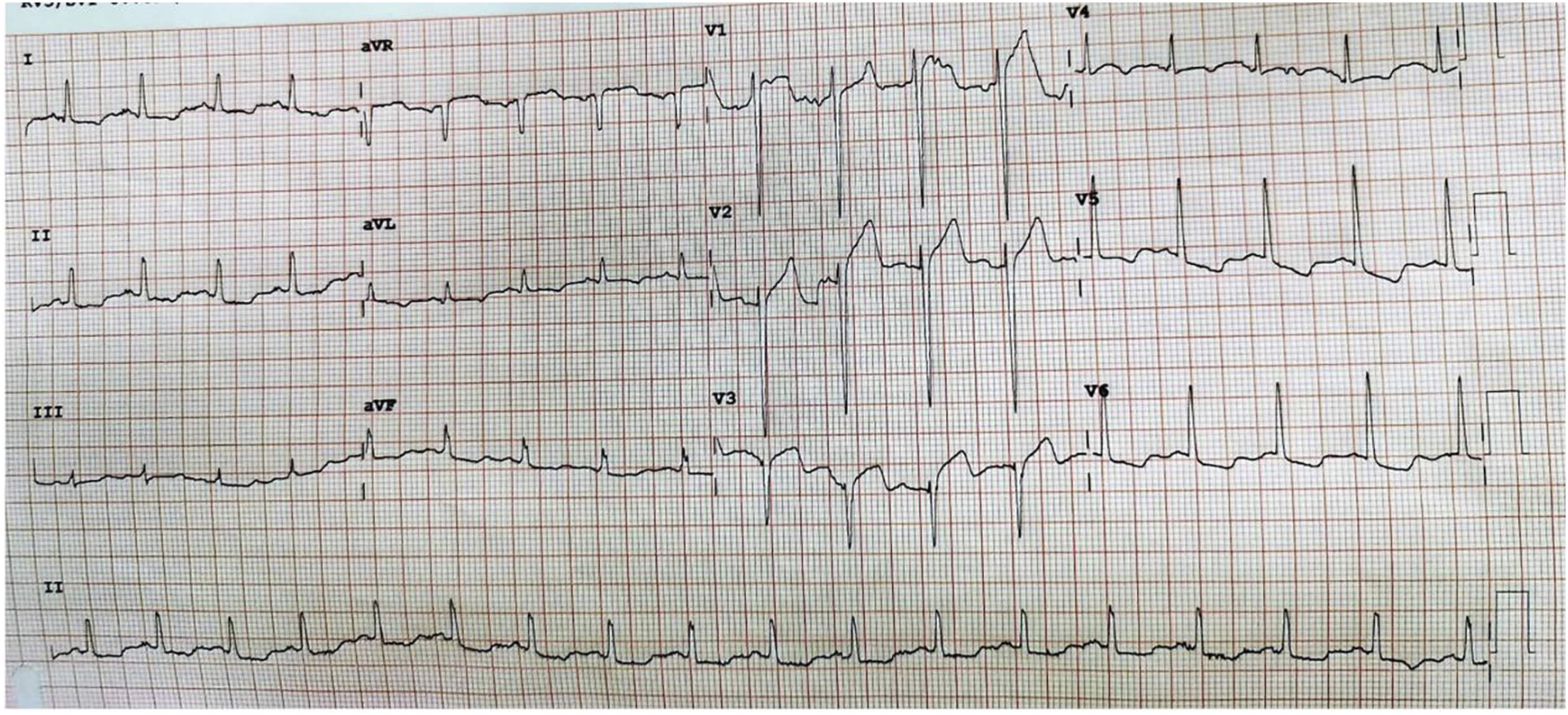

Following a thorough multidisciplinary consultation, the cardiologist initiated coronary vasodilatation and anticoagulation medications, and it was unanimously decided that immediate measures encompassing haemofiltration and heparin anticoagulant therapy should be undertaken. Given the prolonged ischemia period, which exceeded 6–8 hours and resulted in an insensate and immobile limb, the prospects for limb salvage were deemed improbable. Consequently, an urgent amputation of the right lower limb was judged to be the primary course of action for this patient.
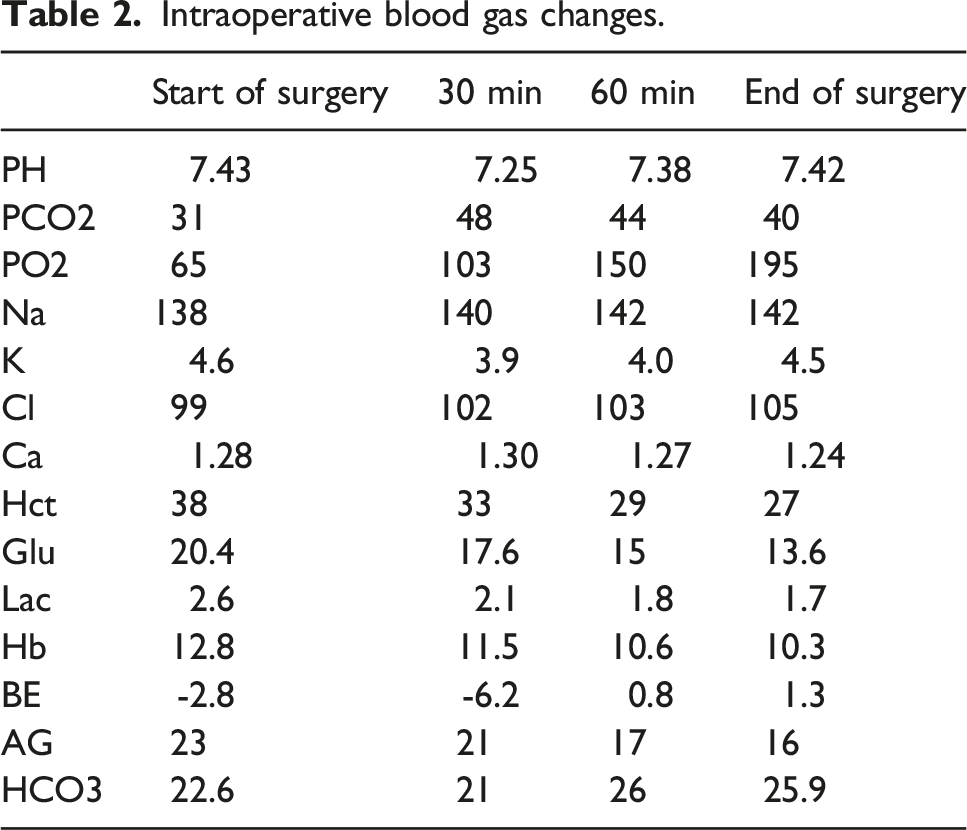
Intraoperative blood gas changes.
The surgical procedure was right superior knee amputation. Anterior and posterior tongue flaps were designed along the amputation plane of 10 cm above the knee on the right side. The length of the flaps was approximately 1/2 of the thigh diameter. The amputation position was 10 cm above the knee. The thrombus was found in the superficial femoral artery of the severed limb, which was consistent with the results of the preoperative examination. No residual thrombus was detected in the proximal arteries and veins of the right lower extremity. After amputation, the bleeding was stopped completely, and the wound was rinsed repeatedly with hydrogen peroxide and saline. Bone residues were covered with periosteum suture, muscle, subcutaneous tissue and skin were sutured at one time, drainage tubes were placed in the wound and VSD was used to cover the wound.
The OI of the patient dropped to 150 during the amputation. Methylprednisolone 0.5 g and dexamethasone 10 mg were administered. Blood gas analysis during amputation showed a pH of 7.25, BE -6.2, and 150 mL of 5% sodium bicarbonate was given intravenously. The blood potassium was maintained for 4.0 L by intravenous infusion of 15% potassium chloride 1.5 g. The patient's OI returned to 210 and remained at that level until the end of the amputation.
The intubated patient was then transferred to the intensive care unit (ICU). Persistent low OI necessitated an extended period of endotracheal intubation, which persisted until the third day postoperatively; this led to the removal of the endotracheal tube from the patient 3 days after the surgery. The creatine kinase of the patient dropped to 5,422 U/L on the first day after surgery and returned to normal on the ninth day after the operation. A colour Doppler ultrasound scan 1 day after the operation confirmed there was no thrombus in the left and right lower legs. On re-examination 3 days after the operation, the results of colour Doppler ultrasound with an ejection fraction of 47% clearly demonstrated that the heart function had improved. The patient received a diagnosis of acute kidney injury, evidenced by a reduction in urine output (<0.5 mL/kg per hour), a condition that persisted for approximately 9 days post-surgery. Haemofiltration was performed to manage fluid balance and facilitate the elimination of toxins from the system until renal function was restored to baseline levels. Twelve days after the operation, the patient's condition was stable and he was transferred from the ICU to the general ward of the cardiology department for further treatment. After the operation, the patient underwent a coronary CT examination following the improvement of lower limb conditions. It was found that the left anterior descending artery had moderately severe stenosis, and the middle and distal segment of the left circumflex artery had severe stenosis. The first obtuse marginal branch and the middle segment of the right coronary artery were severely narrowed. The patient refused to undergo coronary angiography after surgery and was discharged after the symptoms were relieved. During the follow-up after the surgical procedure, the patient underwent regular anticoagulation, lipid-lowering and control of blood glucose and did not present any cardiovascular or cerebrovascular adverse events. Finally, the patient was able to perform normal activities.
Discussion
The risks of cardiovascular and lower limb arterial disease are not uncommon in diabetics. Both DM and other disorders of glucose metabolism are risk factors for CVD. More than half the mortality and a very high level of morbidity in people with DM are related to CVD. 2 The causes of myocardial infarction in diabetic patients may be multifactorial. Coronary artery embolism, in which obstructive material enters the coronary artery, blocks its blood flow and causes ischemia, is an uncommon cause of AMI. Patients with CE represent a high-risk subgroup of patients with AMI. 3 The shedding of cardiogenic embolus can theoretically lead to embolisation of lower extremity arteries, but spontaneous co-occurrence of acute embolisation of the coronary arteries and the great arteries of the lower limbs is very rare.
Previous studies have reported that atrial fibrillation (AF) is the most frequent cause of CE. 4 Diabetes mellitus is frequent in patients with AF; community studies have demonstrated the presence of DM in 13% of patients with AF. 3 The patient in this case did not have AF. In the follow-up of his medical history, it was found that the patient – who was diagnosed with type 1 diabetes – did not control or monitor his blood glucose in any way. Due to the difficulty in using insulin to control blood glucose during hospitalisation, the authors suspected that the patient's blood glucose level before admission was not well controlled. Therefore, he was at high risk of developing CVD due to long-term hyperglycaemia. The authors speculated that the most likely cause of AMI in this patient was the shedding of an embolus in the coronary artery or changes in coronary blood flow under a state of stress after lower limb artery occlusion.
In addition to CVD, DM is also considered an established risk factor for cerebrovascular and peripheral vascular diseases including stroke and peripheral artery disease (PAD). 5 A proinflammatory state in patients with diabetes was considered a possible reason for increased levels of some clotting factors and impairment of the fibrinolytic system leading to a hypercoagulable state. However, the association between DM and venous thromboembolism (VTE) is not confirmed by studies.5,6 A recent study reported that type 1 DM appeared to be an independent risk factor for VTE development. 7 The clinical characteristics of arterial and venous embolic diseases are different, and the symptoms and signs of PAD are variable. Arterial ischemia is often characterised by low skin temperature, pain or intermittent claudication. However, studies have demonstrated that the majority of patients with confirmed PAD do not have typical claudication. 8 Acute limb ischemia (ALI) is one of the most treatable and potentially devastating presentations of PAD. This present case patient presented with an acute embolism of the lower extremity arteries without any other PAD-related symptoms before admission. Long-term abnormal blood glucose levels in this patient may be a potential cause of lower extremity arterial disease (LEAD).
Lower extremity arterial disease is particularly frequent in patients with DM with worse outcomes, especially the risk of lower limb amputation, compared with non-diabetic patients.9–11 The pathogenesis of LEAD in individuals with diabetes includes endothelial dysfunction and increased arterial wall stiffness, which may promote the process of atherosclerosis.12,13 Treatment strategies for LEAD patients include drug therapy and surgical or endovascular revascularisation. However, in patients with ALEAE, the earlier the embolus is removed, the better the chance of preserving the lower extremity function. According to the guidelines, if expertise in treatment for acute ischemia is not locally or rapidly available, there should be strong consideration of transferring the patient to a facility with such resources. 14
Lower extremity symptoms in ALI can include both pain and loss of function. The longer these symptoms are present, the less likely the possibility of limb salvage.15,16 The duration of skeletal muscle tolerance to ischemia is approximately 4–6 hours 17 In this present case, the patient underwent amputation under general anaesthesia during the stage of AMI. Non-cardiac surgery during AMI is undoubtedly a great challenge, but preoperative multidisciplinary consultation provided adequate treatment preparation for the patient. Glucocorticoids were used intraoperatively to prevent the release of ischemic metabolites that may cause multiple organ failure. Intraoperative protective lung ventilation strategies also improved the patient’s OI.
The impact of regional or general anaesthesia on the clinical outcomes of patients undergoing major lower extremity amputation is still controversial. Some studies have revealed that regional anaesthesia can decrease the incidence of postoperative pulmonary complications and cardiac arrhythmias18–21 and reduce the need for perioperative blood transfusions. 22 However, regional anaesthesia does not offer a mortality advantage over general anaesthesia.22,23 Therefore, although studies have reported that regional anaesthesia alone may be safer for amputations in critically ill patients, the authors consider that stress response under regional anaesthesia may increase the risk of cardiac ischemia. Preoperative continuous heparin anticoagulation therapy is also contraindicated for most deep nerve block anaesthesia. Appropriate haemodynamic support and ventilation strategies under general anaesthesia may reduce organ response to tissue necrosis metabolites. This case also provides some experience for patients who need urgent surgery during AMI with haemodynamic instability.
Conclusion
Simultaneous spontaneous occurrence of AMI and ALEAE is very rare. Effective treatment for early acute arterial ischemia is important. If patients with ALEAE miss the opportunity for early treatment, even with AMI, emergency amputation under general anaesthesia is the right strategy to save lives.
Footnotes
Author contributions
Conception and design of the work: Lin YJ; Data collection: Xue YY, Han YL, Bao TX, Xue J, Lu LY; Supervision: Lin YJ; Analysis and interpretation of the data: Lin YJ, Xue YY, Han YL, Bao TX, Xue J, Lu LY; Statistical analysis: Lin YJ, Lu LY; Drafting the manuscript: Lin YJ; Critical revision of the manuscript: all authors; Approval of the final manuscript: all authors.
Ethical statement
Data Availability Statement
All relevant data are within the manuscript and its additional files.