
Abstract
Introduction
In children with myocarditis or dilated cardiomyopathy (DCM) on extracorporeal membrane oxygenation (ECMO) for cardiogenic shock, it is often necessary to decompress the left heart to minimize distension and promote myocardial recovery. We compare outcomes in those who underwent balloon atrial septostomy (BAS) versus direct left atrial (LA) drainage for left heart decompression in this population.
Methods
Retrospective study of the Extracorporeal Life Support Organization (ELSO) multicenter registry of patients ≤ 18 years with myocarditis or DCM on ECMO who underwent LA decompression. Descriptive and univariate statistics assessed association of patient factors with decompression type. Multivariable logistic regression sought independent associations with outcomes.
Results
369 pediatric ECMO runs were identified. 52% myocarditis, 48% DCM, overall survival 74%. 65% underwent BAS and 35% LA drainage. Patient demographics including age, weight, gender, race/ethnicity, diagnosis, pre-ECMO pH, mean airway pressure, and arrest status were similar. 89% in the BAS group were peripherally cannulated onto ECMO, versus 3% in the LA drainage group (p < .001). On multivariable analysis, LA drainage (OR 3.96; 95% CI, 1.47-10.711; p = .007), renal complication (OR 2.37; 95% CI, 1.41-4.01; p = .001), cardiac complication (OR 3.14; 95% CI, 1.70-5.82; p < .001), and non-white race/ethnicity (OR 1.75; 95% CI, 1.04-2.94; p = .035) were associated with greater odds of mortality. There was a trend toward more episodes of pulmonary hemorrhage in BAS (n = 17) versus LA drainage group (n = 3), p = .08. Comparing only those with central cannulation, LA drainage group was more likely to be discontinued from ECMO due to recovery (72%) versus the BAS group (48%), p = .032.
Conclusions
In children with myocarditis or DCM, there was a three times greater likelihood for mortality with LA drainage versus BAS for LA decompression. When adjusted for central cannulation groups only, there was better recovery in the LA drainage group and no difference in mortality. Further prospective evaluation is warranted.
Keywords
Background
In children who are placed on extracorporeal membrane oxygenation (ECMO) for cardiogenic shock in the setting of myocarditis or dilated cardiomyopathy (DCM), it is often necessary to decompress the left heart in order to minimize distension and promote myocardial recovery. 1 In addition, left atrial decompression protects from lung injury secondary to cardiogenic pulmonary edema and pulmonary hemorrhage. 2 Previous studies have demonstrated improved survival in those who have undergone left atrial decompression compared to those who have not. 1 Additionally, early left atrial decompression has been associated with improved survival and shorter duration of mechanical ventilation when compared to delayed intervention. 3
There are various methods of performing left atrial decompression, and no standard practice across institutions. Balloon atrial septostomy (BAS) permits left to right shunting and was among the first invasive strategies used to decompress the left ventricle during ECMO. 4 Left atrial (LA) drainage, either by direct placement of a left atrial cannula or percutaneous technique, allows blood to be actively pumped from the left atrium to the arterial system by the ECMO circuit, which may more effectively decompress the left atrium and maintain systemic arterial pressure. 4 A single institution study has previously demonstrated no difference between decompression technique and outcomes. 5 However, to our knowledge, the association between method of left atrial decompression and outcomes has not been evaluated in a multi-institutional study. Thus, we sought to compare the association of balloon atrial septostomy vs left atrial drainage with survival in children with DCM and myocarditis requiring VA-ECMO.
Methods
The primary aims of the study were to compare hospital outcomes (including ECMO decannulation) and hospital survival between the BAS and LA drainage groups. Secondary analyses were aimed at identifying predictors of successful ECMO decannulation and hospital survival. This analysis incorporated multi-institutional data. All program names and locations were completely de-identified for analysis and publication. Data were obtained retrospectively from the Extracorporeal Life Support Organization (ELSO) registry. Studies utilizing the ELSO database are exempt from local Institutional Review Board approval as the data are de-identified.
All patients less than or equal to 18 years old receiving ECMO support from January 1, 2000-December 31, 2021 with a diagnosis of myocarditis or dilated cardiomyopathy were included and identified using the following ICD-9 codes: 422 (acute myocarditis), 422.0 (acute myocarditis in diseases classified elsewhere), 422.9 (other and unspecified myocarditis), 422.90 (acute myocarditis unspecified), 422.91 (idiopathic myocarditis), 422.92 (septic myocarditis), 425, 425.7, 425.8, 425.9 (DCM), and 429 (myocarditis unspecified); or the following ICD-10 codes: I41 (Myocarditis in diseases classified elsewhere), I40.9 (Acute myocarditis, unspecified), I40.0 (Infective Myocarditis), I40.1 (Isolated Myocarditis), I51.4 (Myocarditis, unspecified), I42.0 (Dilated cardiomyopathy), I43 (Cardiomyopathy in diseases classified elsewhere), I42.7 (Cardiomyopathy due to drug and external agent), B33.24 (Viral cardiomyopathy). Patients with left heart decompression via atrial septostomy were identified using Common Procedural Technology (CPT) code 92,992 (BAS) or 33,735 (open atrial septostomy), and those with left atrial drainage were identified by reviewing their cannulation strategy. Patients with an Impella® device (Abiomed, Danvers, Massachusetts) in place as a method of LA decompression were identified using CPT code 33,990.
Predictor and outcome measurements
Patient demographic information was also collected. This included age, weight, gender, race/ethnicity, primary diagnosis, whether they were receiving extracorporeal cardiopulmonary resuscitation (E-CPR), pre-ECMO blood gases, year of cannulation to determine era effect, program volume, duration of ECMO, and ECMO complications/outcome. ECMO complications included cardiac (arrhythmia, CPR); neurologic (CNS infarction, CNS diffuse ischemia, brain death, seizures (clinically determined or by EEG), intra/extra parenchymal hemorrhage); renal (creatinine 1.5-3, creatinine >3, renal replacement therapy); metabolic (severe hemolysis, hyperbilirubinemia); mechanical (thrombosis/clot (circuit component), oxygenator failure, pump failure, air in circuit, circuit change, cannula problems, other tubing rupture); and bleeding (cannula site bleeding, gastrointestinal hemorrhage, pulmonary hemorrhage, cardiac tamponade).
Outcomes were defined based on the ELSO registry data definitions. Reason for discontinuation was classified as either (1) Expected recovery: ECLS discontinued because patient improved and is expected to recover, (2) Death/Poor Prognosis: ECLS discontinued due to poor prognosis or treatment limitations because the medical team anticipated that the patient had irrecoverable disease; or patient experienced organ failure; or a diagnosis that was incompatible with life; or family/patient perceived poor prognosis or undue suffering and requested discontinuation (3) Ventricular assist device/Transplant.
In our final analysis, we included patients with an Impella® in place in the LA drainage group, as both methods utilize “active” decompression. We excluded those with an ECMO indication other than cardiac failure (i.e. pulmonary indication or E-CPR).
Statistical analysis
Both univariate comparative and multivariate predictive analyses were performed. First, comparative statistics were used to characterize the demographics and clinical characteristics of the balloon atrial septostomy and left atrial drainage groups. Numeric variables were compared using Mood’s median test and/or paired t test was used to compare continuous variables, depending upon normality as determined using the Shapiro-Wilk test. Discrete variables were compared using chi squared and/or Fisher’s exact test were performed for categorical variables.
We assumed that within subject correlation in the pre and post assessments were least rho = 0.5 and that the intraclass correlation for patients nested within centers did not exceed rho = 0.05. Inter-institutional analyses of the primary and secondary aims were performed by grouping programs by ECMO volume. Programs were be categorized as low-, medium-, or high-volume ECMO centers, corresponding to the first quartile, interquartile range, and upper quartile of total ECMO runs performed during the study period.
As above, multivariate analyses were also performed. Analyses employed binary logistic regression to determine predictors for the endpoints of (a) successful ECMO decannulation and (b) survival to hospital discharge (using two separate analyses). Variables used in univariate analysis included demographics (age, gender, race/ethnicity), clinical characteristics (those achieving statistical significance upon comparative analyses), program ECMO volume quartile, ECMO era (2000-2007, 2008-2015, 2016-2021), ECMO cannulation strategy, and time to decompression when available, based on medians. Collinearity between variables were determined on a case-by-case basis. Factors with a p-value of < 0.2 on univariate analysis were employed as covariates on multivariate analyses. We also performed a “post hoc” analysis for all other variables between patients in the earlier era (with no time to decompression data) and the later era (patients with time to decompression data), to assess for era effect.
Results
Demographics and patient characteristics. Values reported as median (IQR) or n (%) as appropriate. BAS, balloon atrial septostomy, MAP, mean airway pressure (mmHg).
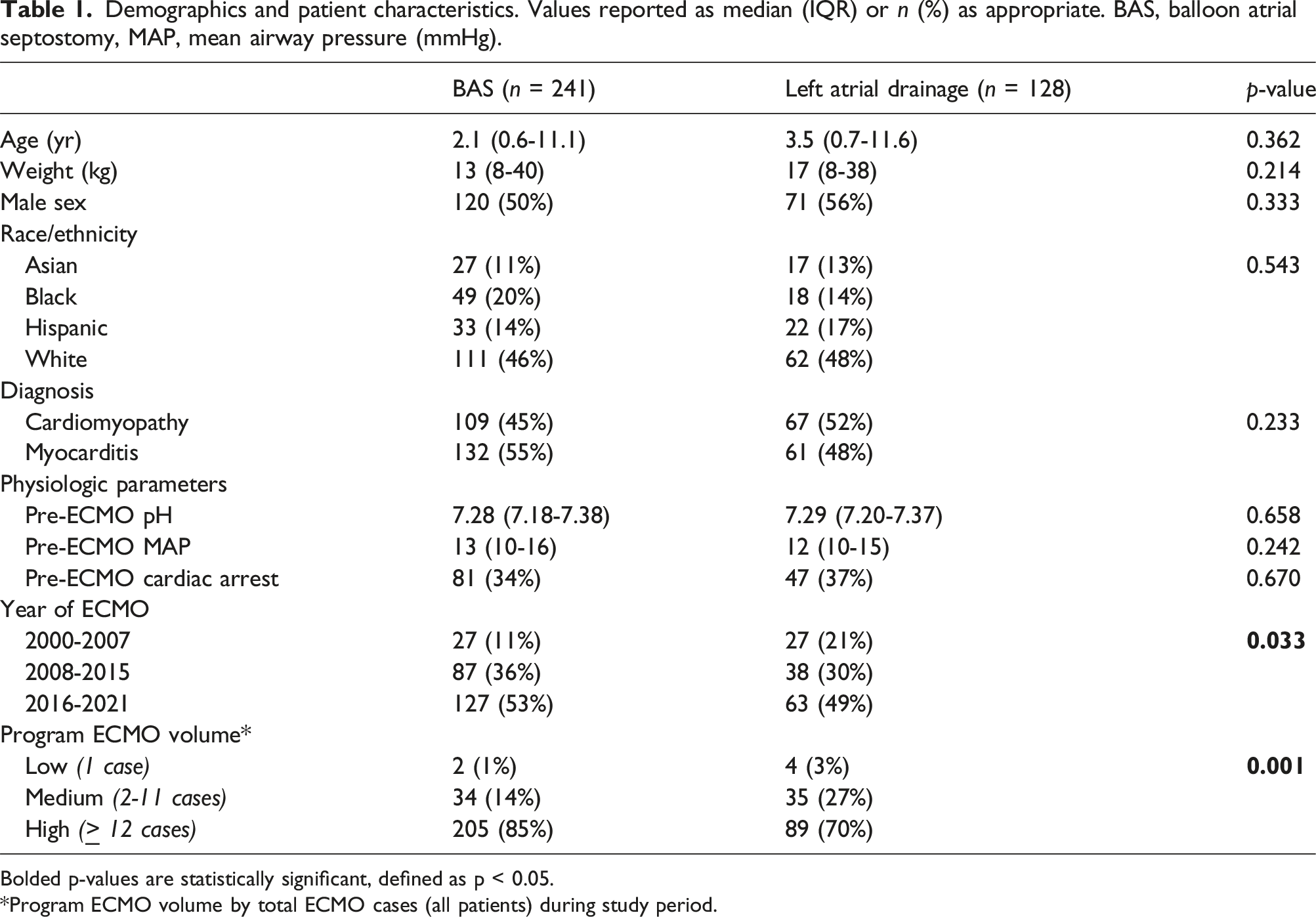
Bolded p-values are statistically significant, defined as p < 0.05.
*Program ECMO volume by total ECMO cases (all patients) during study period.
Details of ECMO run. Values reported as median (IQR) or n (%) as appropriate. ECPR, extracorporeal cardiopulmonary resuscitation; mean AP, mean airway pressure (mmHg).
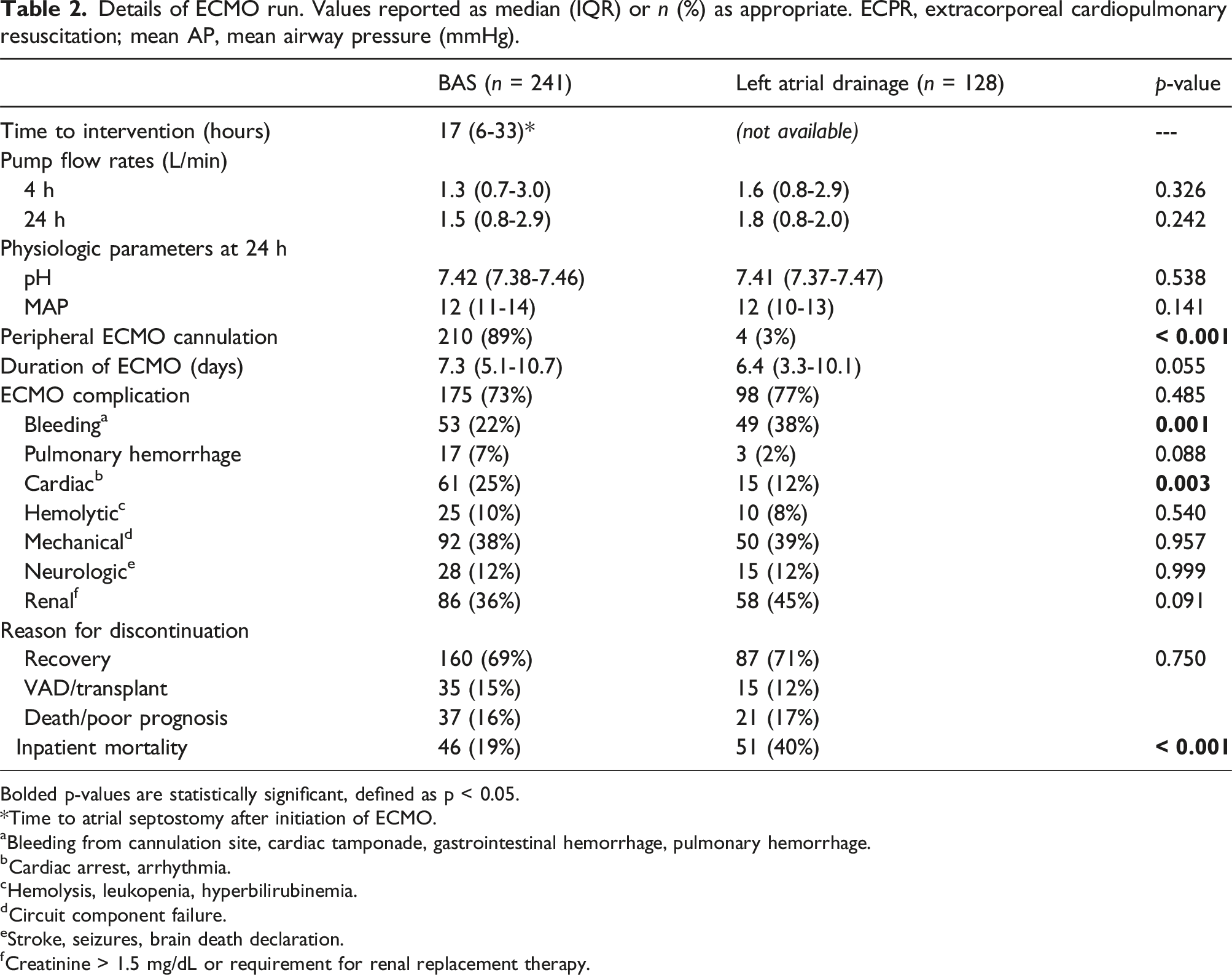
Bolded p-values are statistically significant, defined as p < 0.05.
*Time to atrial septostomy after initiation of ECMO.
aBleeding from cannulation site, cardiac tamponade, gastrointestinal hemorrhage, pulmonary hemorrhage.
bCardiac arrest, arrhythmia.
cHemolysis, leukopenia, hyperbilirubinemia.
dCircuit component failure.
eStroke, seizures, brain death declaration.
fCreatinine > 1.5 mg/dL or requirement for renal replacement therapy.
Multivariable binary logistic regression model for odds of inpatient mortality among extracorporeal membrane oxygenation (ECMO) patients. Odds ratio (OR) > 1.0 indicates positive association with inpatient mortality.
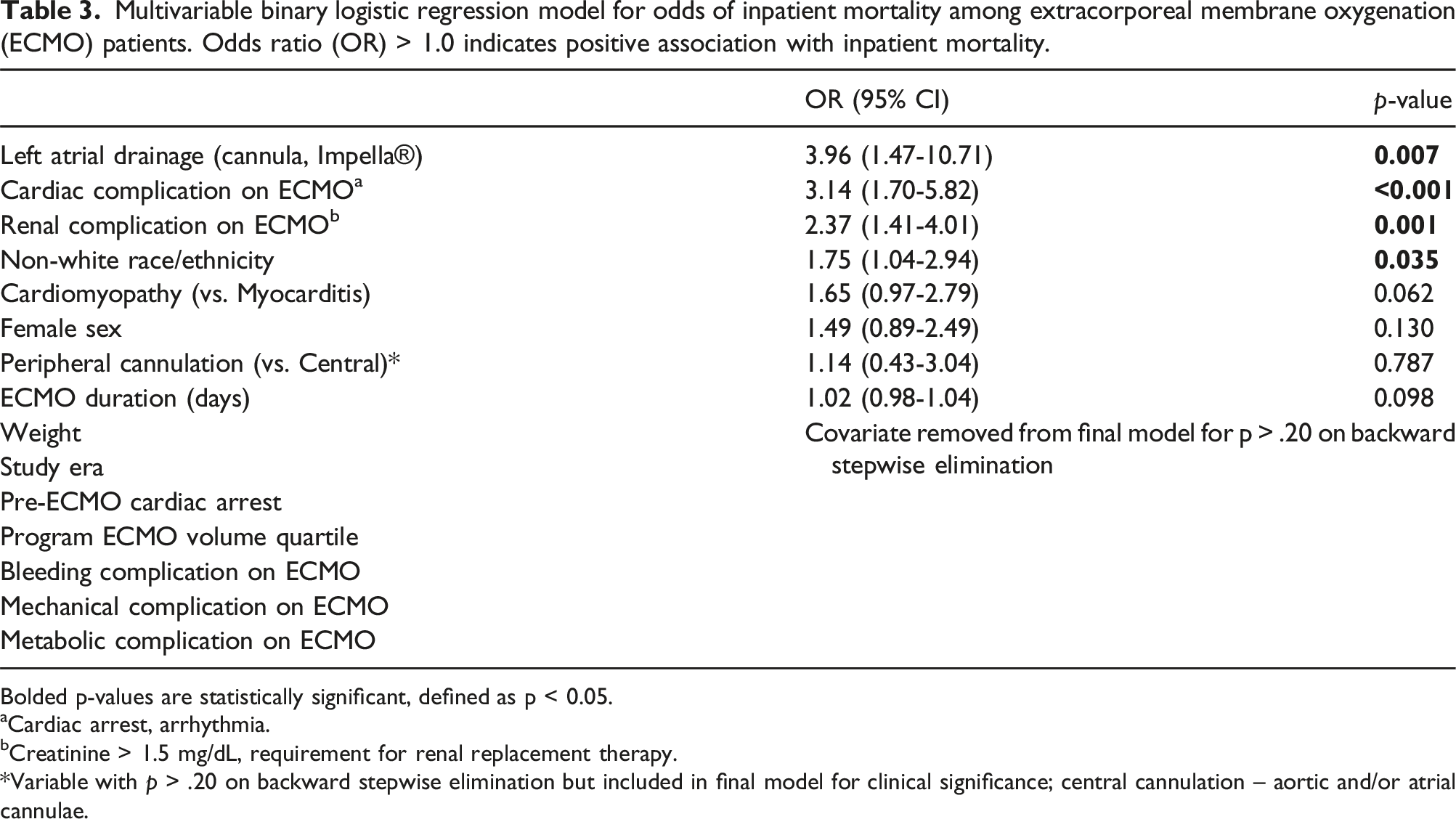
Bolded p-values are statistically significant, defined as p < 0.05.
aCardiac arrest, arrhythmia.
bCreatinine > 1.5 mg/dL, requirement for renal replacement therapy.
*Variable with p > .20 on backward stepwise elimination but included in final model for clinical significance; central cannulation – aortic and/or atrial cannulae.
Demographics, patient characteristics, and details of ECMO run for central cannulation only. Values reported as median (IQR) or n (%) as appropriate. mean AP, mean airway pressure (mmHg).
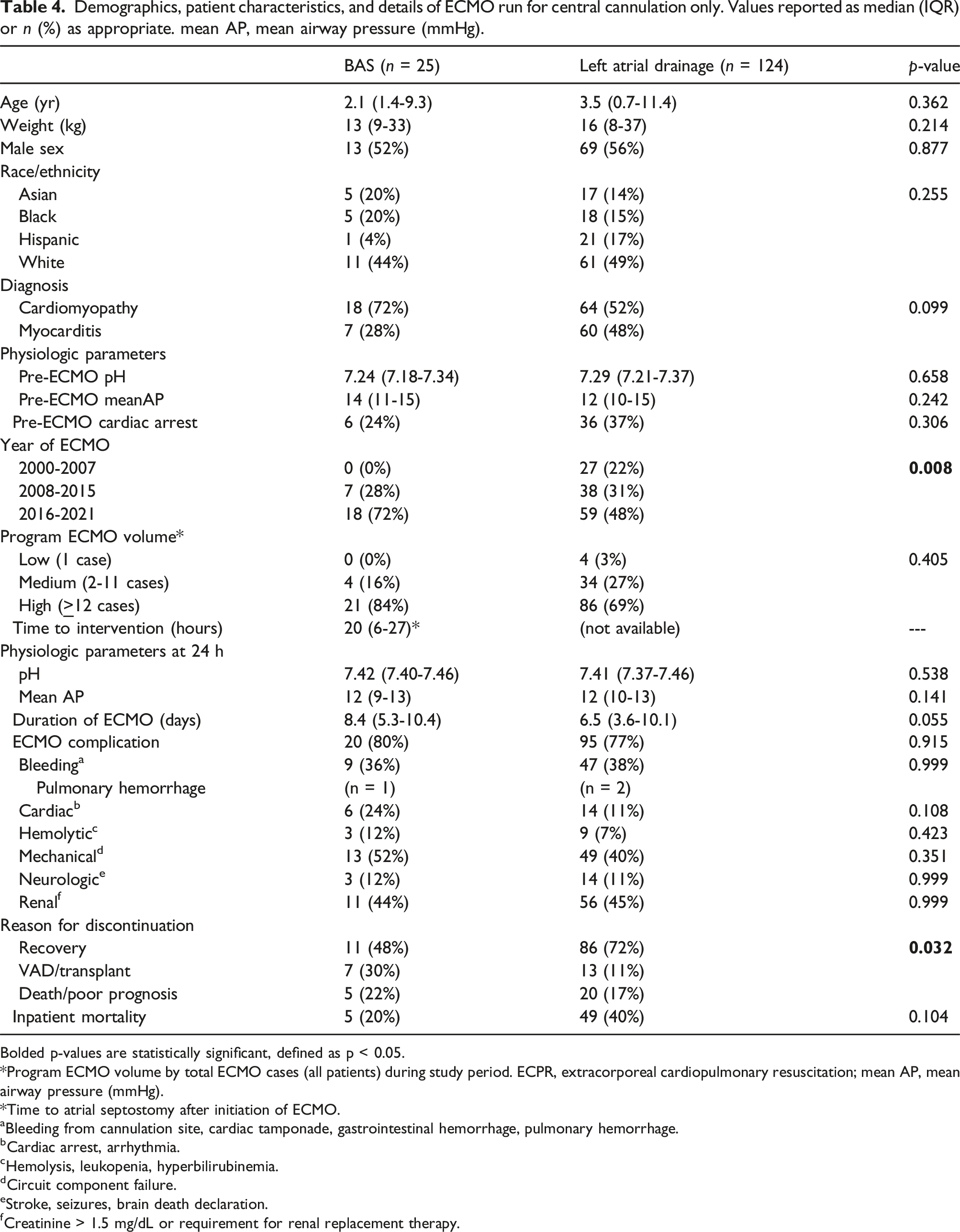
Bolded p-values are statistically significant, defined as p < 0.05.
*Program ECMO volume by total ECMO cases (all patients) during study period. ECPR, extracorporeal cardiopulmonary resuscitation; mean AP, mean airway pressure (mmHg).
*Time to atrial septostomy after initiation of ECMO.
aBleeding from cannulation site, cardiac tamponade, gastrointestinal hemorrhage, pulmonary hemorrhage.
bCardiac arrest, arrhythmia.
cHemolysis, leukopenia, hyperbilirubinemia.
dCircuit component failure.
eStroke, seizures, brain death declaration.
fCreatinine > 1.5 mg/dL or requirement for renal replacement therapy.
Discussion
In this multicenter study of pediatric patients with myocarditis and dilated cardiomyopathy on venoarterial ECMO, LA decompression with BAS was associated with lower mortality when compared to direct placement of an LA cannula (LA drainage or Impella®). However, when adjusted for central ECMO cannulation only, there was no difference in mortality and the indication for ECMO discontinuation of recovery, versus VAD/transplant or death/poor prognosis, was greater in the LA drainage group. This finding was independent of severity of illness markers such as pre-ECLS pH and mean airway pressure. Additionally, there was a trend toward a greater number of episodes of pulmonary hemorrhage in the BAS group compared to the LA drainage group, possibly indicating inadequate decompression in the BAS group. To our knowledge, this is the first study to compare mode of LA decompression in this population.
Inadequate LV decompression in patients on VA ECMO for left ventricular systolic dysfunction, results in left atrial hypertension. Left atrial hypertension, in turn, leads to pulmonary edema, pulmonary hemorrhage, and pulmonary vascular injury and, ultimately, lung injury. This lung injury complicates the management and weaning strategies of the patient on VA ECMO. 3 There was no difference in pre-ECMO mean airway pressure in our study, but we found 17 episodes of pulmonary hemorrhage in the BAS group, and only 3 in the LA drainage group. This might suggest inadequate decompression in the BAS group compared to the LA drainage group. A previous study has shown that larger cannula size and higher flow rates of a left atrial drainage cannula for decompression correlates with better outcomes. 6 Perhaps a larger cohort to evaluate LA pressure and pulmonary hemorrhage as a primary outcome following LA decompression could further evaluate the significance of this finding.
Additional reasons, such as time to decompression, for greater mortality in the LA drainage group may be elucidated on further evaluation. Earlier time to left atrial decompression is associated with improved outcomes, likely due to lung protection from pulmonary edema/hemorrhage as well as minimizing distension and promoting myocardial recovery.3,7 While we were unable to report the time to decompression for the left atrial cannulation group, time to decompression was early in the BAS group (median of 17 h). Previous studies have shown that early LA decompression (< 18 h) was associated with a shorter duration of extracorporeal membrane oxygenation support and mechanical ventilation. 3 Presumably the LA drainage group had the LA cannula placed at the time of ECMO cannulation or shortly thereafter but may have been placed later in the course. Further study to adjust for this variable is warranted.
A greater number of patients with LA drainage were centrally cannulated for ECMO compared to those in the BAS group. Previous studies have shown variable complication rates in central compared to peripheral cannulation strategies.8–10 Thus, we adjusted for cannulation strategy in our analysis and performed a post-hoc analysis on central cannulation strategy only in both groups. We found a statistically significant greater likelihood for the indication for ECMO decannulation to be recovery as opposed to VAD/transplant or death/poor prognosis in the LA drainage group. While these post-hoc analyses were limited by a small sample size and were likely underpowered to show statistical significance, there was a 20% mortality rate in the BAS group, compared to 40% in the LA drainage group. There are comorbidities, such as prior sternotomies or vascular access issues that might lead to a central cannulation strategy compared to peripheral, that we were unable to adjust for and likely play a role in the overall outcomes. The differences in cannulation strategy imply these may be fundamentally different cohorts, and further evaluation is warranted.
Several limitations exist including the retrospective nature of this study and the limitations associated with a multi-institutional registry. Participation in the ELSO registry is voluntary, and thus may represent more experienced centers, which could lead to selection bias. Additionally, we were unable to report on center specific ECMO practice and method of left heart decompression preference across each center. There is also a lack of granularity of severity of illness in this patient population, including pre-ECMO ejection fraction and the presence of pre-ECMO pulmonary hemorrhage. However, we do include pre-ECMO mean airway pressure, which is a reasonable surrogate for the severity of lung disease prior to ECMO cannulation. We do not know the number of LA drainage patients who had cardiopulmonary bypass prior to ECMO in the same admission (open or recently closed chest may lead to easier access for ECMO than percutaneous cannulation), and how many of these were placed on ECMO as a failure to wean from bypass. We also were unable to determine the mean cannula size for LA drainage, which may impact outcomes given a small cannula size for LA drainage can lead to cannula thrombosis and therefore impact effectiveness of the LA decompression. Lastly, we do not have data on the time to LA cannula placement from initiation of ECMO in the LA drainage group. The ELSO registry is currently not able to identify the specific timing with regards to the initial cannula placement reliably. There will be some internal testing for those time periods in the future to validate that data point.
Conclusion
In children with myocarditis or DCM, there was a three times greater likelihood for mortality in those with LA drainage versus BAS for LA decompression. This may reflect an inherent difference in the patient populations. However, in patients undergoing central ECMO cannulation, there is better recovery from ECMO support in the LA drainage group and no difference in mortality, indicating there may be better left heart decompression in the LA drainage group for this specific group of patients. Further prospective evaluation with adjustment for severity of illness is warranted.
Footnotes
Author’s contribution
All authors provided substantial contributions to the conception or design of the work or the acquisition, analysis, or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; final approval of the version to be published; and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of conflicting interests
David LS Morales is a consultant for Abbott, Berlin Heart, CorMatrix/Azyio, Medtronic, and SynCardia Systems. Ravi R. Thiagarajan is supported by a grant from US Department of Defense Clinical Trial Award #W81XWH2210301, Callaghan Family Chair in Cardiac Critical Care. Farhan Zafar is employed as Procurement Surgeon for TransMedics, Inc.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.