
Abstract
Multisystem inflammatory disease in childhood (MIS-C) is a novel pediatric syndrome after a COVID-19 infection that causes systemic injury, with potential life-threatening hemodynamic compromise requiring Extracorporeal Membrane Oxygenation (ECMO) support. We performed an observational retrospective cohort study in children aged 0-18 years with MIS-C and non-MIS-C myocarditis on ECMO between January 2020 and December 2021, using the ELSO Registry database. We aimed to compare the outcomes of both populations and to identify factors for decreased survival in MIS-C patients on ECMO. The Extracorporeal Life Support Organization (ELSO) Registry reported 310 pediatric ECMO patients with MIS-C (56.1%) and non-MIS-C myocarditis (43.9%). No difference was found in survival to hospital discharge between groups (67.2% for MIS-C vs 69.1% for non-MIS-C myocarditis, p 0.725). Multivariable analysis demonstrated that ECPR and co-infection were significantly associated with decreased survival to hospital discharge in MIS-C patients (OR 0.138, p 0.01 and OR 0.44, p 0.02, respectively). Outcomes of children with MIS-C on ECMO support are similar to those of non-MIS-C myocarditis despite higher infectious, multiorgan dysfunction and respiratory complications accompanying COVID-19 infections. The use of ECMO for MIS-C patients seems to be feasible and safe. Prospective studies on the use of ECMO support in MIS-C patients may improve outcomes in this pediatric population.
Keywords
Introduction
Multisystem inflammatory disease in childhood (MIS-C) is a novel post-viral inflammatory vasculopathy and myocarditis in children following Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2) infection that resembles a severe variant of Kawasaki’s disease, toxic shock syndrome, and acute myocarditis.1–3 Cases of MIS-C started to emerge in May 2020 weeks after Coronavirus disease-19 (COVID-19) outbreaks in patients with negative COVID-19 reverse-transcriptase polymerase chain reaction (RT-PCR) tests and positive serum levels of anti-SARS-CoV2 antibodies.1,2,4
Currently, the Center for Disease Control and Prevention (CDC) defines MIS-C as an individual less than 21 years of age presenting with fever for >24 h and clinically severe disease requiring hospitalization with laboratory evidence of inflammation involving more than two organ systems. 5 They must have current or recent SARS-CoV-2 infection or have been exposed to a positive individual within 4 weeks of onset and no other plausible diagnosis. 5 By the end of 2022, the CDC reported 9,333 cases and 76 deaths that met the case definition for MIS-C in the United States. The median age was 9 years, 60% were males, and 56% were of Hispanic or African American race. 6
Myocarditis is an inflammation of the myocardium of infectious and non-infectious etiologies due to immunological and systemic disorders, toxins, and drug toxicity or hypersensitivity with different outcomes. 7 COVID-19 virus has tropism for myocardial cells and may lead to immune activation and myocardial tissue inflammation, causing post-infectious myocarditis. 1 MIS-C patients present a wide spectrum of severity with a shock-like syndrome, myocardial dysfunction, need for vasopressor support, and risk for decompensation requiring Extracorporeal Membrane Oxygenation (ECMO).2,3,8–10
Despite the above similarities, data comparing the clinical characteristics and outcomes of MIS-C and non-MIS-C myocarditis patients requiring ECMO remain limited. The aim of our study was to characterize outcomes of MIS-C and non-MIS-C myocarditis patients requiring ECMO support and to identify factors associated with decreased survival in MIS-C patients supported on ECMO.
Materials and methods
Study design and population
The study was conducted with data from the Extracorporeal Life Support Organization (ELSO) registry database. It was designed as an observational, retrospective cohort study. The ELSO Registry contains de-identified ECMO data from multiple institutions around the world. The Institutional Review Board of the University of Tennessee Health Science Center determined this analysis to be exempt from human participant review.
All neonatal and pediatric ECMO patients ≤18 years of age who received ECMO support as recorded in the ELSO registry between January 1, 2020, and December 31, 2021, with diagnoses of myocarditis and MIS-C were included in the analysis. We excluded 10 patients with incomplete data and secondary ECMO runs.
Definitions and data collection
Primary and secondary diagnoses with International Classification of Disease (ICD) 10 codes for myocarditis (I51.4, I40.0, I40.1, I40.8, I40.9) and MIS-C (M35.8, M35.81, B94.8) were utilized. Patients with ICD-10 codes for both myocarditis and MIS-C were assigned to the MIS-C group. Despite the CDC definition for MIS-C including patients up to 21 years of age, we excluded those older than 18 to fit societal norms in international pediatric hospitals. Patients with ICD-10 codes for pre-diagnosed heart failure were also excluded. We defined ECMO mode as venovenous (VV) when both drainage and return cannulas were in the venous system for the entire ECMO run. Patients on venoarterial (VA) ECMO or any conversion to or from VA ECMO were defined as VA. Support type was classified as pulmonary, cardiac, and Extracorporeal cardiopulmonary resuscitation (ECPR) per ELSO registry definitions. Database included information regarding demographics, comorbid conditions, pre-extracorporeal life support, ECMO support, and outcomes. ECMO complications and adjuvant therapies for myocarditis and MIS-C were also included.
The ELSO data from patients suspected to have MIS-C at the beginning of the pandemic when immunoglobulin testing was not available was also included. These patients fit the current CDC diagnosis with a previous SARS-CoV-2 infection and no other identifiable source of infection or inflammation. Based on the ELSO SARS-CoV-2 addendum form, “co-infection” was defined as the presence of a co-viral infection, bacterial pneumonia, blood stream infection, and/or urinary tract infection. “Comorbidity” was defined as the presence of co-diagnoses during MIS-C such as Acute Respiratory Distress Syndrome (ARDS), pneumonia, septic shock, myocarditis, heart failure, acute renal failure, and pneumothorax, as well as the need for renal replacement therapy present in the ELSO SARS CoV-2 addendum form. The immunomodulatory therapies used that were documented in this form were also evaluated.
Aims and outcomes
We aimed to outline outcomes of MIS-C and non-MIS-C myocarditis patients requiring ECMO support and to identify factors for decreased survival in MIS-C patients on ECMO. The primary outcome was survival to hospital discharge. Secondary outcomes included ECMO duration, mechanical ventilation (MV) duration, length of stay (LOS), and requirement of orthotopic heart transplantation (OHT) or ventricular assist device (VAD) for ECMO decannulation.
Statistical analysis
Continuous variables were described using medians and interquartile ranges (IQR) while categorical variables were described using frequencies and percentages. Chi-square goodness of fit test for comparison of categorical variables and t-test for continuous variables were utilized to ascertain differences in characteristics and outcomes between MIS-C and non-MIS-C myocarditis patients. Univariate and multivariable logistic regression with backward elimination models were utilized to analyze the effects of different variables on survival in MIS-C patients. Odds ratios (OR) and 95% confidence intervals (CI) were calculated and only the statistically significant variables with p-value ≤.05 were considered. All the statistical analyses were performed using SAS software, version 9.4, Copyright © 2016 by SAS Institute Inc, Cary, NC, USA.
Results
Patient characteristics, adjuvant therapies, and complications during ECMO support
Demographic, clinical characteristics and outcomes of MISC and non-MISC myocarditis patients.
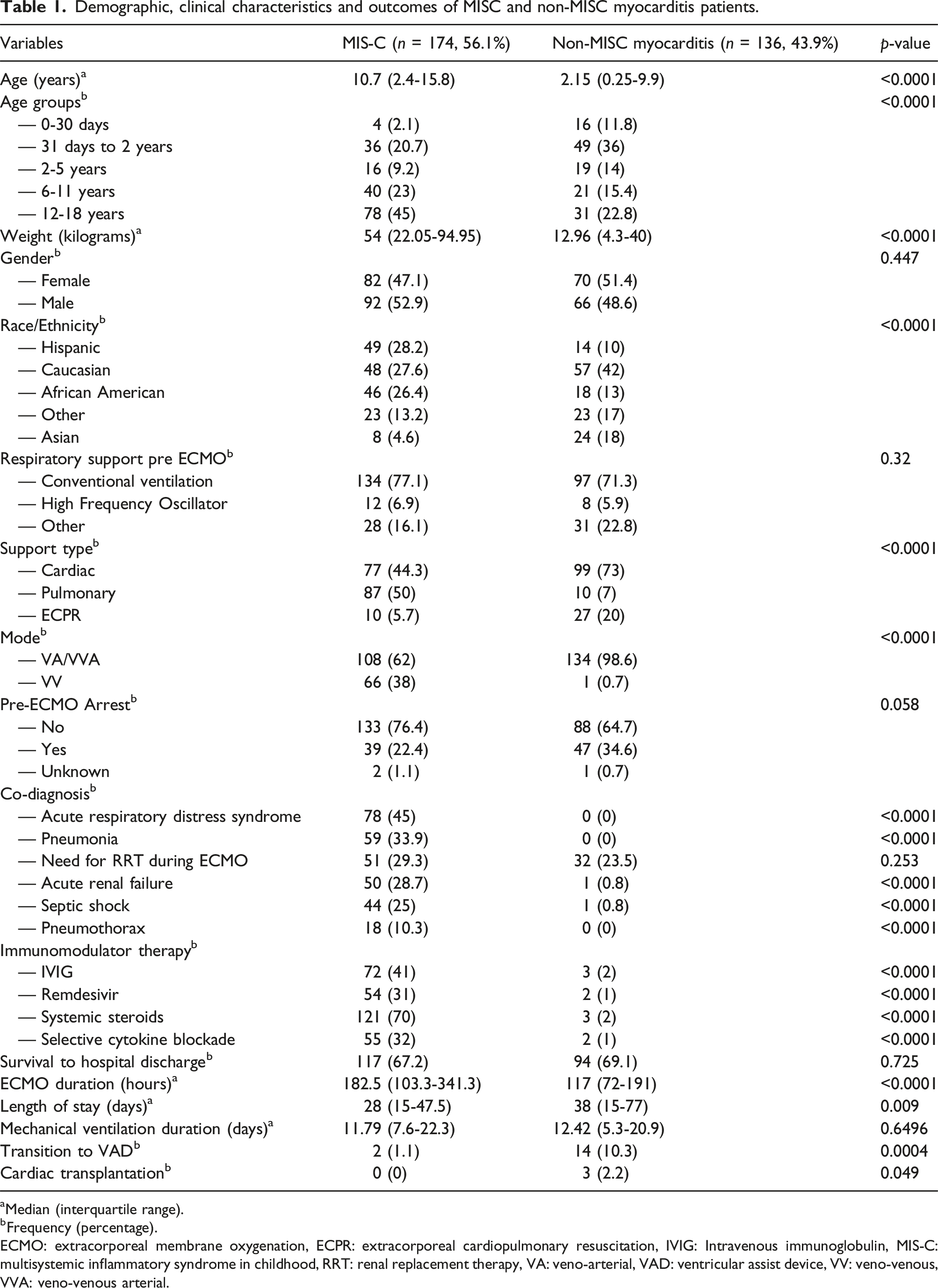
aMedian (interquartile range).
bFrequency (percentage).
ECMO: extracorporeal membrane oxygenation, ECPR: extracorporeal cardiopulmonary resuscitation, IVIG: Intravenous immunoglobulin, MIS-C: multisystemic inflammatory syndrome in childhood, RRT: renal replacement therapy, VA: veno-arterial, VAD: ventricular assist device, VV: veno-venous, VVA: veno-venous arterial.
During ECMO support, MIS-C patients received significantly higher rates of intravenous immunoglobulins (IVIG) (41% vs 2%, p < .0001) as compared to non-MIS-C myocarditis patients. As expected, there was also a significantly higher use of systemic steroids and other immunomodulator therapies in MIS-C patients. Table 1
ECMO complications for MIS-C and non-MIS-C myocarditis patients.
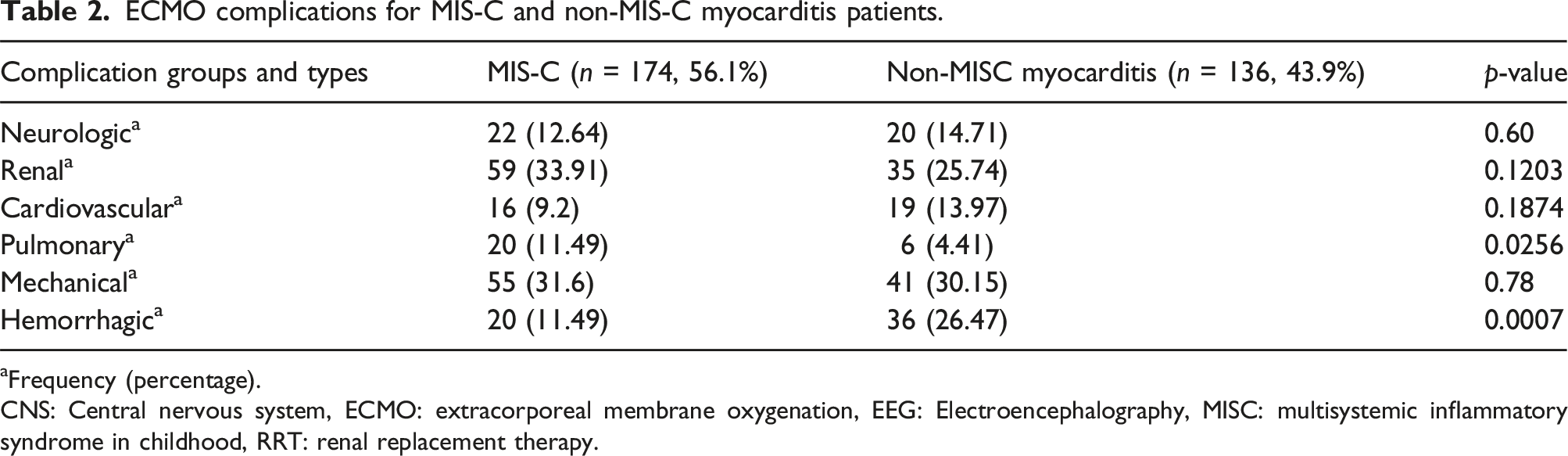
aFrequency (percentage).
CNS: Central nervous system, ECMO: extracorporeal membrane oxygenation, EEG: Electroencephalography, MISC: multisystemic inflammatory syndrome in childhood, RRT: renal replacement therapy.
Primary and secondary outcome measures
Median ECMO duration was significantly longer in MIS-C patients (182.5 h vs 117 h, p < .0001), while LOS was significantly longer in non-MIS-C myocarditis patients (38 days vs 28 days, p 0.009). A significantly higher proportion of non-MIS-C myocarditis patients required transition to a VAD (10.3% vs 1.1%, p 0.0004) for ECMO decannulation and 2.2% underwent OHT post ECMO support. Survival to hospital discharge was not statistically different between groups (67.2% for MIS-C vs 69.1% for non-MIS-C myocarditis, p 0.725). Table 1.
Analysis by support type
A secondary analysis was performed to define patient outcomes related to myocardial involvement only by removing patients supported on VV ECMO. When analyzing only VA/VVA modes. MIS-C and non-MIS-C myocarditis patients accounted for 108 (44%) and 135 (56%), respectively. Comparable to the whole cohort, MIS-C patients were significantly older (9.1 vs 2.1 years old, p < .0001) and had significantly lower rates of cannulation via ECPR (9% vs 20%, p < .0008). Despite eliminating VV mode, MIS-C patients continued to have significant higher rates of ARDS (29.6% vs 0%, p < .0001), pneumonia (19.4% vs 0%, p < .0001), septic shock (28.7% vs 0.7%, p < .0001), and acute renal failure (31.5% vs 0.7%, p < .0001) compared to non-MIS-C myocarditis patients. Hemorrhagic complications remained significantly higher in non-MIS-C myocarditis patients (17.1% vs 7.4%, p 0.045). Similar to the analysis of the whole cohort, survival to hospital discharge was not statistically different between groups (72.2% for MIS-C vs 69.6% for non-MIS-C myocarditis, p 0.65), non-MIS-C myocarditis patients had significantly longer LOS (25.5 days vs 38 days, p 0.02) and a higher proportion required transition to a VAD (10.4% vs 1.9%, p 0.0078) for ECMO decannulation and 2.2% of them underwent OHT post ECMO support. Mechanical ventilation duration was also significantly longer in this group (10 days vs 12.4 days, p 0.04). (Supplementary Tables 1 and 2)
Regarding the VV cohort, the median age and weight were 14.8 years (IQR 5.1, 16.6) and 93 kg (IQR 58.8, 113.5), respectively. Cannulation via ECPR occurred in one patient. Primary diagnoses for VV mode was pneumonia due to coronavirus infection (64%), acute respiratory failure (13.4%) and ARDS (8.9%). Co-diagnoses occurred in 65.6% of patients and ECMO complications in 32.8%. Median MV duration and LOS reached 17.5 days (IQR 9.9, 29.2) and 32 days (IQR 21, 50.5), respectively. A total of 55% of patients survived to hospital discharge.
Effects of variables on survival to hospital discharge in MIS-C patients
Effects of variables on survival to discharge in MIS-C patients.
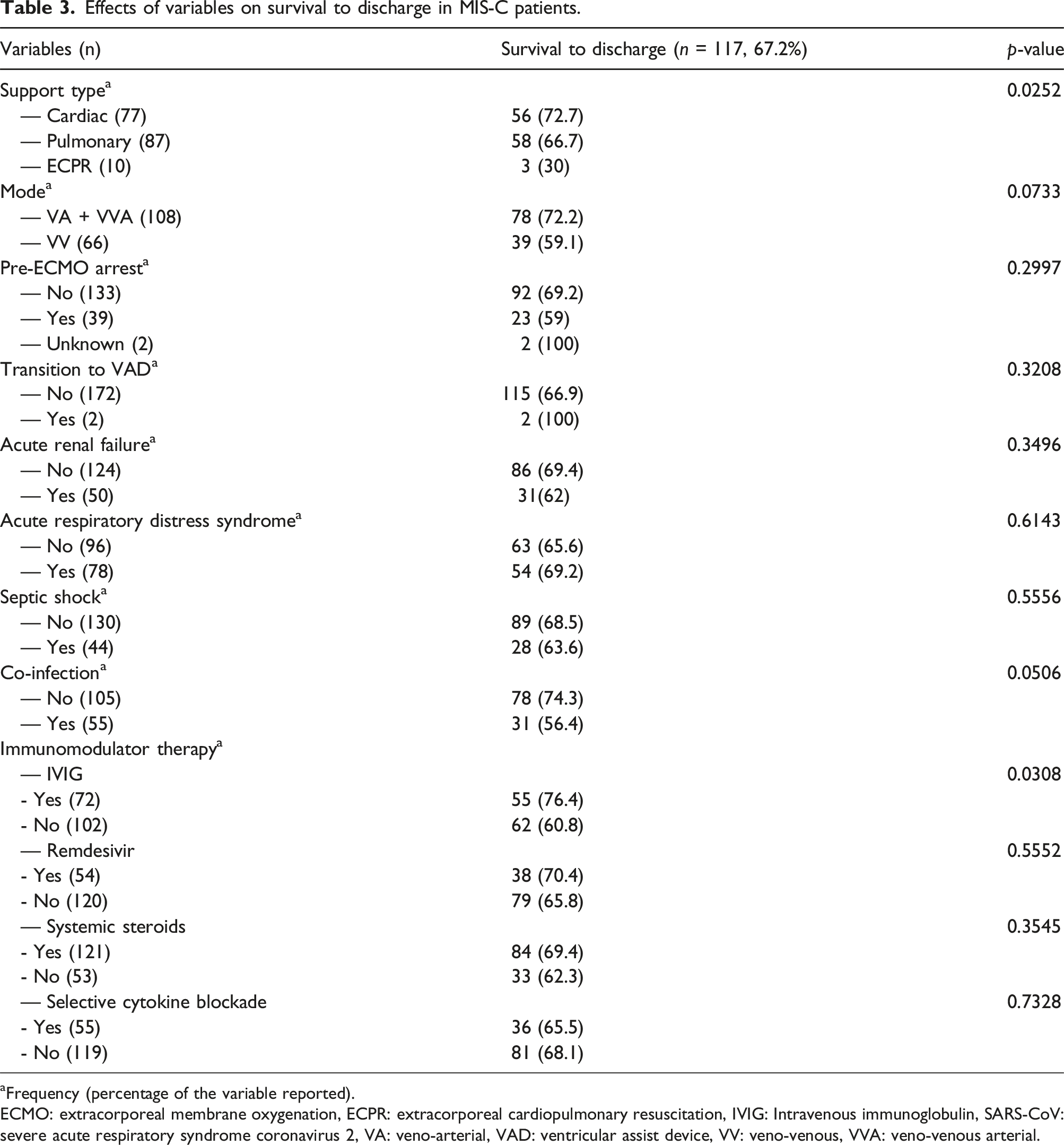
aFrequency (percentage of the variable reported).
ECMO: extracorporeal membrane oxygenation, ECPR: extracorporeal cardiopulmonary resuscitation, IVIG: Intravenous immunoglobulin, SARS-CoV: severe acute respiratory syndrome coronavirus 2, VA: veno-arterial, VAD: ventricular assist device, VV: veno-venous, VVA: veno-venous arterial.
Univariate logistic regression to ascertain for factors associated with survival to discharge in MIS-C patients.
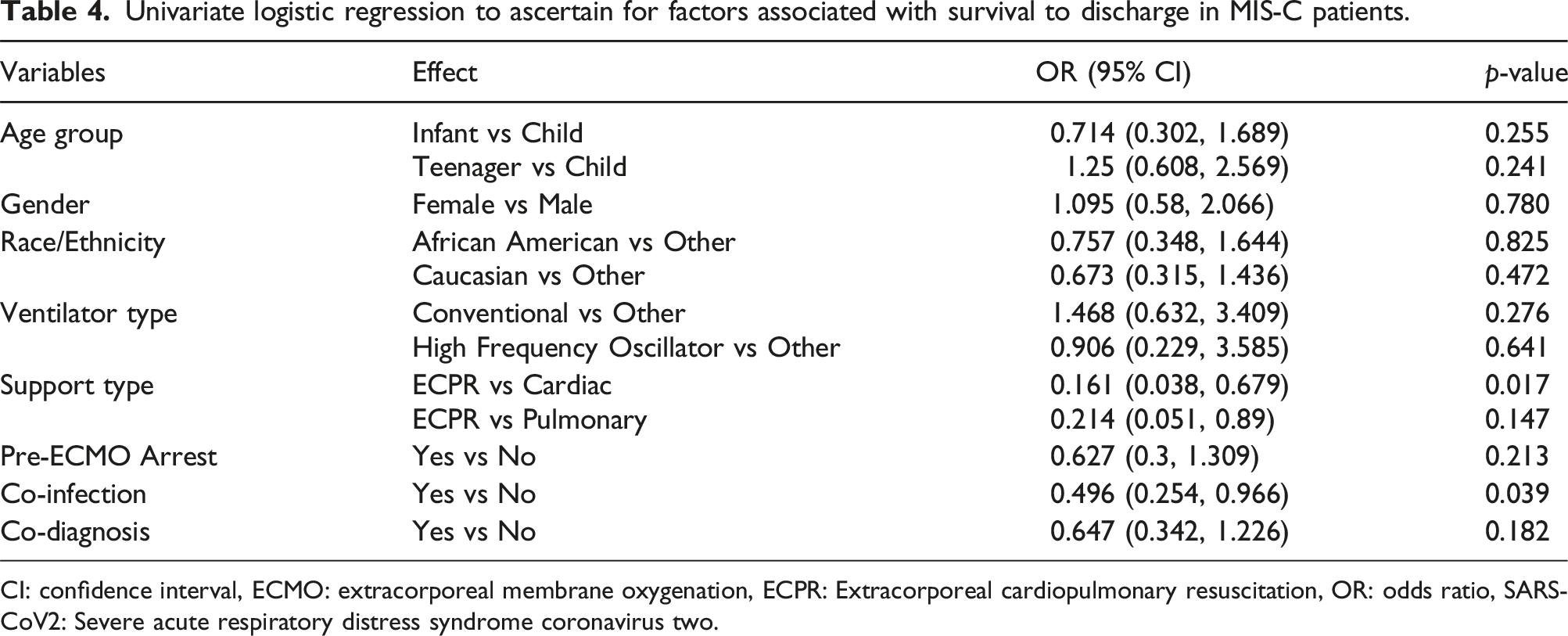
CI: confidence interval, ECMO: extracorporeal membrane oxygenation, ECPR: Extracorporeal cardiopulmonary resuscitation, OR: odds ratio, SARS-CoV2: Severe acute respiratory distress syndrome coronavirus two.
Multivariable model after backward variable elimination to identify factors associated with survival to discharge in MIS-C patients.

CI: confidence interval, ECPR: Extracorporeal cardiopulmonary resuscitation, OR: odds ratio.
Discussion
Our study is the first report of MIS-C patients on ECMO support from the ELSO Registry database. Recent case series demonstrated that using ECMO in MIS-C and COVID-19 patients is feasible and markedly contributes to their prognosis.2,9,11–15 Our primary finding is that survival to hospital discharge in MIS-C patients on ECMO was similar to pre-pandemic rates reported by ELSO in mixed pediatric populations and pandemic multicenter studies in children supported on ECMO for MIS-C.2,11,16 Our ELSO data demonstrated lower rates of ECPR in MIS-C patients (5.7%) compared to the Overcoming COVID-19 Public Health Surveillance Registry showing an incidence of 19% in their 37 MIS-C patients requiring ECMO support. 2 Despite our lower rates and in line with other ECMO studies, ECPR seemed to be a predictor for decreased survival to hospital discharge in our ELSO cohort of MIS-C patients. 17 This also suggests that when facing patient deterioration, it is reasonable to consider a “planned” cannulation to prevent ECPR in MIS-C patients. Other predictors for decreased survival were the presence of a MIS-C co-infection and Caucasian race in VA/VVA modes only. Coinfection at the time of MIS-C seems to be a predictor since concomitant infections may negatively impact outcomes; however, we cannot draw conclusions regarding the effect of the Caucasian race on mortality.
Previous studies demonstrated health disparities during the pandemic, with African American and Hispanic children constituting a disproportionate majority of patients receiving ECMO for MIS-C. 2 Our ELSO data showed a similar distribution of MIS-C patients requiring ECMO among African American, Hispanic, and Caucasian children, speaking against this finding. Comparable to CDC data and other studies, MIS-C patients requiring ECMO support were school-aged (median 9–10 years old).2,5 These patients were older than non-MIS-C myocarditis patients. The lower age in non-MIS-C myocarditis patients may have contributed to faster deterioration and the need for ECMO support, as well as to the complication profile, given the neonatal preponderance in this group (20.5%).
Our cohort of MIS-C patients on ECMO had high rates of respiratory, infectious, and renal co-diagnoses (ARDS, pneumonia, septic shock, acute renal failure, and the need for renal replacement therapies) compared to those of non-MIS-C myocarditis patients. This is likely due to the immune-mediated systemic response to the previous SARS COV-2 infection, whereas other forms of myocarditis are limited primarily to the myocardium, and end-organ dysfunction occurs due to inadequate cardiac output. However, these co-diagnoses were not associated with decreased survival to hospital discharge unlike most other disease processes needing ECMO.18,19 The longer ECMO duration in the MIS-C group may be secondary to the multisystem (especially pulmonary) inflammatory involvement and the significant number of concomitant infections in these patients.
Regarding complications, the significant number of respiratory co-diagnoses in MIS-C patients may have contributed to higher rates of pulmonary complications in this cohort. Studies have demonstrated higher rates of thromboembolic events in MIS-C patients, negatively impacting outcomes. 20 We did not find increased thrombosis rates in our MIS-C cohort, probably due to the systemic anticoagulation management used during ECMO in these patients. Most of the ECMO hemorrhagic complications in non-MIS-C myocarditis patients occurred at the surgical site. We believe patient size played a role in the higher proportion of this complication type due to the age and weight predominance in this group. Despite the complication rates, ECMO decannulation as a result of a life-threatening complication only occurred in two MIS-C patients and in none of the non-MIS-C myocarditis patients.
In their subpopulation of MIS-C patients on ECMO, Bembea et al. demonstrated that up to 13% were cannulated for respiratory reasons and 8% were VV supported. 2 We eliminated the VV mode in a secondary analysis to align the cardiac pathophysiology of the MIS-C and myocarditis cohorts more accurately. There were minimal differences in clinical characteristics, co-diagnosed conditions, and complications when the analysis included only VA/VVA modes. Survival to hospital discharge remained similar in both MIS-C and non-MIS-C myocarditis patients despite removing VV mode.
The use of MIS-C adjuvant therapies during ECMO support has been described in a few reports.10,13,15 When analyzing the use of concomitant therapies in our ELSO MIS-C cohort, survival to hospital discharge seemed to be influenced by the use of IVIG in these patients but was not an outcome predictor. This aligns with previous MIS-C literature demonstrating better outcomes with IVIG therapy.9,10 The sample size of non-MIS-C myocarditis patients who received IVIG was small, leaving us unable to draw conclusions about its effect on survival. The use of systemic steroids and other immunomodulators did not show differences in survival in any cohort. This aligns with conflicting myocarditis literature where the use of IVIG and steroids remains controversial.7,21
A higher proportion of non-MIS-C myocarditis patients were transitioned to a VAD for decannulation and underwent OHT post-ECMO, which may explain their longer mechanical ventilation duration and LOS. This finding may speak to the reversibility of MIS-C related cardiac inflammation and myocardial damage as compared to other forms of myocarditis, as described in previous MIS-C reports.10,13,14 Wu et al, described biopsy results of MIS-C patients with evidence of the SARS-COV-2 virus within the myocardium, evidence of myocardial inflammatory response, and even contraction band necrosis at autopsy. 22 Coronary artery dilation could also play a role in arteritis and coronary ischemia. 22 The combination of these findings suggests that the myocardial damage seen in MIS-C is multifactorial.22,23 Despite functional recovery, late gadolinium enhancement on cardiac magnetic resonance imaging at 6 months post-treatment in MIS-C patients suggests lasting fibrosis and scar formation within the myocardium. 23 Regardless of the multiple co-diagnosed conditions, systemic inflammation, prolonged ECMO courses, and need for other forms of mechanical support such as renal replacement therapy, MIS-C patients were able to recover their cardiac function without significant need for more durable circulatory support or transplantation, required shorter duration of mechanical ventilation and went home earlier.
This study has some limitations. It is a retrospective review of an international database. The accuracy of the ELSO data depends on voluntary reports from multiple institutions worldwide, so missing or inaccurate information may confound outcomes. Criteria for ECMO deployment and management for MIS-C patients were not standardized, leaving us unable to draw definite conclusions. We were limited by the data in the registry and could not adjust for other factors that might be associated with survival to hospital discharge, such as severity of illness, co-infection type, and other unrecorded pre-existing conditions or complications. Differences in age and weight between groups may have also impacted outcomes. We were also limited by the number of patients who received immune modulators as this was retrospective and not standardized at each institution. This limits our ability to conclude how those affect survival. Finally, the degree of myocardial involvement in MIS-C patients could be variable, complicating the comparison between the two populations.
Conclusion
Outcomes of children with MIS-C requiring ECMO support are similar to those of non-MIS-C myocarditis despite higher infectious, multiorgan dysfunction and respiratory complications accompanying COVID-19 infections. The use of ECMO in MIS-C patients for hemodynamic and respiratory support seems to be feasible and safe. Prospective studies on the use of ECMO support in MIS-C patients may improve outcomes in this pediatric population.
Supplemental Material
Supplemental Material - “Extracorporeal membrane oxygenation outcomes in multisystem inflammatory syndrome of childhood – An ELSO registry study”,
Supplemental Material for “Extracorporeal membrane oxygenation outcomes in multisystem inflammatory syndrome of childhood – An ELSO registry study”, by Noah Miller, Hitesh S Sandhu and Pilar Anton-Martin in Perfusion
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.