
Abstract
Coarctation of the aorta (CoA) is a congenital heart disease (CHD) that may remain undiagnosed until adulthood. Its clinical manifestations vary depending on the anatomical severity of the narrowing and the degree of collateral circulation development. The management of CoA, particularly when associated with additional CHDs or acquired cardiovascular pathology in adult patients, necessitates a comprehensive and individualised treatment strategy. We present a clinical case of a 33-year-old female diagnosed with CoA, complicated by an aortic root aneurysm and bicuspid aortic valve (BAV) insufficiency. Given the complexity of her condition, a staged hybrid approach was implemented. In the first stage, the patient underwent surgical valve-sparing aortic root replacement (David procedure), preserving the native valve function. Three weeks later, thoracic endovascular aortic repair (TEVAR) was performed to address the CoA. The patient’s postoperative recovery was uneventful. Follow-up imaging, including computed tomography angiography (СТА) and transthoracic echocardiography at 3 months post-discharge, demonstrated an optimal surgical outcome, confirming the efficacy of this tailored two-stage strategy.
Keywords
Introduction
Bicuspid aortic valve is the most prevalent CHD occurring in approximately 1%–2% of the population. It is commonly associated with coarctation of the aorta (CoA). An estimated 85% of CoA cases also present with a bicuspid aortic valve (BAV), while the remaining cases are linked to other congenital cardiac anomalies. 1 Emerging data suggest that the coexistence of BAV and CoA significantly contributes to aortic pathology, particularly aortic dilation, more frequently than isolated forms of either condition. 1 Patients with BAV often develop progressive valvular dysfunction, including stenosis and regurgitation, which predisposes patients to aortic root and ascending aortic dilation. 2
The combination of CoA, aortic root aneurysm, and BAV is relatively rare in adult patients, presenting unique challenges for surgical management. Currently, no standardised surgical guidelines exist for this subset of patients, and treatment strategies depend largely on anatomical variations, patient-specific haemodynamic considerations, and the expertise of the surgical team. Undiagnosed adult patients with CoA often present with poorly controlled arterial hypertension, which exacerbates the progression of aortic dilation and valve dysfunction. Various surgical and hybrid approaches have been described in the literature, including single-stage and staged interventions for addressing CoA in conjunction with aortic valve disease or an aortic root aneurysm.3,4
In this report, we present a case of a 33-year-old female patient with CoA, BAV with severe regurgitation, and an aortic root aneurysm who underwent a two-stage hybrid approach. The first stage involved a valve-sparing aortic root replacement (David procedure) followed by endovascular aortic coarctation stenting (TEVAR) in the second stage. This approach was selected to optimise the surgical outcome and mitigate the intraoperative risks.
Case report
A 33-year-old female patient was admitted to our clinic with complaints of palpitations, chest discomfort, uncontrolled arterial hypertension and blood pressure readings reaching 180/100 mmHg. Her CHD was initially diagnosed at the age of 18 during a routine examination conducted as part of her prenatal care. Despite a recommendation for surgical intervention postpartum, the patient declined surgery and remained under regular cardiology follow-up. Over the previous month, her symptoms had worsened, prompting a consultation with our cardiothoracic surgical team and subsequent hospitalisation for further evaluation and treatment.
Her heart sounds were clear on physical examination, though a systolic murmur was auscultated along the left sternal border. Her blood pressure measurements revealed asymmetry: the left upper limb was 150/90 mmHg, the right upper limb was 135/87 mmHg, and the left lower limb was 120/90 mmHg. The patient’s physical development was consistent with her age. However, the bilateral femoral artery pulsation was diminished, suggesting haemodynamically significant aortic coarctation.
Transthoracic echocardiography demonstrated a type 1 BAV with severe regurgitation (grade III) and significant aortic root dilatation (41 mm), sinotubular junction (38 mm), and aortic annulus (34 mm), with concomitant ascending aortic dilation (46 mm). The left ventricular ejection fraction (LVEF) was preserved at 60%. Computed tomography angiography (CTA) confirmed the aortic coarctation, with a narrowing of 2–6 mm in diameter (Figure 1), an aortic arch measuring 22 mm, and a descending aorta measuring 16 mm. Computed tomography angiography demonstrated anatomy of coarctation segment and extensive internal thoracic artery.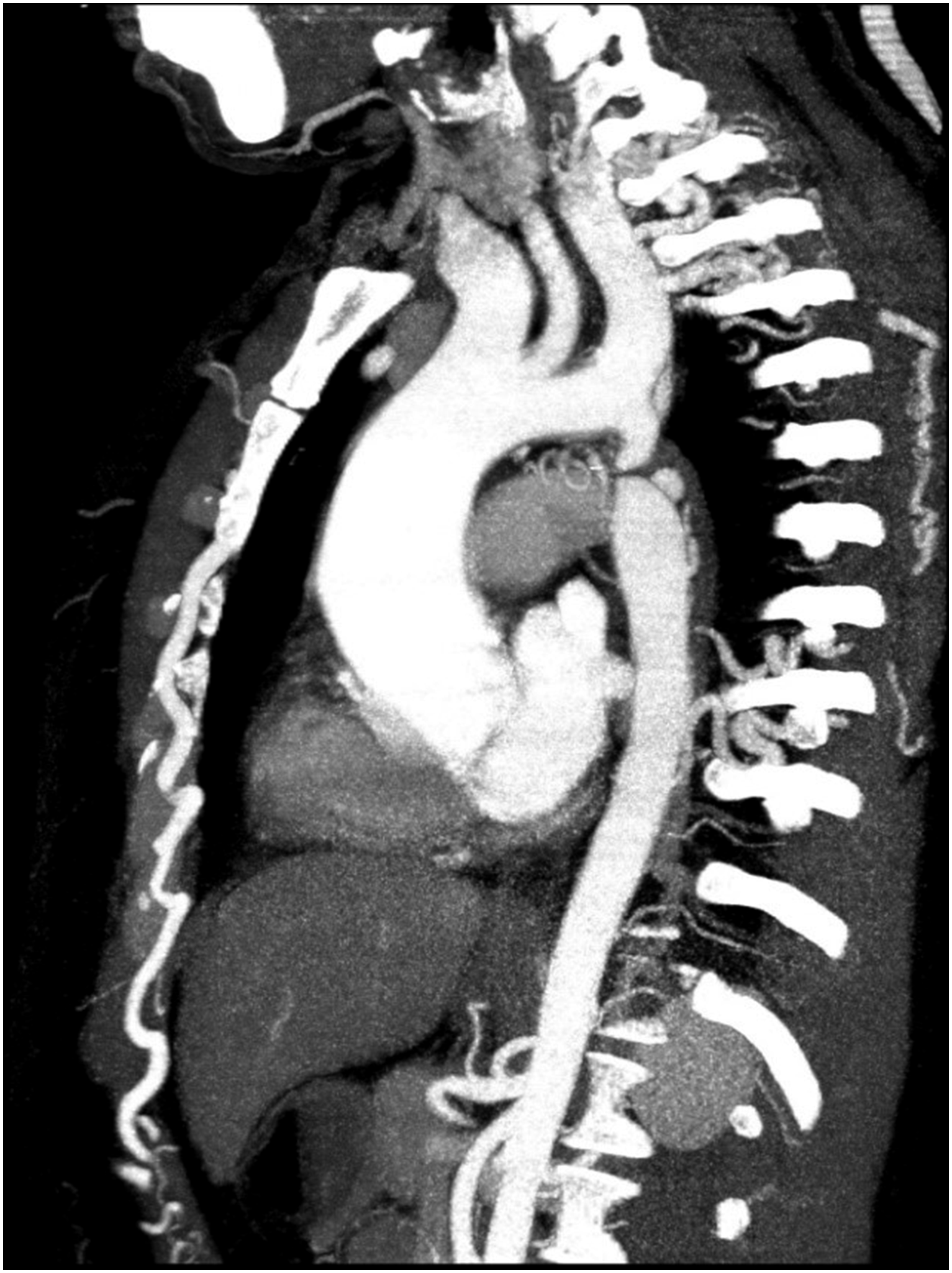
The first stage involved a valve-sparing aortic root replacement (David procedure). The surgery was performed using a standard technique, with the fibrous ring reinforced by interrupted U-shaped sutures along the basal ring. The native aortic valve was reimplanted within a synthetic polyethylene terephthalate vascular graft (28 mm diameter), which was secured using U-shaped sutures. The commissures and valve cusps were anatomically repositioned and affixed to the prosthetic wall. Plication of the right and non-coronary cusps was performed to enhance coaptation. The sinus geometry was preserved within the graft to maintain the natural haemodynamics. The coronary arteries were reimplanted in positions that ensured optimal physiological perfusion. A distal anastomosis was created between the graft and the native aorta using continuous over-and-over sutures. Intraoperative transoesophageal echocardiography confirmed the absence of residual aortic regurgitation.
Originally, a one-stage correction of the CHD was considered. However, extensive collateralisation of the arteries around the descending aorta during surgery complicated the clamping and exposure. Due to the increased risk of haemorrhage and prolonged cardiopulmonary bypass time, the aortic coarctation correction was postponed for a subsequent procedure.
Three weeks later, the patient underwent TEVAR for the aortic coarctation. Bilateral arterial punctures were performed via the right radial and common femoral arteries. Aortography confirmed coarctation with a stenotic segment measuring 4.8 mm, an aortic arch diameter of 13.4 mm, a pre-coarctation aorta diameter of 10.57 mm, and a post-coarctation aorta diameter of 13 mm. The systolic pressure gradient was 120/56–77 mmHg before the stenosis and 53/37–42 mmHg distally, yielding a pressure gradient of 67 mmHg. Antegrade recanalisation of the stenotic segment was successfully achieved, followed by balloon dilation. A Covered CP Stent™ (39 mm) was mounted on a Z-Med II 14/40 balloon and delivered via a Cook 14 Fr introducer sheath. The stent was deployed precisely within the descending aorta, with controlled expansion using balloon inflation. The final positioning ensured optimal correction of the stenotic segment, as confirmed by angiography (Figure 2). The post-procedural invasive pressure gradient measurements demonstrated a reduction in the systolic pressure gradient from 96/40–58 mmHg pre-stenting to 76/34–48 mmHg post-stenting, resulting in a residual gradient of 20 mmHg, indicative of successful revascularisation. Completion angiogram after stent implantation.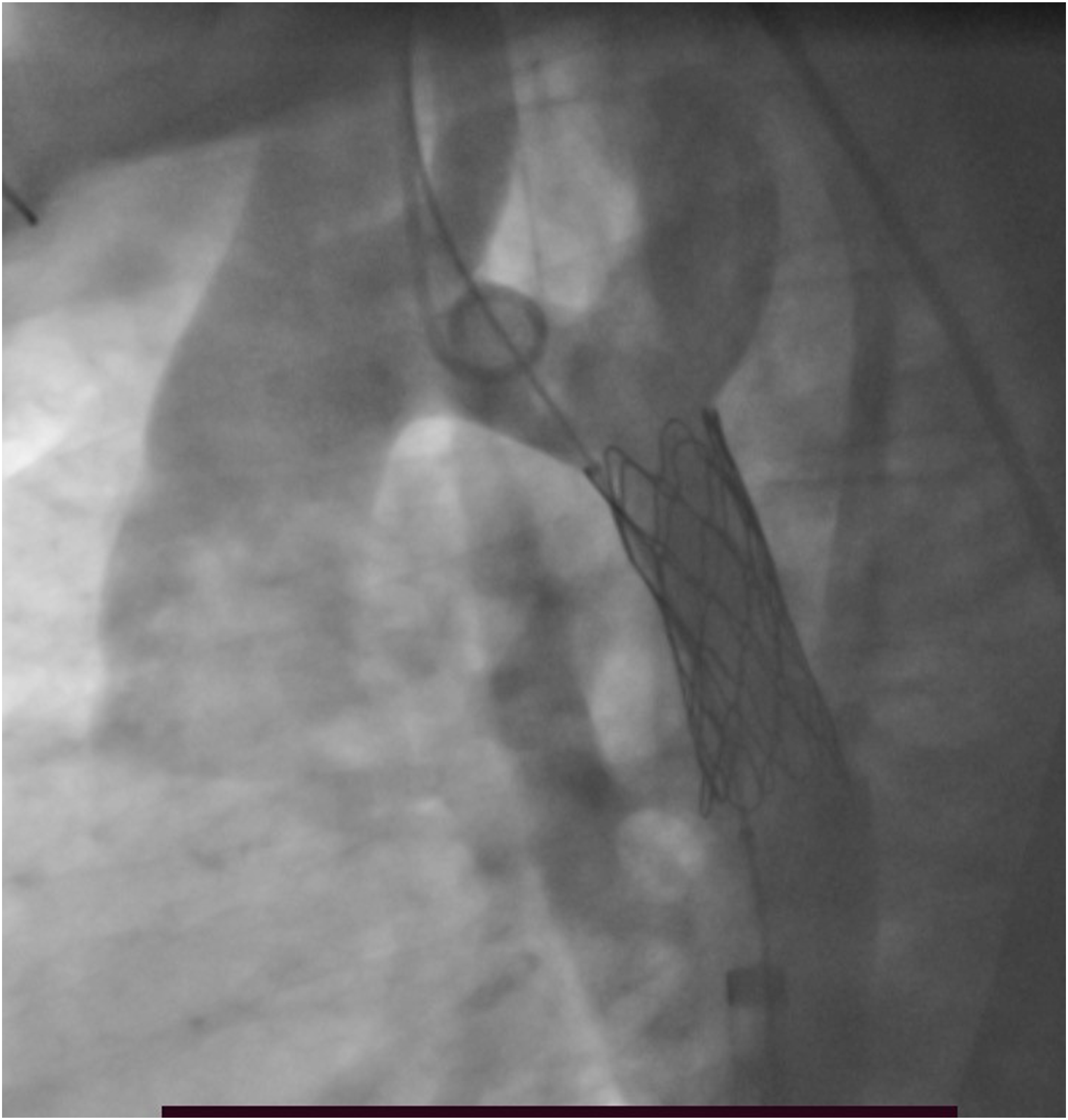
At the 3-month follow-up (Figure 3), CTA confirmed full patency of the stent graft in the aortic isthmus, with final dimensions measuring 38 × 15 mm. Aortic root measurements had significantly improved: the aortic root diameter was reduced to 31 mm, sinotubular junction to 28 mm, ascending aorta to 27 mm, aortic arch to 17 mm, and the descending aorta to 18 mm. Transthoracic echocardiography showed the absence of aortic valve regurgitation, unrestricted leaflet motion, and a transvalvular pressure gradient of 13 mmHg. The LVEF had increased to 68%, reflecting improved cardiac function post-repair. Control computed tomographic angiography 3 month after repair of coarctation.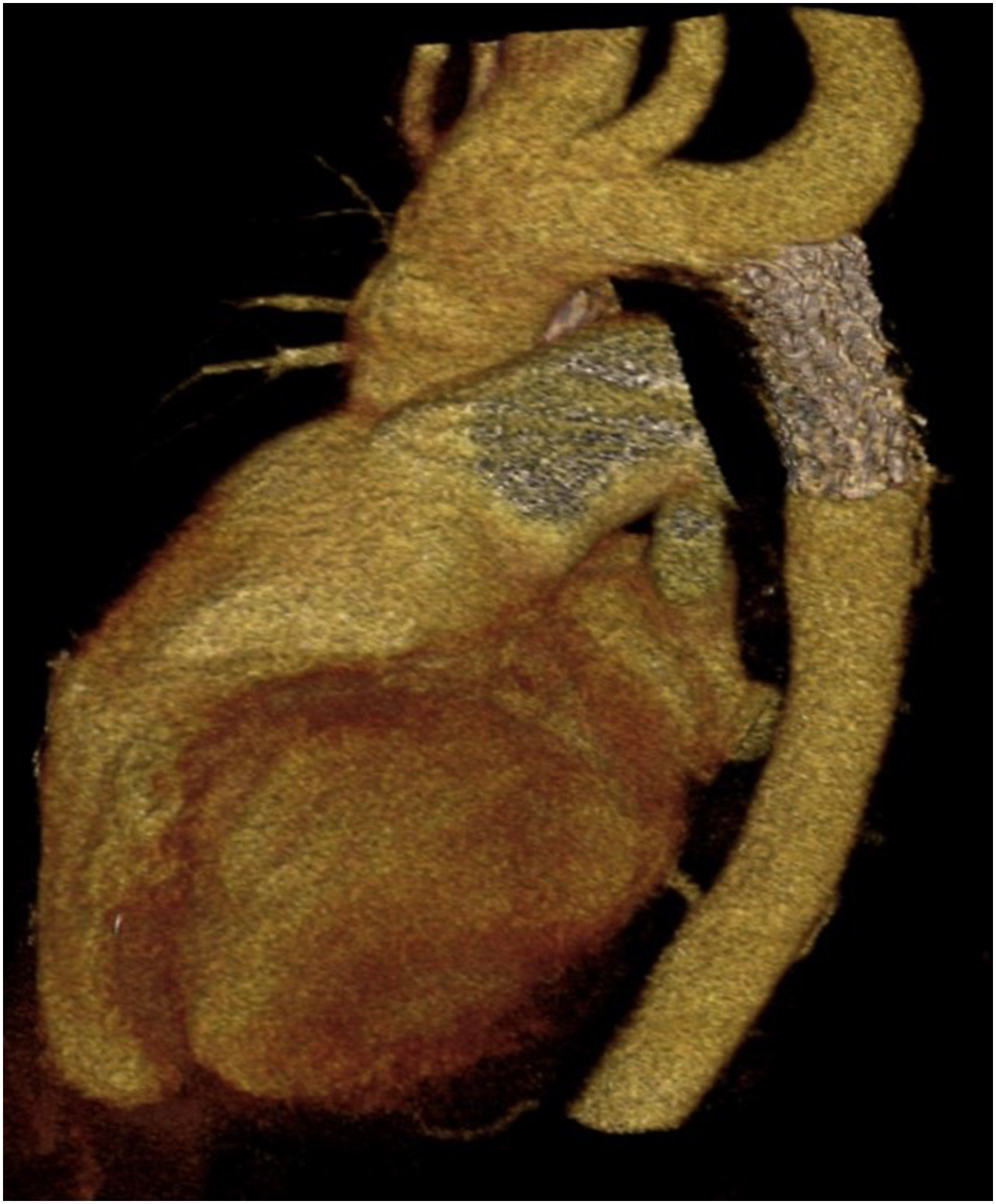
Discussion
As highlighted by Sievers and Schmidtke, 5 the coexistence of CoA and BAV is strongly associated with progressive dilation of the aortic root and ascending aorta, particularly in cases where type 1 BAV presents with fusion of the left and right coronary cusps. This anatomical variation increases the afterload on the left ventricle, contributing to aneurysm formation and further haemodynamic complications.
Historically, CoA was treated exclusively through surgical intervention until the advent of balloon angioplasty in 1982. While this less invasive technique provided an alternative, complications such as re-coarctation, aneurysm formation, and aortic dissection remained concerns for both surgical and percutaneous approaches. Endovascular stenting was introduced in 1990 to address these challenges, emerging as an effective alternative for treating both congenital and recurrent CoA.6–8
In cases of severe aortic valve stenosis, valve replacement is the standard approach. However, when significant aortic regurgitation is present, the decision to perform a valve-sparing repair depends on the anatomical integrity and functional status of the aortic valve. With advancements in reconstructive valve surgery, the David procedure has gained recognition as an optimal method for aortic root replacement while preserving the native aortic valve, particularly in cases involving BAV.9,10
Currently, TEVAR, benefiting from advancements in interventional cardiology, is the preferred treatment for CoA, provided the anatomical morphology of the coarctation is favourable.11–13 However, in the present case, computed tomography imaging of the aortic coarctation raised concerns regarding the potential presence of an interrupted aortic arch. Initially, a single-stage approach was planned. This involved the David procedure with valve-sparing aortic root replacement and radical correction of CoA through resection of the coarctated segment with an end-to-end anastomosis, a method well-documented in the literature.14–17
During the intraoperative assessment, extensive collateral arteries were observed surrounding the descending aorta, complicating the clamping and surgical access. Given the high risk of intraoperative bleeding and prolonged cardiopulmonary bypass time, an intraoperative decision was made to defer the CoA correction to a subsequent procedure. Consequently, a hybrid two-stage approach was adopted, consisting of the David procedure followed by TEVAR.
It is noteworthy that, under ideal circumstances, the logical sequence of a two-stage approach would be first to prioritise TEVAR, thereby reducing the left ventricular afterload and allowing for the observation of the aortic size dynamics and valve function over time. However, in this case, the intraoperative considerations necessitated prioritising the primary correction of the aortic root, valve, and ascending aorta. Three weeks later, the patient underwent the second stage, during which aortography revealed extensive collateral circulation between the brachiocephalic arteries and the descending aorta. This observation validated the intraoperative decision to delay CoA correction, as it clarified why the patient exhibited no severe symptoms aside from uncontrolled hypertension and had developed normally for her age.
A 39-mm Covered CP Stent was subsequently deployed at the coarctation site. The presence of extensive collateral arteries in both surgical and angiographic evaluations is a well-recognised physiological adaptation to aortic coarctation. The body compensates for the narrowed aortic segment by forming alternate pathways for blood flow, often allowing patients with CoA to reach adulthood without significant symptoms. The development of these collaterals likely masked the severity of the condition until adulthood, further complicating the initially planned single-stage approach.
Following TEVAR, there was no immediate reassessment of the collateral circulation. However, it is well established that successful CoA stenting typically leads to regression of the collateral vessels over time. The long-term impact of these vessels, including the potential remodelling after intervention, remains an area requiring further research and long-term clinical monitoring.
Some studies suggest that the initial correction of CoA does not always resolve persistent hypertension, which can contribute to ongoing or worsening aortic dilation. Therefore, in cases where BAV with CoA is accompanied by an aortic root aneurysm and ascending aortic dilation, a staged approach with the David procedure followed by CoA correction represents a reasonable and effective treatment strategy.18–20
This case underscores the importance of individualised surgical planning in complex congenital heart disease. The hybrid two-stage approach provided an optimal outcome, balancing surgical complexity, haemodynamic stability, and long-term prognosis. The David procedure, a valve-sparing aortic root replacement, has emerged as a preferred approach for patients with aortic root aneurysms and preserved cusp function, offering excellent long-term durability while minimising the need for lifelong anticoagulation therapy. Similarly, TEVAR has revolutionised the management of aortic coarctation by providing a minimally invasive alternative to conventional surgical repair, particularly in adult patients. The ability of TEVAR to restore aortic patency, normalise haemodynamic parameters, and facilitate long-term remodelling of the aorta underscores its role as an essential component of modern cardiovascular intervention.
Conclusion
Implementing a two-stage hybrid approach—consisting of aortic root replacement with valve preservation via the David procedure as the first stage, followed by TEVAR for correcting aortic coarctation as the second stage—has demonstrated a highly favourable clinical outcome. This strategy ensured optimal haemodynamic stability, reduced surgical trauma, and mitigated the perioperative risks associated with extensive single-stage procedures.
The advancements in both open cardiac surgery and endovascular techniques have significantly expanded the therapeutic landscape for complex aortic pathologies, particularly in patients with coexistent congenital abnormalities such as aortic coarctation and bicuspid aortic valve disease.
The integration of these two advanced surgical techniques into a staged hybrid approach not only optimises patient safety and recovery but also highlights the evolving paradigm in the management of complex aortic diseases. By leveraging the strengths of both open and endovascular modalities, this strategy exemplifies the shift towards personalised, less invasive, and highly effective treatment solutions, ultimately improving patient prognosis and quality of life.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.