
Abstract
Objectives
Colloids are added to the priming solution of the cardiopulmonary bypass (CPB) pump to maintain colloid osmotic pressure and prevent fluid overload. This study aimed to compare the effects of 6% hydroxyethyl starch (HES) 130/0.4 and ringer’s lactate (RL) priming solution on patients’ outcomes undergoing isolated heart valve surgery with CPB.
Methods
This randomized clinical trial included one hundred and 20 patients undergoing heart valve surgery, and those were allocated into two groups. Patients in the RL group received 1500 mL of RL, and those in the RL + HES group were given 500 mL of HES and 1000 mL of RL.
Results
The patients’ median age was 52 (IQR 42–60) and 50 (IQR 40–61) years in the RL + HES and the RL group, respectively (p = .71). The number of cases that required blood product transfusion in both the operating room and intensive care unit was also significantly higher in the RL + HES group compared to the RL group (RR 2.04, 95% CI 1.50–2.76; p < .01 and RR 1.42, 95% CI 1.01–2.01; p = .05, respectively). Declines in postoperative creatinine levels and platelet counts were higher in the RL + HES compared to the RL group (between-subjects effect p = .007 and p = .038, respectively), while the incidence of acute kidney injury was comparable between groups (RR 0.66, 95% CI 0.13–3.30; p = .55).
Conclusions
Among patients undergoing heart valve surgery with CPB, 6% HES added to RL for priming compared with only RL increased the risk of the need for blood product transfusion over the hospitalization period.
Keywords
Introduction
Air removal from the cardiopulmonary bypass (CPB) circuit is accomplished using priming solutions. 1 Crystalloids, starch, gelatins, human albumin serum, or a mixture of these fluids with predetermined compounds are used for this purpose.2–4 Several crystalloids and colloid fluids have been used as a priming solution for CPB. Essentially, colloid fluids or human albumin have been added to the priming solution to maintain colloid osmotic pressure and avoid fluid retention.3,5 Mild and controlled blood dilution can be beneficial in cases of anemia because it can enhance the microvascular flow, while excessive blood dilution might be associated with harmful consequences. Therefore, in such a condition, in addition to a dramatic fall in hematocrit, coagulation factors, specifically fibrinogen and plasma proteins, can be significantly reduced. 6
Colloids are still predominantly used as a priming fluid, and hydroxyethyl starch (HES) and gelatin are the most widely utilized among those.3,7 However, some concerns have arisen regarding the impact of HES on blood coagulation. 8 Although it is claimed that using the new generation of HES (1330/0.38-0.45) has no dangerous effects on blood coagulation and renal function, recent concerns have surfaced. 9 Many studies have indicated that using HES (130/0.4) [Voluven®] instead of crystalloids can increase the risk of renal failure in ICU patients. (ICU). 10 Moreover, it can impair fibrin, clot formation, 9 and renal function during cardiac surgery. 11 A recent meta-analysis reported that using HES can be followed by more chest tube drainage, reoperation due to chest bleeding, and blood product transfusion compared to albumin.
Before this trial, our center’s protocol called for the use of RL + HES; however, previous research findings concerning renal complications and bleeding associated with RL + HES, along with the ongoing controversy surrounding the use of HES in cardiac surgery patients8–11 led us to decide to outline a study to compare the effects of adding 6% HES (130/04) to the ringer’s lactate (RL) versus only RL as priming solutions in patients undergoing isolated elective heart valve surgery.
Methods
Study design
In a randomized controlled trial (RCT) study, we assessed one hundred 40 adult patients undergoing elective open heart valve surgery in Tehran, Iran, from December 2016 to April 2021. The study was approved by the local ethics committee of Rajaie Cardiovascular Medical and Research Center (ID IR.RHC.IREC.1395.45). Upon enrolment into the study, informed consent was obtained from the participants. This study was registered at ClinicalTrials.gov (Trial identifier of NCT05223361).
Inclusion criteria required patients to provide signed informed consent, without heart failure with a left ventricular ejection fraction <40% at baseline, be free of hepatic failure defined as aspartate transaminase (AST) > 40 mg/dL and/or alanine transaminase (ALT) > 40 mg/dL, have no history of prior cardiac surgery, not experience drug-induced acute kidney injury within 5 days before surgery, without severe carotid stenosis, emergency valvular stenosis, infective endocarditis, severe right ventricular failure, heparin-induced thrombocytopenia, cancer, severe pulmonary valve insufficiency, and pulmonary function test defined as forced expiratory volume in one second <65% before heart valve surgery. In addition, patients were required to have serum creatinine level<1.5 mg/dL, a serum hemoglobin level ≥10 mg/dL, and a body mass index<40 kg/m2. Exclusion criteria included consent withdrawal by the patient or their proxy and any drug allergic reactions. Patients who underwent hemofiltration were also excluded.
Out of the 140 patients initially assessed for eligibility, we randomly assigned 120 adult patients aged ≥18 years into two groups at a 1:1 ratio, with 60 patients in the RL + HES group and 60 in the RL group (Figure 1). We used computer software to generate a table of random numbers for the simple randomization process. Patients were assigned numbers from 1 to 120, and 60 patients were then randomly assigned to either the RL + HES or RL groups. All participants, perfusionists, and surgeons were blinded to the study groups. An independent perfusionist not involved in this study prepared the priming solutions under sterile conditions and randomly allocated patients into the study groups. The priming solution was previously designed and was labeled with table numbers. To conceal the allocation into study groups, 120 envelopes were labeled with randomly assigned numbers. For the control group, 1250cc prime included 150 cc mannitol 20% and 1100cc RL were used, and the patients in the intervention group were given 1250 cc fluid as a prime. It contained 500cc of HES, 150cc of mannitol 20%, and 600cc RL, manufactured in Fresenius Kabi, Bad Homburg, Germany. Moreover, 10_15 mL per kilogram of RL was also administered in all patients pre CPB and post CPB. Study flow diagram.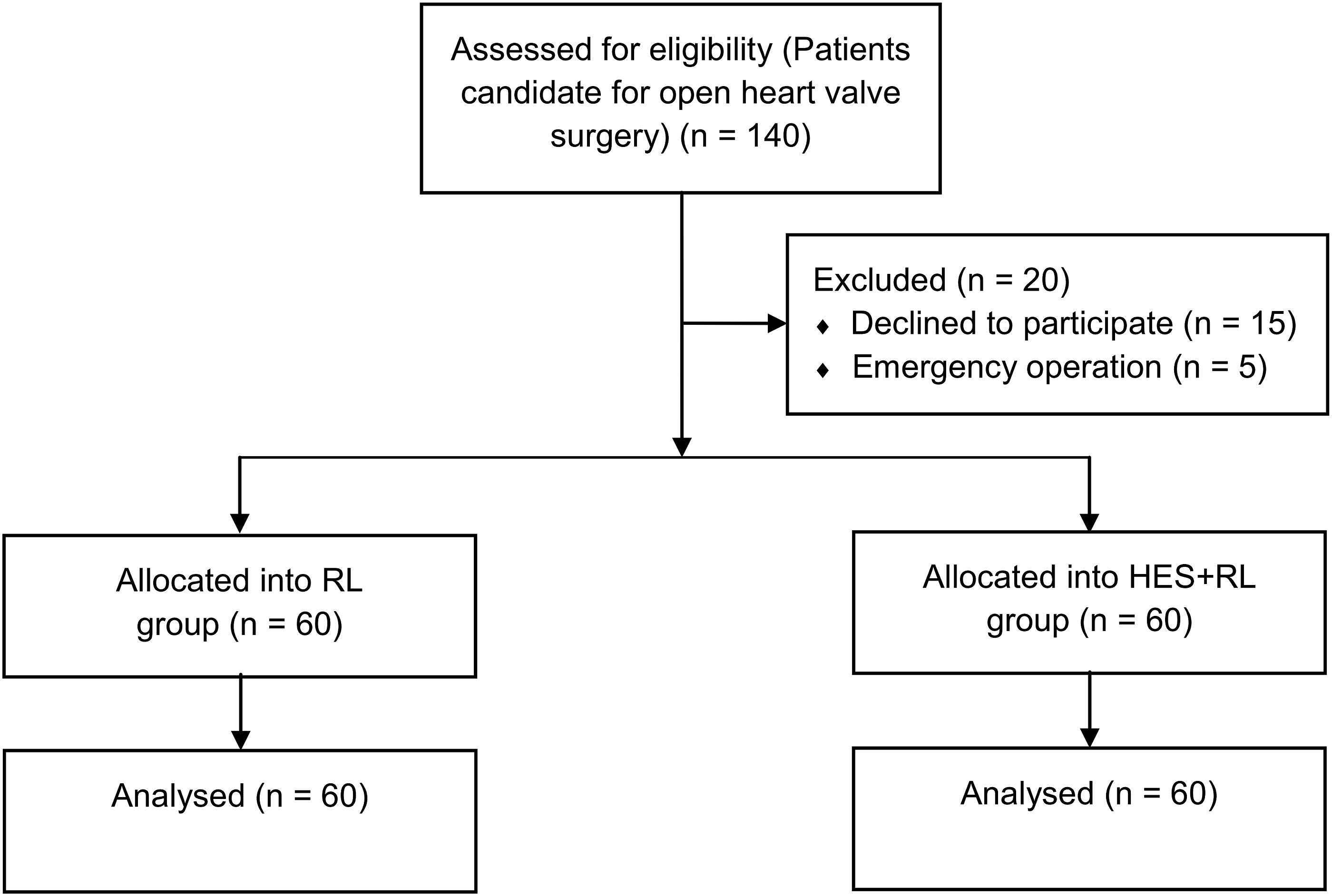
Surgical modalities
Baseline characteristics, pulmonary function test, renal function, coagulation parameters, and cerebral oxygenation were perioperatively collected. The cardiac function and blood oxygen saturation were routinely monitored, and peripheral venous access via an 18-gauge catheter was placed. Additionally, we inserted an arterial catheter for invasive radial blood pressure monitoring under regional anesthesia. The anesthesia was induced by the administration of etomidate (0.2 mg/kg), sufentanil (0.5 µg/kg), and atracurium (0.5 mg/kg). After intubation and mechanical ventilation, a central venous catheter was inserted via the left jugular vein to analyze the CVP. An arterial blood gas (ABG) was monitored too.
The temperature amount was also monitored by the nasopharyngeal. Cerebral oxygenation at both hemispheres was monitored trendily by INVOS from the onset of anesthesia, still at its end. When the cerebral oxygen was less than 50% or varied by more than 20% from the baseline value, that was a sign of an inappropriate amount of cerebral oxygenation that necessitated action.
The CPB was implemented using a roller pump, a membranous oxygenator (CAPIOX FX25) TERUMO, a non-pulsatile blood flow (2.4 mL/m2), moderate hypothermia (28–32°C), and maintaining blood pressure at a range of 50 to 80 mm Hg during surgery. The Hb was maintained above seven during surgery. Heparin at a dose of 3 mg/kg was given during the CPB as an anticoagulant, with an activated clotting time (ACT) target of 480. The near-infrared spectroscopy (NIRS) changes during the CPB. Patients with a stable hemodynamic status after surgery were weaned from the CPB, and protamine was administered to reverse the effects of heparin. The amount of chest tube drainage within the first 24 h in the ICU was assessed in both groups. After completion of the surgery, patients were transferred to the ICU.
Venous blood was drawn to assess coagulopathy and platelet counts before surgery, 12 h postoperatively and 24 h postoperatively. Likewise, hemoglobin and hematocrit levels were measured before inducing general anesthesia, after aortic cross-clamp (after injection of the cardioplegic agent), during the warming period, on arrival to the ICU, 12 h postoperatively, and 48 h postoperatively. If patients did not have active bleeding after 8 h of surgery, we started heparin infusion. Our goal was to maintain INR within the lower limit, and if our patients required maintenance anticoagulant medication, we added warfarin or NOAC. A hemoglobin concentration of around 8 g/d has been considered the cutoff for the transfusion of packed RBCs. Patients with massive bleeding have received FFP and platelet transfusions. Of note, according to the routine hospital practice, patients received packed red blood cells during the CPB time to maintain their hemoglobin over 7 g/dL and also were given packed red blood cells in the ICU to maintain hemoglobin level over 8 g/dL or above 9 g/dL in patients with hemodynamic instability. Moreover, patients received platelets if their platelet count was lower than 100,000 platelets per microliter of circulating blood.
Study endpoints
The primary endpoint of the study was the necessity for blood transfusion. Secondary endpoints included acute kidney injury (AKI), defined as a sudden reduction in renal function within 48 h, with an increase in serum creatinine of 0.3 mg/dL, 12 the need for renal replacement therapy, changes in the amount of liver function tests (i.e., AST and ALT), as well as ventilation times recorded at 12 and 48 h postoperatively in both groups. Additionally, the number of reoperations and the mortality rate during hospitalization and within 30 days after the operation were assessed in both groups.
Statistical analysis
A prior study involving patients undergoing mitral valve surgery revealed that half of the patients need a postoperative transfusion of blood products. 13 To achieve a 60% reduction in postoperative transfusion rates, we aimed for a statistical power of 90% with a two-sided α = 0.05. This led to the requirement of 55 participants per group. To account for an estimated 10% dropout rate during the research, we considered enrolling 60 patients per group to maintain study power. Categorical variables were presented as numbers (percentage) and values compared by chi-squared test between study groups. Continuous variables were reported as mean ± SD or median (interquartile range [IQR]), and those were compared between groups using a t-test or Mann-Whitney U test, as appropriate.
Moreover, a general linear model for repeated measurements was implemented to compare laboratory changes measured at several postoperative times in both groups. When sphericity assumptions were met, we reported sphericity-assumed p-values. In cases of sphericity violation, we adjusted degrees of freedom via the Greenhouse-Geisser correction. In addition, considering the status of sphericity, the between-subjects effect was reported for group comparisons. A 2-tailed p-value <.05 was considered statistically significant. All statistical analyses were performed using the STATA software (StataCorp, TX, USA).
Results
Baseline characteristics
Baseline characteristics and surgical features of patients in both study groups.
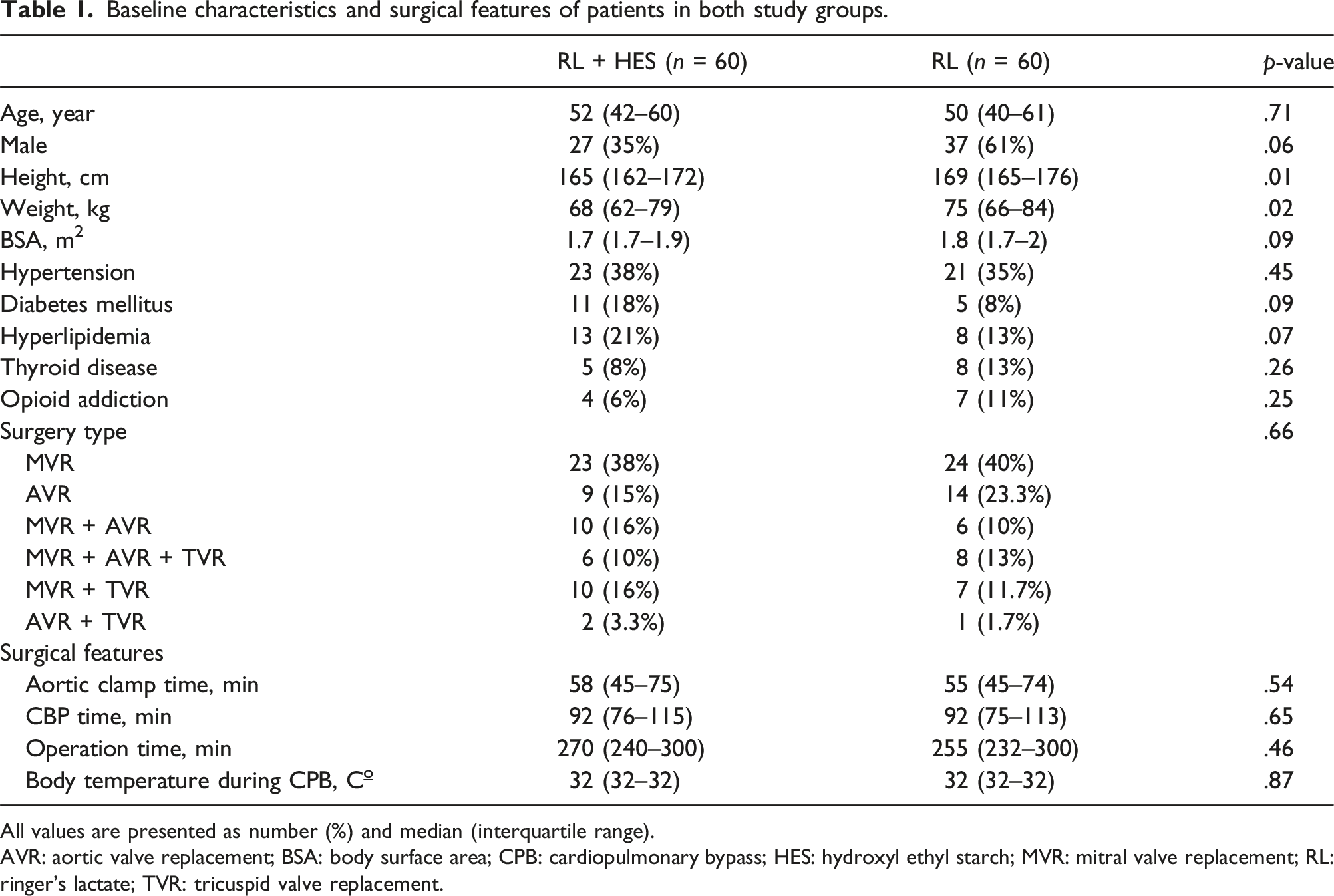
All values are presented as number (%) and median (interquartile range).
AVR: aortic valve replacement; BSA: body surface area; CPB: cardiopulmonary bypass; HES: hydroxyl ethyl starch; MVR: mitral valve replacement; RL: ringer’s lactate; TVR: tricuspid valve replacement.
Primary and secondary endpoints
Study endpoints measured in both study groups during the follow-up period.
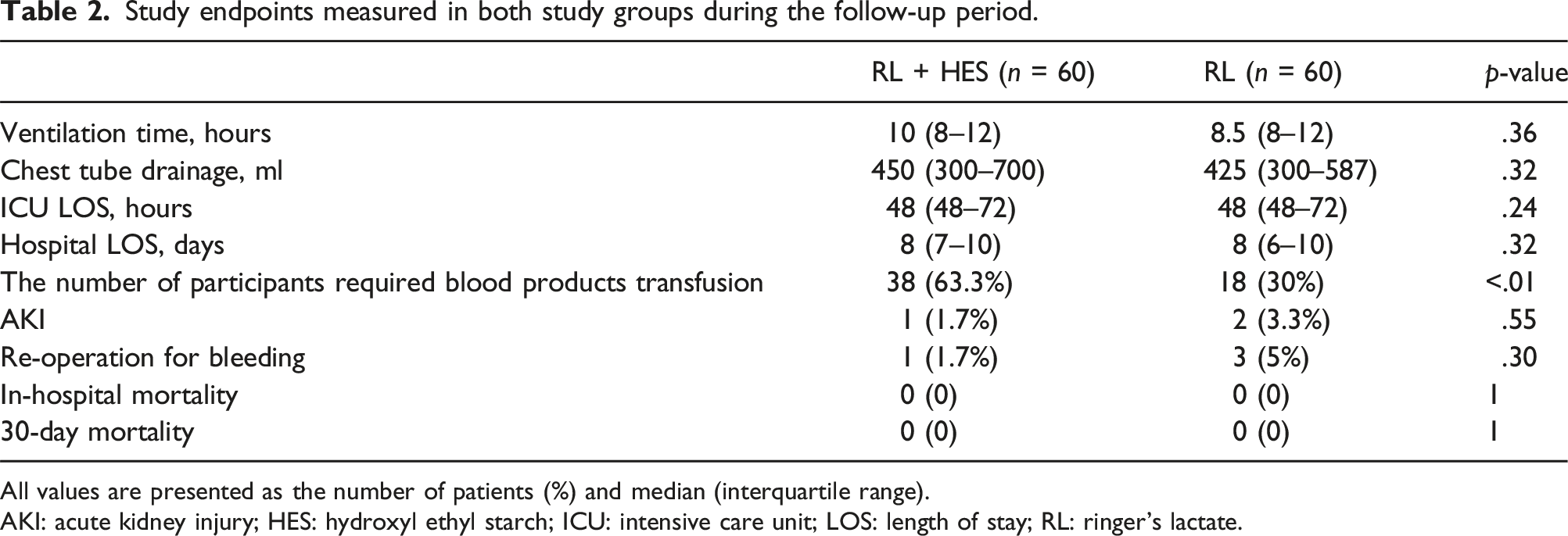
All values are presented as the number of patients (%) and median (interquartile range).
AKI: acute kidney injury; HES: hydroxyl ethyl starch; ICU: intensive care unit; LOS: length of stay; RL: ringer’s lactate.
The number of patients who transfused blood products in study groups during the hospitalization period.
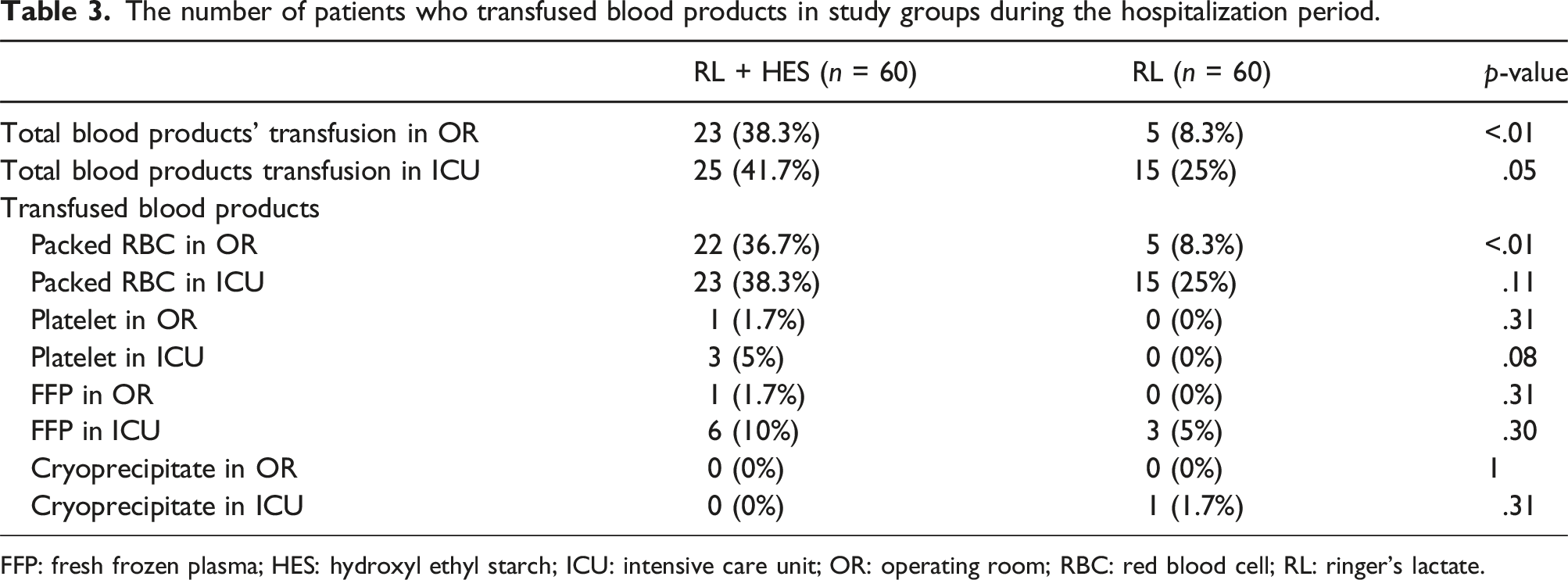
FFP: fresh frozen plasma; HES: hydroxyl ethyl starch; ICU: intensive care unit; OR: operating room; RBC: red blood cell; RL: ringer’s lactate.
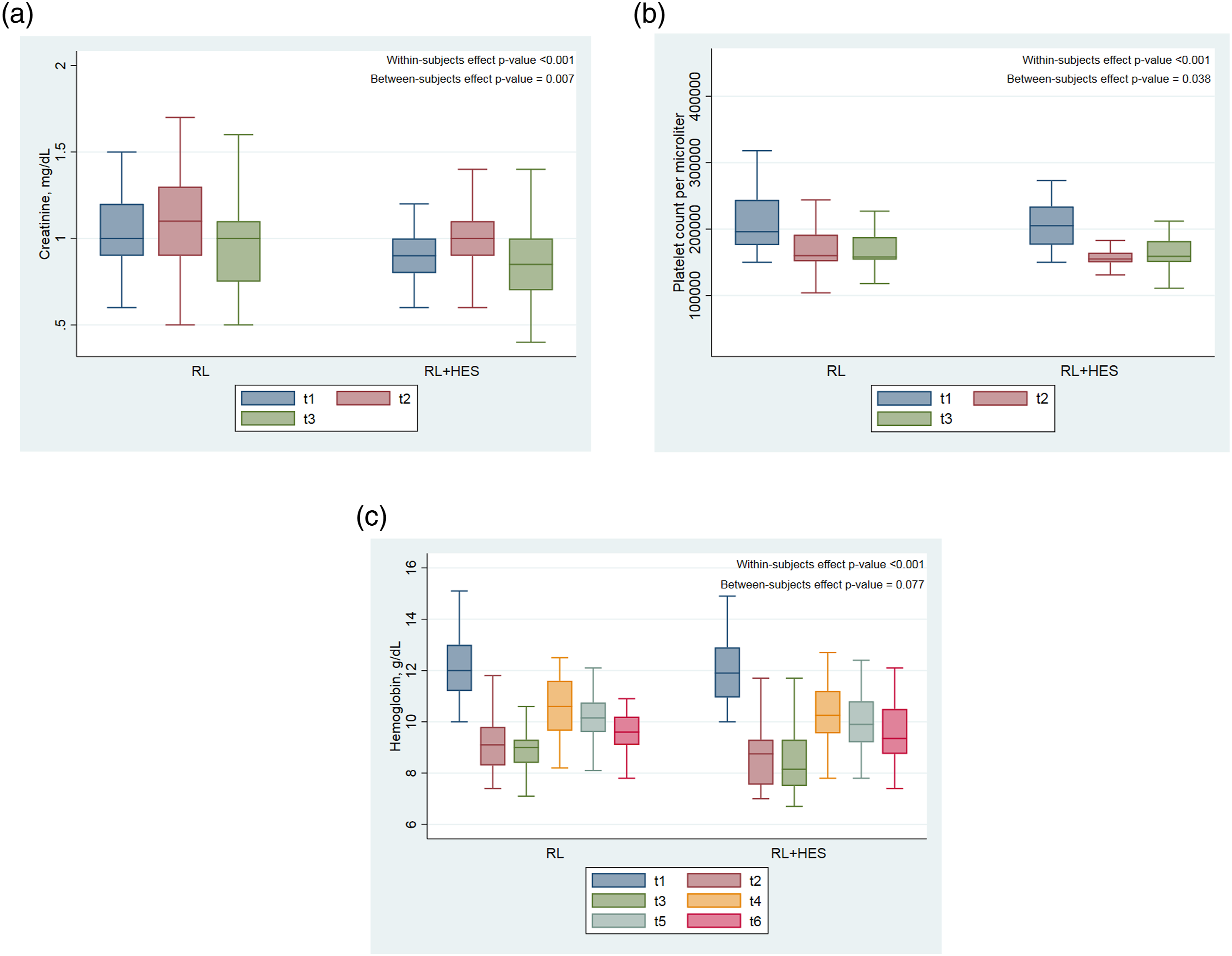
Postoperative changes in laboratories, including (a) creatinine, (b) platelet count, and (c) hemoglobin. Time assessments: t1, t2, and t3 were preoperative, 24 h postoperative, and 48 h postoperative, respectively, for creatinine and platelet counts; Time intervals for hemoglobin measurements including t1, t2, t3, t4, t5, and t6 were before anesthesia, after aortic cross-clamping, rewarming time, 12 h postoperative, 24 h postoperative, and 48 h postoperative, respectively.
Discussion
In our research, we observed a noteworthy increase in the requirement for blood product transfusions during isolated heart valve surgery with the use of CPB in the RL + HES compared to the RL group. We noted postoperative decreases in serum creatinine levels, and platelet counts were significantly higher in the RL + HES compared to the RL group. On the other hand, other endpoints, including AKI, liver function tests, and cerebral oxygenation, were comparable between the study groups.
Postoperative bleeding is common among patients undergoing open heart surgery, which is, in some parts, attributed to the CPB effects on coagulation systems and the activation of the complement system. 14 The type and volume of priming solution can play essential roles in the pathogenesis of derangements caused by CPB. Kuitunen et al. 8 revealed that HES as a priming solution for CPB impairs hemostasis after cardiac surgery and leads to higher blood loss through the chest tube than human albumin. Similarly, in another study involving adult patients undergoing cardiac surgery, the use of HES as a priming solution was associated with higher chest tube drainage and a greater need for blood product transfusions when compared to the use of balanced crystalloids. 15 In contrast, Tiryakioglu et al. 16 demonstrated no significant difference between HES and Ringer solution as CPB prime regarding the amount of blood product transfusion.
Furthermore, the mediastinal drainage, red cell, platelet, fresh frozen plasma requirements, and reoperation for postoperative bleeding were comparable between patients receiving low-molecular-weight HES and RL or human albumin as priming solution during cardiac surgeries. 17 A meta-analysis of studies that applied HES as a priming solution or perioperative volume expansion revealed that it is associated with increased risks of blood loss, reoperation for bleeding, and blood product transfusion after CPB. 18 In contrast, another meta-analysis of studies showed no difference between the colloid and crystalloid groups in terms of platelet count, blood loss, hematocrit levels, or the requirement for PRBC transfusions. In contrast to crystalloids, HES had lower fluid balances. 19 Our study, in line with these findings, showed that the RL + HES priming increased the requirements for blood product transfusion relative to the RL in adult patients undergoing isolated heart valve surgery. However, it’s worth mentioning that there exist some controversies regarding the effect of HES priming on postoperative bleeding.13,20–22 Based on our center experts’ opinions, the cause of the decrease in Hb in the RL + HES group probably is the shift of fluid from the interstitial space into the vessels in the RL + HES group and the fluid shift from intravascular to interstitial space in the RL group.
Renal function after cardiac surgery holds paramount importance due to its implications for prognosis, a factor influenced by various surgical-related variables. The effect of HES as volume replacement has not been associated with renal function deterioration in non-cardiac surgeries.23,24 Furthermore, a study conducted by Akkucuk FG and colleagues 25 evaluated the use of HES as a priming solution in children undergoing cardiac surgeries, demonstrating no adverse impact on postoperative renal function. Likewise, in the adult population undergoing CABG 26 and valve surgery, 22 the administration of HES as a priming solution did not significantly affect renal function. In contrast, Tiryakioglu et al. 16 reported that creatinine level after CABG surgery was higher in HES priming than in the RL priming group. Our study found that the development of AKI was comparable between the HES + RL and the RL group; however, the decrease in creatinine level was significantly higher among patients given the RL + HES. Further studies are required to evaluate the effect of HES as a priming solution on renal function in patients undergoing cardiac surgeries.
CPB can also deteriorate organ functions through mechanisms such as hemodilution, hypothermia, and ischemia-reperfusion injuries. 14 Shahbazi et al. 27 showed that tissue and organ perfusions were comparable among patients given HES or crystalloids as priming solutions. In an animal model, it has been demonstrated that the volume replacement following bleeding with HES was associated with maintaining the cardiac output and cerebral oxygenation during a more extended period than RL. 28 These results agree with previous suggestions that colloids improve cardiac performance in patients with hypovolemia. 29 This improvement is likely related to the fact that crystalloids are electrolyte solutions lacking intrinsic colloid osmotic pressure when entering the interstitial space. 30 In our study, cerebral oxygenation of cerebral hemispheres showed decreases in both groups, but the between-group difference was not significant. In addition, changes in liver enzymes were also comparable between the study groups. Our findings for organ perfusions in the setting of heart valve surgery were not clinically significant; however, these findings need to be re-investigated in large-scale studies.
Study limitations
This study is the first randomized clinical trial to evaluate the effect of 6% HES priming on outcomes of patients undergoing isolated heart valve surgery with CPB; however, it suffers from some limitations that need to be addressed in other studies. Firstly, we defined our sample size based on postoperative transfusion of blood products. It can be postulated that the small sample size can influence the lack of between-group differences for other endpoints. Secondly, we could not evaluate further details of coagulation and inflammatory factors to explore the proper effects of HES as a priming solution on patients’ outcomes undergoing heart valve surgery. Other large-scale randomized studies can provide valuable findings for our daily practice to improve patient outcomes and cost of care.
Conclusions
In this randomized clinical trial study, we revealed that the utility of RL + HES as CPB priming among patients undergoing elective isolated heart valve surgery led to a higher rate of need for blood product transfusion than using only RL priming fluid. Notably, we found the decline in postoperative creatinine level. The rate of AKI was comparable between groups. It is important to highlight that there was also a significant decline in platelet counts among patients in the RL + HES group.
Supplemental Material
Supplemental Material - Comparison of six percent hydroxyethyl starch 130/0.4 and ringer’s lactate as priming solutions in patients undergoing isolated open heart valve surgery: A double-blind randomized controlled trial
Supplemental Material for Comparison of six percent hydroxyethyl starch 130/0.4 and ringer’s lactate as priming solutions in patients undergoing isolated open heart valve surgery: A double-blind randomized controlled trial by Behzad Sheikhi, Yousef Rezaei, Farnaz Baghaei Vaji, Mostafa Fatahi, Mehdi Hosseini Yazdi, Ziae Totounchi, Sepideh Banar, Mohammad Mehdi Peighambari, Saeid Hosseini and Carlos - A Mestres in Perfusion.
Footnotes
Acknowledgements
We thank the operation room and intensive care unit staff for their whole-hearted support in data collection during the study conduction.
Author contributions
BS, ZT, MMP, SH and CM conceptualized and designed the study. BS, FB, MF, MHY, SB, and YR drafted the initial manuscript under the supervision of ZT, SH, and CM. YR, BS, SB, and SH performed the statistical and interpreted analyses. All authors revised critically, approved the final manuscript as submitted, and agreed to be accountable for all aspects of the work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Rajaie Cardiovascular Medical and Research Center.
Data availability statement
Rajaie Cardiovascular Medical and Research Center provided the article’s data with permission. De-identified data will be shared on request to the corresponding author via email address with the permission of the institution 12 months after the publication of all results, after approval of a proposal, and with a signed data access agreement.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.