
Abstract
This case report describes the pharmacokinetics of levetiracetam in a critically ill patient supported on venovenous membrane oxygenation. While levetiracetam has emerged as a first line option to treat seizures in critically ill patients, there is limited information available regarding the impact of extracorporeal membrane oxygenation on the pharmacokinetics of this medication. This report contributes to the limited body of literature describing the pharmacokinetics of medications in extracorporeal membrane oxygenation.
Introduction
Levetiracetam is a first line option to treat seizures in critically ill patients.1–3 Its clinical efficacy combined with wide therapeutic index, few drug interactions, and favorable safety profile position this medication to be appealing in the intensive care unit (ICU).3,4 Venovenous extracorporeal membrane oxygenation (VV ECMO) is a life-saving intervention for patients requiring advanced respiratory support. The ECMO circuit contributes to a number of pharmacokinetic alterations, and limited data is available regarding levetiracetam in this population. 5 To our knowledge, this is the first case report of levetiracetam in an adult supported on VV ECMO.
Case report
A 40-year-old female (height 162.6 cm, weight 57.2 kg) with systemic lupus erythematosus, seizure disorder, and common variable agammaglobulinemia presented to the hospital with ambulatory dysfunction. Steroids and intravenous immunoglobulin were administered for a lupus flare. She experienced a seizure despite administration of her home regimen levetiracetam 500 mg and 750 mg in the morning and evening, respectively. The dose was increased to 750 mg every 12 h, changed to the intravenous form, and she was escalated to critical care for intubation. Four days later seizures on the electroencephalogram prompted a dose increase to 1500 mg every 12 h and initiation of lacosamide. Over the next 2 weeks, acute respiratory distress syndrome is the primary medical problem, and profound hypoxemia prompted initiation of VV ECMO. She was supported using a Maquet Quadrox oxygenator and Rotaflow centrifugal pump, using one liter of crystalloid to prime the circuit, and initial flow was set to 5 L/min and sweep gas flow was 3 L/min. She was cannulated with a 25 french drainage cannula in the right femoral vein, and a 21 french return cannula in the right internal jugular vein. Two weeks post-cannulation, a clinical seizure prompted increasing levetiracetam to 2000 mg every 12 h. The patient thereafter experienced a complicated hospital course, but not additional seizures. She endured complications including but not limited to recurrent multidrug resistant ventilator associated pneumonia, right ventricular dysfunction, and pneumothoraces, although her renal and liver function remained stable throughout admission. She was denied by several centers for lung transplantation, and after 4 months she was transitioned to comfort care and passed away.
Pharmacokinetics of levetiracetam in a patient supported on venovenous extracorporeal membrane oxygenation.
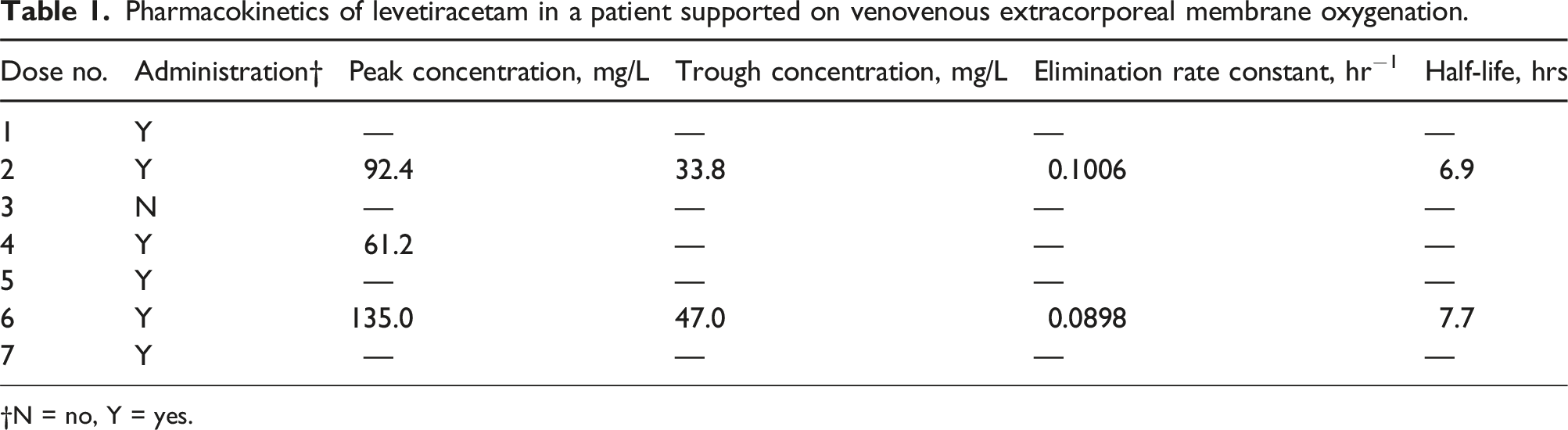
†N = no, Y = yes.
Available peak and trough concentrations indicated an elimination half-life of 6.9-7.7 h (Table 1). Volume of distribution (Vd) was calculated to be 0.58 L/kg and 0.39 L/kg for each set of available peak and trough concentrations, respectively. One-compartment modeling was employed for levetiracetam calculations. 6 During this time in therapy, the patient was euvolemic with a net negative fluid balance. There were two circuit exchanges performed: one 3 days prior to the levetiracetam dose increase to 2000 mg, and the other was 2 weeks later. The patient’s parent provided informed consent for the publication of this case report.
Discussion
This is the first case report describing levetiracetam pharmacokinetics in an adult during VV ECMO. Our patient demonstrated a Vd of 0.39-0.58 L/kg and a half-life of 6.9-7.7 h. In a patient with normal renal function Vd is 0.5-0.7 L/kg, half-life is 6 to 8 h, and the typical dose is 1000-1500 mg every 12 h although higher doses may be necessary in the setting of uncontrolled seizures or status epilepticus.1,3 The patient reported here was titrated up to 2000 mg every 12 h in the setting of uncontrolled seizures and demonstrated pharmacokinetic parameters similar to those in healthy adults. Levetiracetam is a hydrophilic medication with LogP of −0.6. 7 If the ECMO circuit was to impact levetiracetam pharmacokinetics, it would be at highest risk to do so via hemodilution at the initiation of ECMO from introduction of priming solution, increasing Vd thereby decreasing plasma concentration, and potentially leading to a therapeutic failure. 8 ECMO circuit exchange procedures also include introducing a new primed circuit, which also could result in hemodilution with the same rationale as cannulation. The patient reported here did not experience seizures peri-cannulation, did experience a seizure 3 days after her first circuit exchange, and did not experience seizures after her second circuit exchange. The priming solutions offering clinically significant hemodilution for levetiracetam seems to be unlikely given the timing of the observed seizures for this patient.
There is a case report of levetiracetam in veno-arterial (VA) ECMO and continuous venovenous hemofiltration (CVVH) demonstrating a Vd of 0.65 L/kg and half-life of 8.72-10.11 hours. 9 One may have expected the apparent Vd of levetiracetam to markedly increase in the setting of two extracorporeal circuits, volume positivity, and multiorgan dysfunction, however it was similar to healthy volunteers, as is the case with our patient. 6 When comparing the ECMO modalities, loss of pulsatile flow during VA ECMO can result in upregulation of the renin-angiotensin system and significantly alter the regulation of fluid and electrolytes, increasing blood volume and as a result Vd; although this pharmacokinetic difference was not appreciated when comparing this case report to our patient. 10 Additionally, when comparing the serum concentrations of these two cases the VV ECMO concentrations were substantially increased. The authors speculate the lower concentrations observed with CVVH could be attributable to drug removal given the low molecular weight and low protein binding of levetiracetam combined with the hemofiltration rate of 3 L/hr. 5
Comparing this patient’s pharmacokinetic parameters to critically ill adults who were not supported with ECMO should be considered. Levetiracetam pharmacokinetic data in the critically ill is limited to the setting of augmented renal clearance (ARC) in trauma and neurocritical care patients. In these patients Vd is unchanged or increased whereas clearance increases proportionally with creatinine clearance.11–13 Urine creatine was not collected for our patient, so ARC cannot be completely ruled out although her ARC score was 6 indicating ARC is less likely limiting comparison to this population. 14
There is a case report of levetiracetam in a 16-year-old patient supported on VV ECMO demonstrating pharmacokinetic parameters similar to those in healthy pediatric patients. 15 Pediatric patients often have a larger Vd and higher clearance of levetiracetam compared to adults,16,17 so there are limitations to this comparison for our patient.
Levetiracetam is primarily excreted through the kidneys, with 66% recovered in urine and 27% metabolized via enzymatic hydrolysis in the blood. 6 The patient described here had stable kidney function throughout her described ECMO run, so this did not influence dosing. She did have multiple comorbid conditions and received many medications accordingly, yet with levetiracetam metabolism mostly independent of the liver it’s unlikely concomitant medications affected the pharmacokinetics of levetiracetam. However, it is possible the concomitant antiseizure medication, lacosamide, may have offered antiseizure effect in addition to levetiracetam and may be a confounder for efficacy.
Typically, therapeutic drug monitoring is not conducted for levetiracetam as the therapeutic range is wide and adverse events are infrequent. The target trough range for levetiracetam is 12-46 mg/L while peak concentrations frequently aren’t reported.6,18 The patient described here required multiple dose escalations of levetiracetam in addition to a second medication to achieve seizure control. In the setting of VV ECMO support, therapeutic drug monitoring was pursued to ensure adequate serum concentrations were achieved. A major limitation to this case report is hemodilution would take place at the time of cannulation, or as the authors also speculate after a circuit exchange, and pharmacokinetic monitoring was not conducted immediately surrounding these events. Absence of seizures during cannulation and circuit exchanges does not rule out that these changes may have occurred. Despite these limitations the conducted monitoring was a valued opportunity to share the impact, or lack thereof, of VV ECMO on the pharmacokinetics of levetiracetam.
Conclusion
This case of a critically ill adult receiving levetiracetam while supported with VV ECMO demonstrated a comparable apparent Vd and half-life with that observed in healthy volunteers. Pharmacokinetic monitoring of levetiracetam after achieving steady-state is not necessary during ECMO as pharmacokinetic parameters were unchanged.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.