
Abstract
Introduction
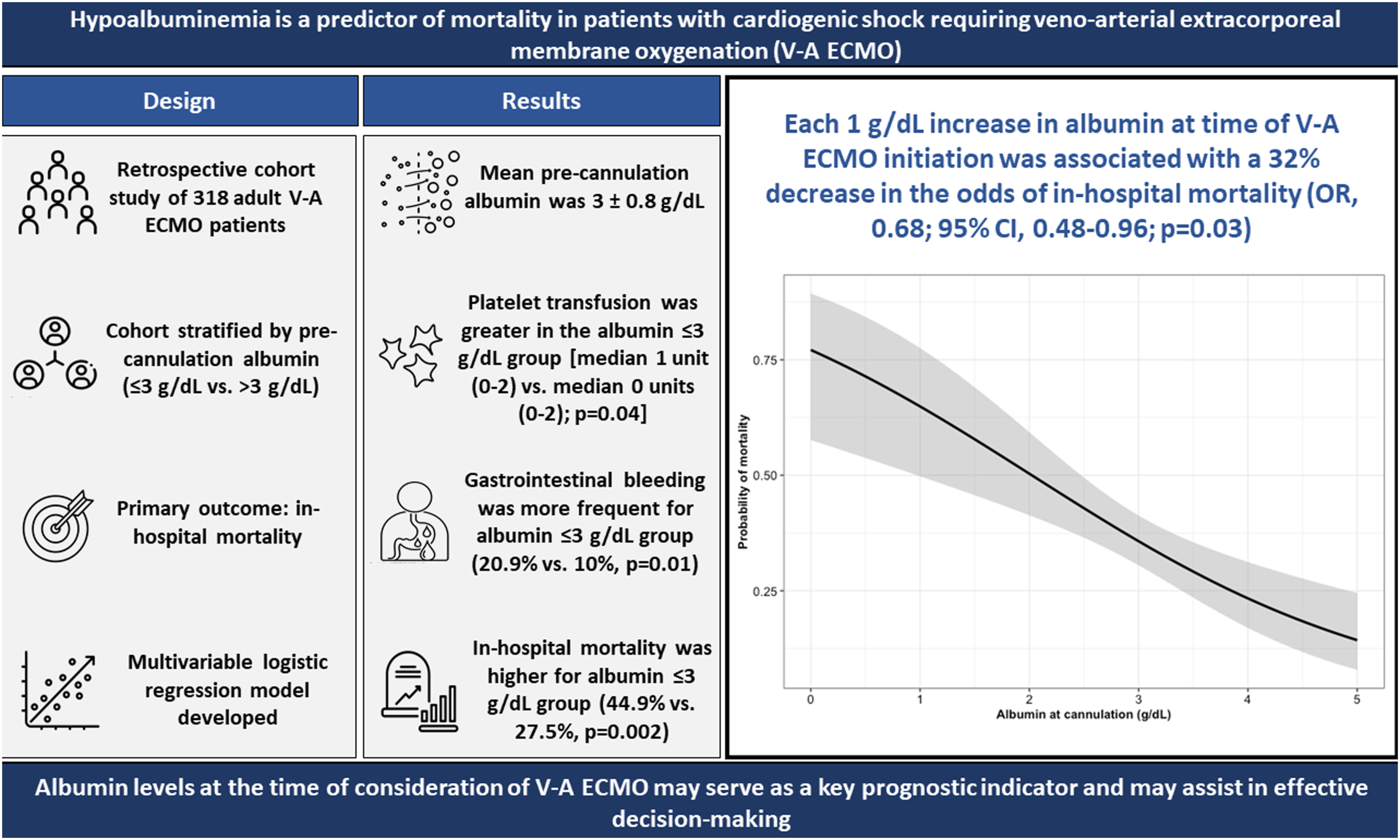
Hypoalbuminemia is predictive of mortality in critically ill patients, especially those with cardiac etiologies of illness. The objective of this study was to determine the association of albumin level pre-cannulation for veno-arterial (V-A) extracorporeal membrane oxygenation (ECMO) and important clinical hospital outcomes.
Methods
This was a retrospective, observational cohort study of albumin levels in patients with cardiogenic shock requiring V-A ECMO between December 2015 and August 2021 in a single, high-volume ECMO center. The primary outcome was in-hospital mortality.
Results
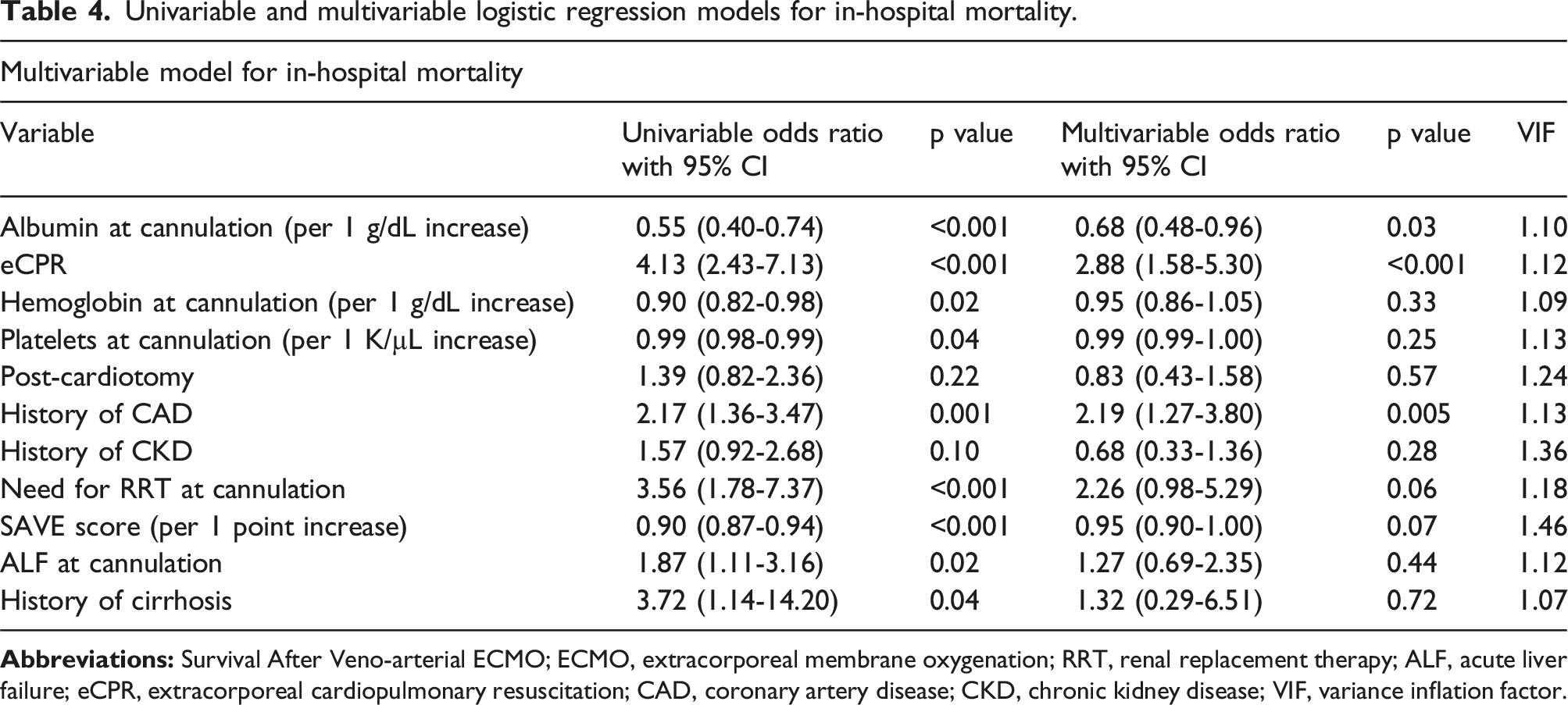
Of 434 patients assessed, 318 were included. The overall mean pre-ECMO albumin was 3 ± 0.8 g/dL and mean albumin at 72 hours post-cannulation was 2.7 ± 0.5 g/dL. For patients with pre-ECMO albumin ≤3 g/dL vs. >3 g/dL, in-hospital mortality was 44.9% vs. 27.5%, respectively (p = .002). In multivariable logistic regression analysis, higher albumin (per 1 g/dL increase) at time of V-A ECMO initiation was associated with decreased odds of in-hospital mortality (OR, 0.68; 95% CI, 0.48-0.96; p = .03). Patients with a pre-ECMO albumin ≤3 g/dL required significantly more platelet transfusions and had higher incidence of gastrointestinal bleeding during V-A ECMO support (both p < .05).
Conclusions
Hypoalbuminemia at time of cannulation is significantly associated with in-hospital mortality and ECMO-related complications including platelet transfusion and gastrointestinal bleeding. Albumin levels at the time of consideration of V-A ECMO may serve as a key prognostic indicator and may assist in effective decision-making regarding this invasive and costly resource.
Keywords
Introduction
In patients with refractory cardiogenic shock, veno-arterial extracorporeal membrane oxygenation (V-A ECMO) can be used to provide circulatory support with a reported survival that ranges from ∼30%–50% depending on indication.1–4 In addition to variability in outcomes, extracorporeal therapies like V-A ECMO are resource intensive and incur risks associated with therapy. 5 Thus, determining which individuals will gain the most potential benefit from V-A ECMO support is of critical importance.
Clinical factors associated with poor outcomes and increased mortality in patients on V-A ECMO include renal insufficiency, advanced age, prolonged time on ECMO, increased duration of mechanical ventilation, pre-ECMO cardiac arrest, low serum bicarbonate, congenital heart disease, decreased pulse pressure, and pre-ECMO INR >1.8.1,3,6,7 To aid with resource allocation and management of V-A ECMO, several of these characteristics have been incorporated into scoring tools developed to predict an individual’s likelihood of survival with V-A ECMO treatment such as SAVE and PREDICT V-A-ECMO scores.1,7 However, these models are imperfect and may perform inconsistently when applied to different populations limiting their current utility. 8 Thus, continued investigation of variables that accurately predict mortality and other important clinical outcomes in V-A ECMO candidates is essential.
As the most abundant plasma protein in vertebrates, albumin is involved in many key biological processes including maintenance of blood colloid osmotic pressure, ion transfer, free radical neutralization, and transport of metabolically active substances. 9 While traditionally used as a marker of nutritional status, numerous medical conditions other than malnutrition can cause hypoalbuminemia including liver disease, heart disease, gastrointestinal disorders, renal disease, infection, inflammatory diseases, and endocrinopathies. Albumin levels are also shown to correlate with disease severity in critically ill populations.10,11 Increased capillary permeability in the setting of inflammation, decreased synthesis, increased catabolism, and hemodilution from resuscitative fluid administration can contribute to development of hypoalbuminemia in both acute and chronic illness.10–13 Notably, hypoalbuminemia has been found to be predictive of morbidity and mortality in patients with a broad range of pathologies such as heart failure, sepsis, renal insufficiency, coronary artery disease, transplantation, and malignancies.11,13–21 While albumin levels are readily available and have significant potential to serve as a prognostic indicator in various clinical scenarios, their association with outcomes in patients on V-A ECMO has not been thoroughly evaluated. 22 This study aims to determine the relationship between pre-cannulation hypoalbuminemia and important clinical events in patients who underwent treatment with V-A ECMO.
Methods
Study population
This retrospective, observational cohort study examined patients at University of Maryland Medical Center who were cannulated for V-A ECMO between December 1st, 2015 and August 1st, 2021. This study was approved by the Institutional Review Board at University of Maryland, Baltimore (HP-00104157). Patients were identified from internal databases of all patients cannulated for ECMO. Data from first ECMO treatment period were included, while subsequent cannulation data were excluded. In the final analysis, patients were included if they were ≥18 years of age, initially cannulated in V-A configuration, and had serum albumin drawn within 24 hours prior to cannulation. Patients were excluded if they were cannulated for veno-venous (V-V) or veno-arterial-venous (V-AV) ECMO during index admission or cannulated at another institution as laboratory and/or clinical data were not readily available in electronic medical record (EMR).
Data collection and definitions
Demographic, comorbidity, laboratory, echocardiographic, ECMO circuit, transfusion, exogenous albumin administration, and clinical outcomes data was retrospectively extracted from EMR. Baseline laboratory data included relevant markers of end-organ perfusion and were only recorded if collected within 6 hours prior to V-A ECMO cannulation. Serum albumin was collected at hospital admission to our institution, within 24 hours prior to cannulation, and at 72 hours post-cannulation. Exogenous albumin administration was documented prior to and for 72 hours following cannulation. Albumin administration was at treating provider direction; our institution does not utilize albumin-specific resuscitation protocols. To estimate baseline illness severity and probability of in-hospital mortality, survival after veno-arterial-ECMO (SAVE) score was calculated using methods previously described. 1
Major bleeding was defined as any overt bleeding that resulted in hemoglobin decrease of ≥2 g/dL, transfusion of ≥2 units packed red blood cells (PRBCs), or need for urgent surgical intervention. Gastrointestinal bleeding (GIB) included any major bleeding event with direct evidence of gastrointestinal source. Minor bleeding included any bleeding that did not meet the criteria for major bleeding, but still required intervention to achieve hemostasis (e.g., cannula site bleeding requiring re-suturing). Intracranial hemorrhage and acute ischemic stroke were defined as any acute change in neurological status lasting for at least 24 hours and was confirmed by neuroimaging. Acute liver failure was defined as total bilirubin ≥10 mg/dL or international normalized ratio (INR) ≥2 in the absence of direct thrombin inhibitors or vitamin K antagonists.
Institutional ECMO practice
The Rotaflow pump (Getinge Group, Wayne, NJ) and Quadrox-I oxygenators (Getinge Group) were the institutional standard during this study period. Typically, V-A ECMO flows were sustained between 3.5-5 L/min and could be adjusted at treating team discretion. Adjustments are often made based on markers of end-organ perfusion and/or myocardial recovery (e.g., lactate, urine output, etc.). Mean arterial pressure goal was maintained ≥65 mmHg for most V-A ECMO patients but could be adjusted based on patient-specific characteristics. Anticoagulation on V-A ECMO is usually unfractionated heparin targeting a goal activated partial thromboplastin time (aPTT) between 60-80 seconds; goals can be altered at clinical team discretion. Direct thrombin inhibitors are used if heparin-induced thrombocytopenia or heparin resistance are suspected.
Statistical analysis
All analyses were performed using R statistical software (version 4.3.1; R Core Team [2022]. R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria). The STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) checklist for cohort studies was referenced during the preparation of this manuscript. The cohort was stratified by serum albumin at the time of cannulation; serum albumin >3 g/dL (high albumin) and serum albumin ≤3 g/dL (low albumin) were selected as the breakpoints based on the distribution of albumin values from our sample. A breakpoint of ≤3 g/dL was chosen to reflect presence of moderate to severe hypoalbuminemia. 23 Sample size was determined pragmatically and based on the number of patients cannulated for V-A ECMO during the study period; however, our sample size of 318 patients would provide sufficient power (two-sided α = 0.05 and β = 0.20) to detect an absolute difference of 15.2% for in-hospital mortality between the low and high albumin groups.
Categorical variables are reported as number and percentage. A Pearson chi-square test or Fisher’s exact test was used to compare categorical data; the Fisher’s exact test was used for small cell counts (n<10). Normality was assessed for all continuous data via direct visualization of histograms and with assistance of the Shapiro-Wilk test. Parametric continuous data is expressed as mean ± standard deviation; nonparametric continuous data is reported as median (25th-75th percentile). Difference in means for parametric continuous data was compared using an independent samples t-test. Nonparametric data was analyzed using the Wilcoxon rank-sum test. A two-sided p-value <.05 was considered statistically significant for all analyses.
Univariable logistic regression was used to identify the crude association of serum albumin at time of cannulation with in-hospital mortality; albumin was modeled as a continuous variable. Subsequently, the association of other relevant baseline covariates at the time of ECMO cannulation with in-hospital mortality was assessed to assist in the detection of potential confounders. These baseline covariates were selected based on either prior data demonstrating a direct association with in-hospital mortality during extracorporeal support or if there was a theoretical clinical association with in-hospital mortality.
To fully explore the relationship of serum albumin at cannulation with in-hospital mortality, a multivariable logistic regression model was developed with in-hospital mortality set as the dependent variable. Independent variables were selected for inclusion in this final multivariable model if there was clinical plausibility for confounding or if univariable analysis demonstrated potential association with in-hospital mortality (p-value <.20 in univariable analysis). All covariates identified as potential confounders were forced into a large multivariable logistic regression model; backward stepwise elimination was implemented, removing the least significant variables one-by-one. Several non-significant covariates were retained in the final multivariable model due to clinical suspicion of confounding. Ultimately, eleven covariates were included in the final model: albumin at cannulation, eCPR status, hemoglobin at cannulation, platelet count at cannulation, post-cardiotomy status, history of coronary artery disease, history of chronic kidney disease, need for renal replacement therapy at cannulation, SAVE score, acute liver failure at cannulation, and history of cirrhosis. The 10-15 events per covariate concept was used in the development of the final multivariable model in an effort to avoid overfitting and introduction of bias via a low number of events per covariate. 24 Odds ratios (OR) and 95% confidence intervals (CI) are reported for each covariate in both the univariable and multivariable analyses.
Multiple imputation was not required for this analysis as the percentage of missing data was negligible. Multicollinearity in the multivariable model was assessed using correlation matrices and variance inflation factors (VIF) from the car package. Inclusion of covariates with high correlation (R2 > 0.8) or high VIF (>5) was avoided. Model discrimination was assessed using the rms package. After building the final multivariable logistic regression model, a marginal effects plot was developed using the ggeffects package to aid in the visualization of albumin’s predicted association with in-hospital mortality across the spectrum of albumin values at time of ECMO cannulation. To produce this plot, all other covariates within the model are held constant (e.g., continuous covariates within the model are set to their mean values and categorical covariates are set to their reference values).
In an effort to avoid multicollinearity, reduce optimism bias, and automate covariate selection, we performed a post hoc sensitivity analysis using Least Absolute Shrinkage and Selection Operator (LASSO) regression via the glmnet package. LASSO regression imposes a penalty on model parameters, effectively shrinking regression coefficients towards zero. Only the most pertinent covariates are maintained in the final sparse model. The goal of this sensitivity analysis was to ensure that albumin at cannulation was selected as a pertinent covariate and to report its penalized LASSO coefficient and subsequent odds ratio.
Results
Baseline characteristics.
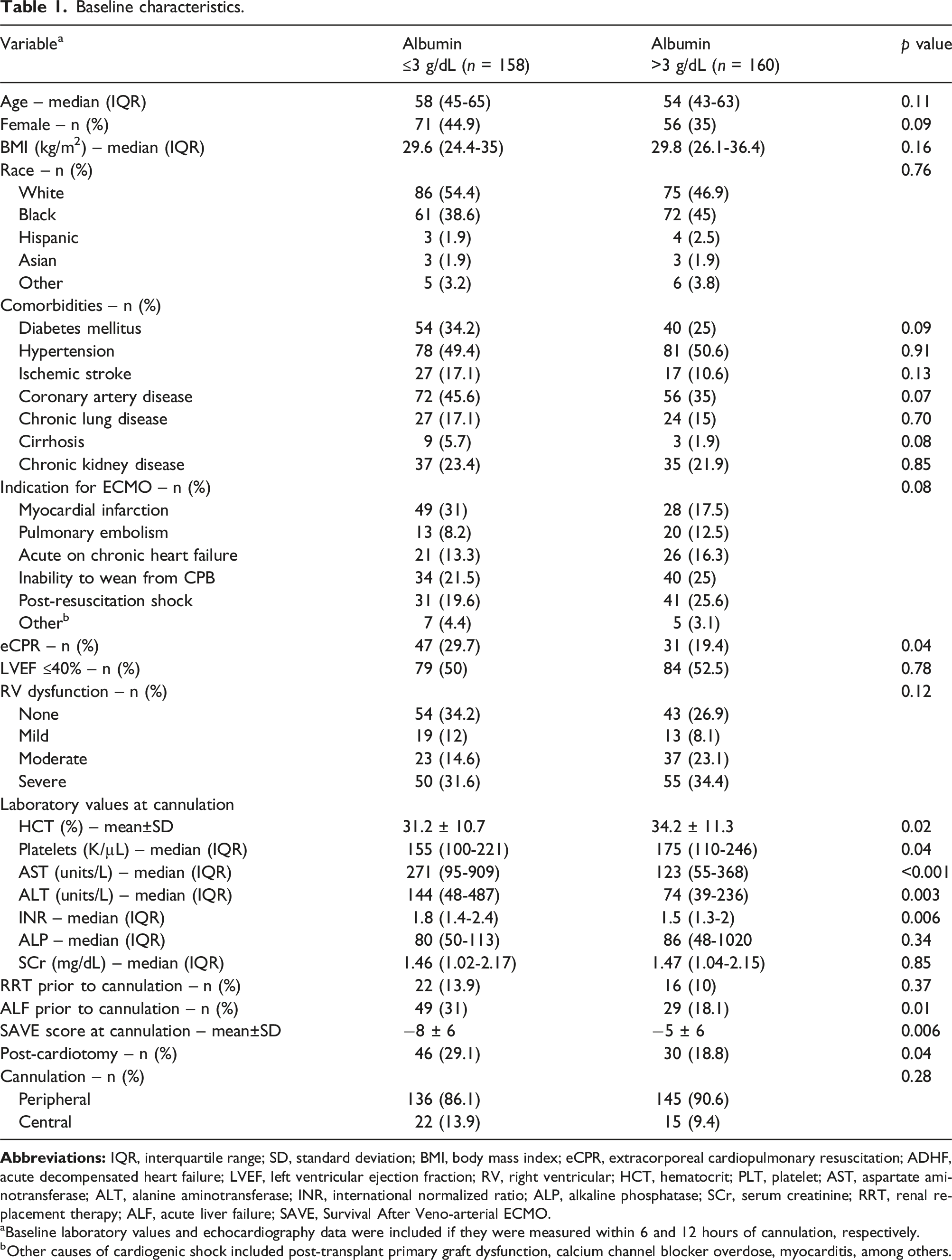
aBaseline laboratory values and echocardiography data were included if they were measured within 6 and 12 hours of cannulation, respectively.
bOther causes of cardiogenic shock included post-transplant primary graft dysfunction, calcium channel blocker overdose, myocarditis, among others.
Briefly, patients in the low albumin group were more likely to undergo extracorporeal cardiopulmonary resuscitation (eCPR), had lower baseline SAVE scores (higher predicted mortality), were more likely to meet criteria for acute liver failure (ALF) at cannulation, were more likely to have received cardiotomy pre-ECMO, had lower hematocrit and platelet counts at cannulation, had higher transaminases prior to ECMO, and had higher international normalized ratio (INR) at cannulation compared to the high albumin cohort.
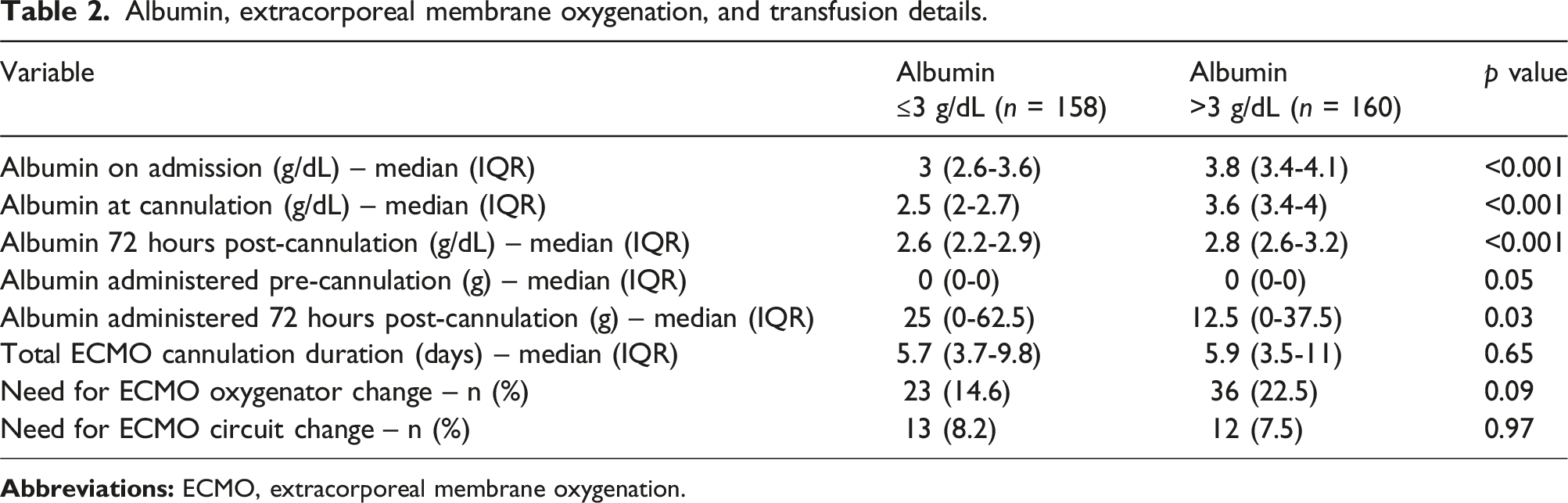
Albumin, extracorporeal membrane oxygenation, and transfusion details.
Clinical outcomes.
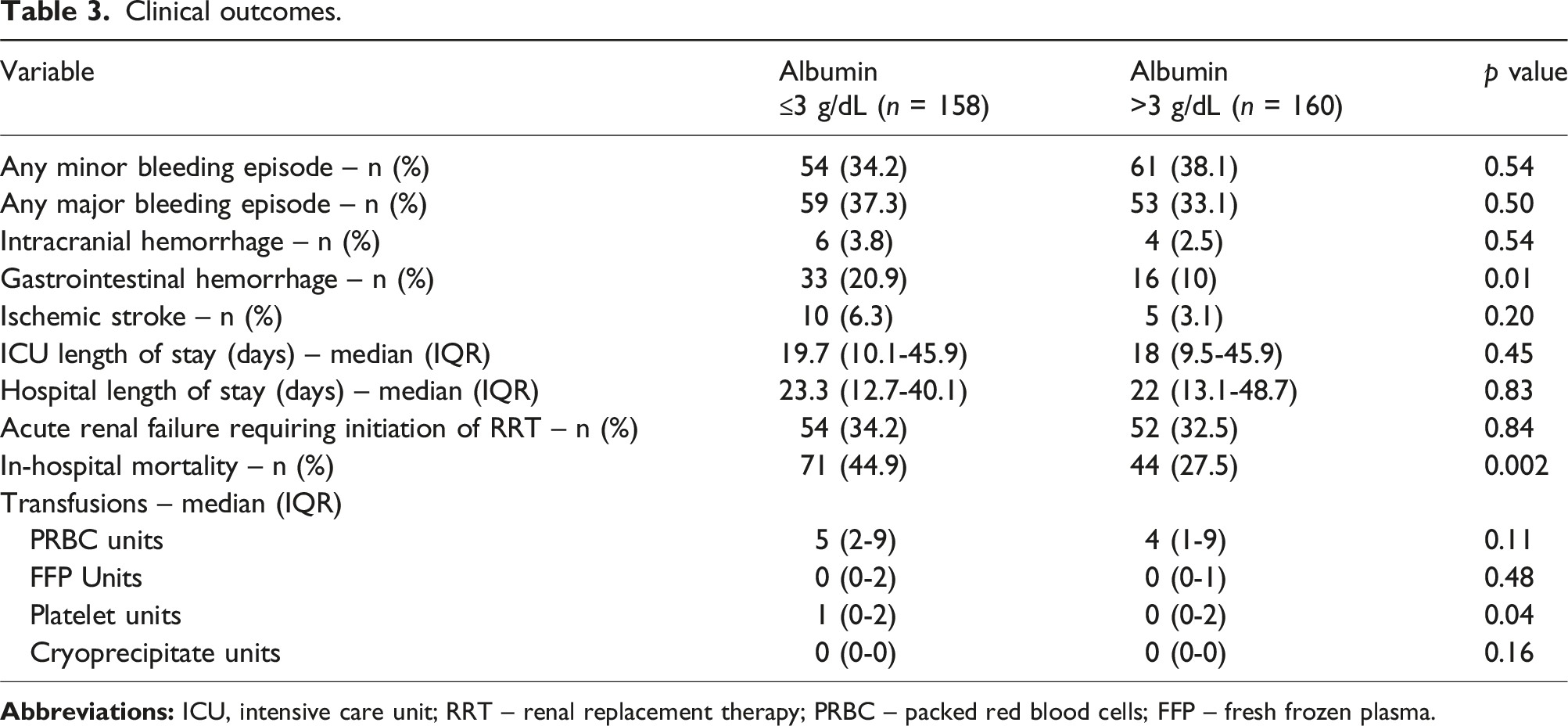
Patients in the low albumin group were more likely to receive transfusion of platelets. In-hospital mortality was significantly higher in the low albumin group compared to the high albumin group (44.9% vs. 27.5%, p = .002). GIB was also more common in the low albumin group (20.9% vs. 10%, p = .01); however, there were no other significant differences among the two albumin groups for the remaining clinical outcomes of interest.
Univariable and multivariable logistic regression models for in-hospital mortality.
Lastly, a post hoc sensitivity analysis using LASSO regression was performed. The minimum mean squared error was achieved when the penalty, λ, was set to 0.03583324. The subsequent LASSO model automatically selected albumin at cannulation, ECMO indication, eCPR status, coronary artery disease history, serum creatinine at cannulation, need for RRT at cannulation, and SAVE score as pertinent covariates. The regularized odds ratio for albumin at cannulation was 0.77. Marginal effects plot of in-hospital mortality across the spectrum of serum albumin concentrations at cannulation.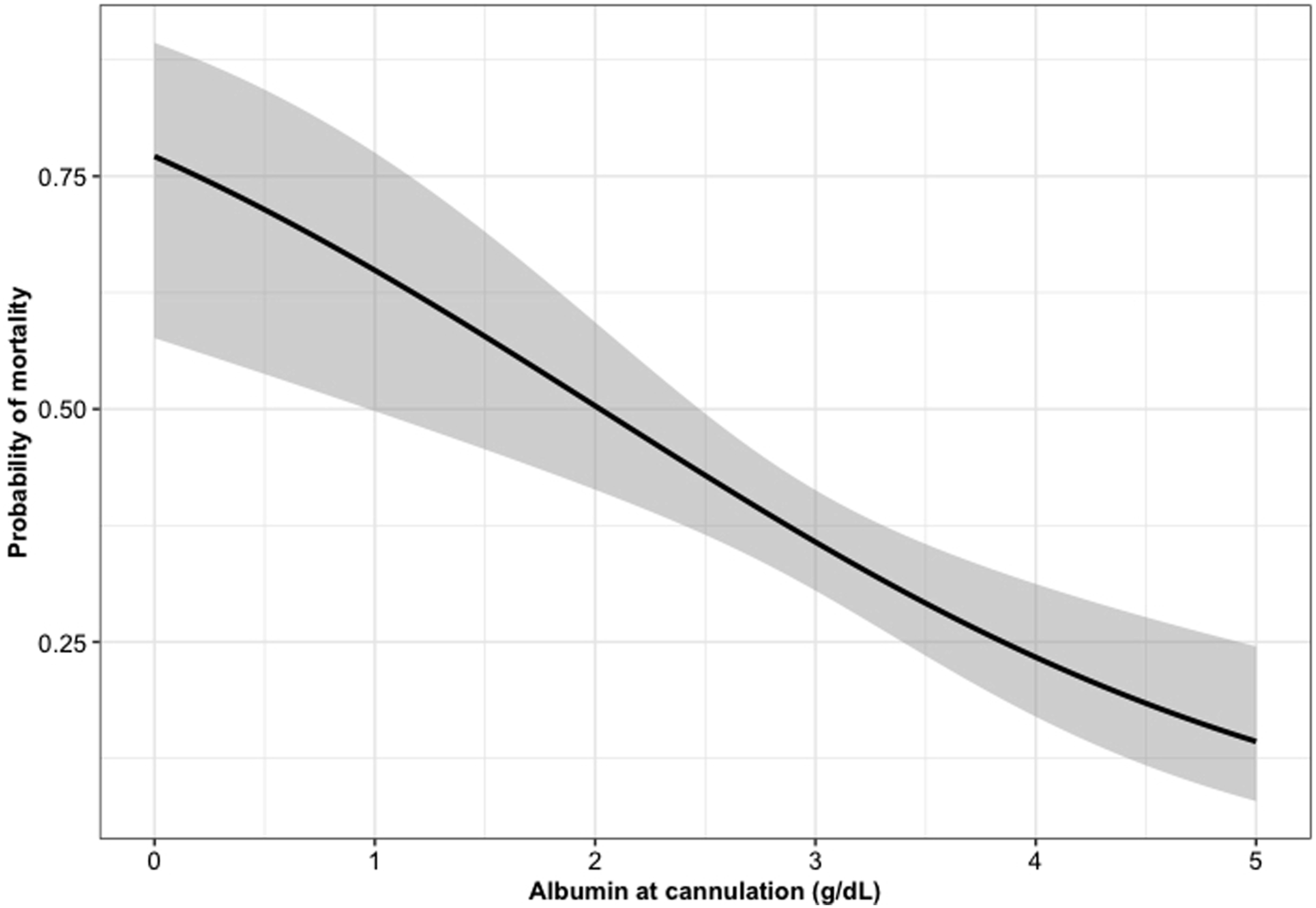
Discussion
In an observational cohort study of 318 patients in a single center, we found that higher pre-ECMO albumin levels were independently associated with decreased odds of in-hospital mortality in individuals placed on V-A ECMO. Patients who received VA-ECMO therapy with albumin levels ≤3 g/dL had the highest in-hospital mortality rate and each 1 g/dL incremental elevation of albumin value at cannulation was associated with a striking 32% increase in hospital survival. We also found an association with the occurrence of complications of V-A ECMO support and serum albumin level including GIB and platelet transfusion. While our findings of a strong correlation with hypoalbuminemia and poor outcomes are consistent with previous studies of critically ill populations, this is the largest report, to our knowledge, to investigate the association of important hospital outcomes and albumin in a cohort of individuals placed on V-A ECMO for a range of indications.11,13,22
Advanced critical illness and therapeutic risks associated with ECMO underlie many of complications and morbidities experienced by those requiring mechanical support. The association of hypoalbuminemia and outcomes for those undergoing V-A ECMO had a strong relationship with not just in-hospital mortality, but also with ECMO-associated complications such as GIB (20.9% vs. 10% in those with albumin ≤3 g/dL and >3 g/dL, respectively). Interestingly, a correlation with low albumin levels and increased non-variceal gastrointestinal hemorrhage has been reported in non-ECMO cohorts.25,26 Although the reasoning behind the correlation of hypoalbuminemia and increased GIB is unknown, it is possible that the strong associations of low albumin with malnutrition, inflammation, and illness severity align it with critical determinants of mucosal integrity. 26 In addition, decline in albumin levels secondary to liver dysfunction may also occur with concomitant coagulation system dysregulation attributed to the hepatic derivation of albumin and many clotting factors. 27 As seen in our cohort, acute liver injury was prominent in those with hypoalbuminemia (31% vs. 18.1%) at cannulation, which may have been accompanied by a coagulopathy that increased risk of GIB. However, we did not find a significant baseline difference in the median platelet values, presence of acute liver failure or INR values in the group of V-A ECMO patients that experienced gastrointestinal hemorrhage and the group that did not (data not shown).
While transfusion is commonplace in V-A ECMO therapy, those with hypoalbuminemia were found to have an increased need for platelet administration that is likely multifactorial. In our cohort, the pre-ECMO albumin ≤3 g/dL group had lower baseline platelet levels, which was not surprising given that both hypoalbuminemia and thrombocytopenia correlate with illness severity. Furthermore, those with hypoalbuminemia also had higher incidence of acute liver failure at cannulation, which can contribute to thrombocytopenia. 28 Platelet transfusion goals for ECMO patients are not protocolized at our institution and variability exists, yet the targets are usually similar: around 30 K/µL for most ECMO patients and 50 K/µL or higher when bleeding is present. Given increased thrombocytopenia at cannulation found in those with hypoalbuminemia in our cohort, it is likely that additional platelet administration was required to meet clinical transfusion goals in these patients. While there was no major difference in overall major or minor bleeding episodes, there was increased incidence of GIB in those with hypoalbuminemia, which may have contributed to institution of higher transfusion goals for prolonged time periods in this subset.
An additional report is available describing the association of hypoalbuminemia and increased 30-day mortality in a smaller cohort of 114 V-A ECMO patients at a center in South Korea. These results are concordant with our finding of decreased in-hospital survival in those with lower pre-cannulation albumin levels. 22 We similarly found that higher volumes of albumin were more likely to be infused in patients with baseline hypoalbuminemia. However, there were several notable differences between the two studies. The relationship between albumin and additional clinical outcomes were not assessed by Jeon et al. as it was in our report. Our study also included patients placed on V-A ECMO for all indications, whereas post-cardiotomy, septic shock and undifferentiated shock etiologies were excluded from the South Korean cohort. Furthermore, the chosen primary endpoint of 30-day mortality subjected the investigation to a degree of loss to follow-up introducing potential selection bias, which is not the case with an in-hospital mortality endpoint. 22
ECMO is an invasive and costly resource necessitating great efforts to ensure its utilization in those who are most likely to benefit without undue risk. While prognostic scores to assess outcomes of individuals being considered for V-A ECMO such as the SAVE score have been proposed and validated, performance can be imperfect in different populations. 8 This can lead to erroneous decision-making regarding candidacy and the potential exclusion of individuals who might otherwise survive with extracorporeal support. In our cohort, both SAVE score and pre-ECMO serum albumin levels were independently associated with mortality via multivariable logistic regression analysis. Thus, the addition of albumin, an inexpensive and widely available value, may enhance predictive models of mortality like the SAVE score if incorporated. Surprisingly, leading outcome prediction models in critically ill ECMO and non-ECMO populations do not currently include albumin levels.1,7,29 While the hypoalbuminemia that is observed in patients requiring VA-ECMO initiation is likely multifactorial, its severity at the time of cannulation is a probable reflection of the extent of critical illness. This likely underlies the strong potential of albumin level to serve as a significant indicator of survival with extracorporeal therapy. The incorporation of albumin in established ECMO survival prediction models, ideally after further validation in additional cohorts, warrants investigation to delineate added value.
Limitations of this study include that it was performed at a single, high volume ECMO center and results from this patient group are likely not generalizable to all V-A ECMO patients as extracorporeal protocols, approach to care, and patient demographics will vary, limiting the external validity of our findings. While a causal relationship between hypoalbuminemia and in-hospital mortality cannot be established using analysis of this single cohort, our study highlights the need for further investigation into the role of albumin as a prognostic biomarker in patients with cardiovascular compromise requiring V-A ECMO. Given the retrospective nature, this study design is prone to confounding. While we attempted to control for relevant covariates associated with extracorporeal in-hospital mortality, residual confounding may exist. Importantly, many variables known to be associated with mortality in patients on V-A ECMO are already incorporated into the calculation of the SAVE score, which was included in our multivariable logistic regression analysis. 8 Our multivariable logistic regression model may have been prone to multicollinearity; however, we demonstrated that the final covariates included in the model had low VIF and post hoc sensitivity analysis using LASSO regression selected albumin at cannulation as a pertinent covariate to be considered for in-hospital mortality. Lastly, a proportion of screened patients were excluded for missing pre-cannulation albumin values (n = 72). Given the study design, it is challenging to retrospectively determine the reason for this missing data. However, albumin is part of a routine metabolic panel so one can postulate that it is likely that these patients required urgent cannulation. These missing samples may have biased our findings; however, these 72 patients had wide variation in their etiologies of cardiogenic shock and severity of illness, which was likely already represented well by this large, heterogenous V-A ECMO cohort.
In summary, our study demonstrates that albumin levels, a readily available value at time of cannulation, may be an independent predictor of in-hospital mortality in patients receiving V-A ECMO therapy. In our cohort, hypoalbuminemia was also found to be associated with important ECMO-related complications including GIB and platelet transfusion. As a likely indicator of the extent of overall critical illness, albumin levels may serve as an important prognostic tool that can be used to help guide clinical V-A ECMO decision-making and to optimize equitable utilization of this important resource. Further research in large, diverse, multicenter ECMO populations is needed to better determine the exact relationship between hypoalbuminemia and outcomes in those being considered for V-A ECMO therapy and to identify any causal effect of albumin on these important clinical events.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.