
Abstract
Aim
To characterize the impact of BMI (body mass index) on HIBI (hypoxic-ischemic brain injury) in patients receiving ECPR, with the hypothesis that elevated BMI is associated with increased risk of HIBI.
Methods
The Extracorporeal Life Support Organization (ELSO) registry was queried for patients who received ECPR during 2020-2024. Patients were categorized into 5 standard BMI groups. Normal Weight was used as the reference group. Generalized additive model (GAM) analysis was performed to identify the BMI range with greatest predicted HIBI risk. Multivariable logistic regression was used to compare odds of HIBI and post-HIBI mortality between standard BMI groups and Normal Weight.
Results
Of 6413 included patients (median age = 57.4, 68.6% male, median BMI = 28.1), 10.5% of Class 1 Obesity patients experienced HIBI compared to 5.0% of Normal Weight patients, 9.6% of Class 2 Obesity patients, 6.3% of Overweight patients, and 3.6% of Underweight patients (p < 0.001). GAM analysis showed a non-linear relationship between BMI and HIBI with highest predicted HIBI risk for Class 1 Obesity patients, which was confirmed by multivariable regression (adjusted odds ratio (aOR) = 1.86, 95%CI = 1.09, 3.20, p = 0.02). HIBI led to >90% mortality in all BMI categories, with increased odds of post-HIBI mortality for Class 1 Obesity patients compared to Normal Weight (aOR = 1.97, 95%CI = 1.14, 3.47, p = 0.016). There was no significant difference in odds of HIBI or post-HIBI mortality for any other BMI category compared to Normal Weight.
Conclusions
ECPR patients with Class 1 Obesity had increased odds of HIBI and post-HIBI mortality compared to Normal Weight patients after adjusting for covariates.
Introduction
Extracorporeal cardiopulmonary resuscitation (ECPR) using venoarterial extracorporeal membrane oxygenation (VA-ECMO) has been gaining attention as a rescue therapy in patients with refractory cardiac arrest. 1 However, despite representing a lifesaving treatment for many patients, ECPR has also been linked to various on-ECMO complications including acute brain injury (ABI). ABI can occur in up to 27%–32% of ECPR patients,2,3 and hypoxic-ischemic brain injury (HIBI) is one of the most common types of ABI in patients receiving ECMO treatment.3,4 A prolonged and profound ischemic and hypoperfusion state after cardiac arrest before VA-ECMO makes these patients especially vulnerable to HIBI and secondary reperfusion brain injury. While HIBI is well recognized complication of ECPR, there remains a paucity of research regarding specific risk factor of HIBI in patients receiving ECPR. Gaining a better understanding of risk factors of HIBI in ECPR patients has the potential to significantly improve our management of these critically ill individuals.
While several risk factors for both ABI including HIBI in patients receiving VA-ECMO have been identified,4–6 there is currently lack of research into the impact of BMI on these outcomes, particularly in patients receiving ECPR. Notably, obesity affects up to 20% of critically ill patients, and management of these patients poses specific and unique challenges. 7 Evidence exists to suggest an increased risk of complications for obese patients on ECMO including bleeding, 8 mortality, 9 and cardiovascular, renal, and device-related complications. 10 One study that investigated the association between the BMI and the favorable neurologic outcomes and survival to discharge of patients resuscitated from out-of-hospital cardiac arrest did not find significant differences between BMI groups. 11 However, the impact of BMI and obesity on HIBI outcome in ECPR patients, who are particularly vulnerable to neurological complications, is still largely unknown.
Thus, our study aims to fill this critical gap by characterizing the impact of BMI on HIBI in patients receiving ECPR, with the hypothesis that elevated BMI is associated with increased risk of HIBI and post-HIBI mortality.
Methods
Patients
The Extracorporeal Life Support Organization (ELSO) registry was queried for adult patients who received ECPR during 2020-2024. Patients were categorized into 5 standard BMI groups: Underweight (<18.5 kg/m2), Normal Weight (18.5-24.9 kg/m2), Overweight (25-29.9 kg/m2), Class 1 Obesity (30-34.9 kg/m2), and Class 2 Obesity (≥35 kg/m2). This retrospective observational cohort study was approved by the Johns Hopkins Hospital Institutional Review Board with a waiver of informed consent (IRB00216321). This study is reported using Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 12
Data source
The Extracorporeal Life Support Organization (ELSO) registry is a voluntary international database that collects information on use, indications, complications, and outcomes of ECMO support in adults and children from more than 50 countries. 13 Diagnosis and medical history are reported according to the International Classification of Diseases 9th edition (ICD-9) and 10th edition (ICD-10) codes.
For all included patients, we extracted the following information from the ELSO registry database: pre-ECMO demographic information; comorbidities; pre-ECMO clinical variables; laboratory values; on-ECMO clinical variable; and ECMO-associated morbidity and mortality, including HIBI, renal replacement therapy, hemolysis, arrythmia, gastrointestinal hemorrhage, and seizure. The ELSO variable for HIBI is defined as “Diffuse Ischemia” of the central nervous system.
Arterial blood gases were collected at baseline/pre-ECMO and at 24 h, and pCO2 difference was defined as pCO2 at 24 h - pCO2 at baseline/pre-ECMO. The pre-ECMO hemodynamics and arterial blood gas (ABG) values were measured no more than 6 h before ECMO; if the database contained multiple values, we chose those closest to the time of cannulation. Twenty-four-hour ABG values were drawn between 18 and 30 h after ECMO start time. Renal replacement therapy occurred during ECMO support.
Statistical analysis
Patient characteristics, clinical management, and outcomes data were summarized as medians and interquartile range [IQR] for continuous variables. Numbers and percentages were calculated for categorical variables. Continuous baseline characteristics were compared using the Wilcoxon rank-sum test, and discrete characteristics were compared using the Chi-square test. Normality of variables was assessed using Shapiro-Wilk testing and histogram visualization. A p-value of <0.05 was considered to be statistically significant. All statistical analyses were performed using R Studio (R 4.1.2, 2022).
Generalized additive model (GAM) analysis was performed to identify the BMI range with the greatest effect on predicted risk of HIBI. Multivariable logistic regression was used to compare odds of HIBI and post-HIBI mortality between standard BMI groups and Normal Weight. Normal Weight was used as the reference group for all multivariable models. Covariates included in the multivariable logistic regression were age, sex, race, comorbidities including diabetes, heart failure, chronic kidney disease, hyperlipidemia, and chronic obstructive pulmonary disease, ECMO indication, hours on ECMO, pre-ECMO pH, pre-ECMO HCO3, pre-ECMO PO2, PO2 at 24 h, pump flow, on-ECMO renal replacement therapy, and on-ECMO complications including circuit complications, gastrointestinal hemorrhage, seizure, arrythmia, and hemolysis.
Covariate selection (pre-selected) for multivariable models was guided by both literature review and clinical relevance of candidate predictors. Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated. Collinearity between confounders was assessed, with a variance inflation factor (VIF) greater than 5 considered to be indicative of problematic multicollinearity.
Results
Study population
Overall patient characteristics by BMI category.
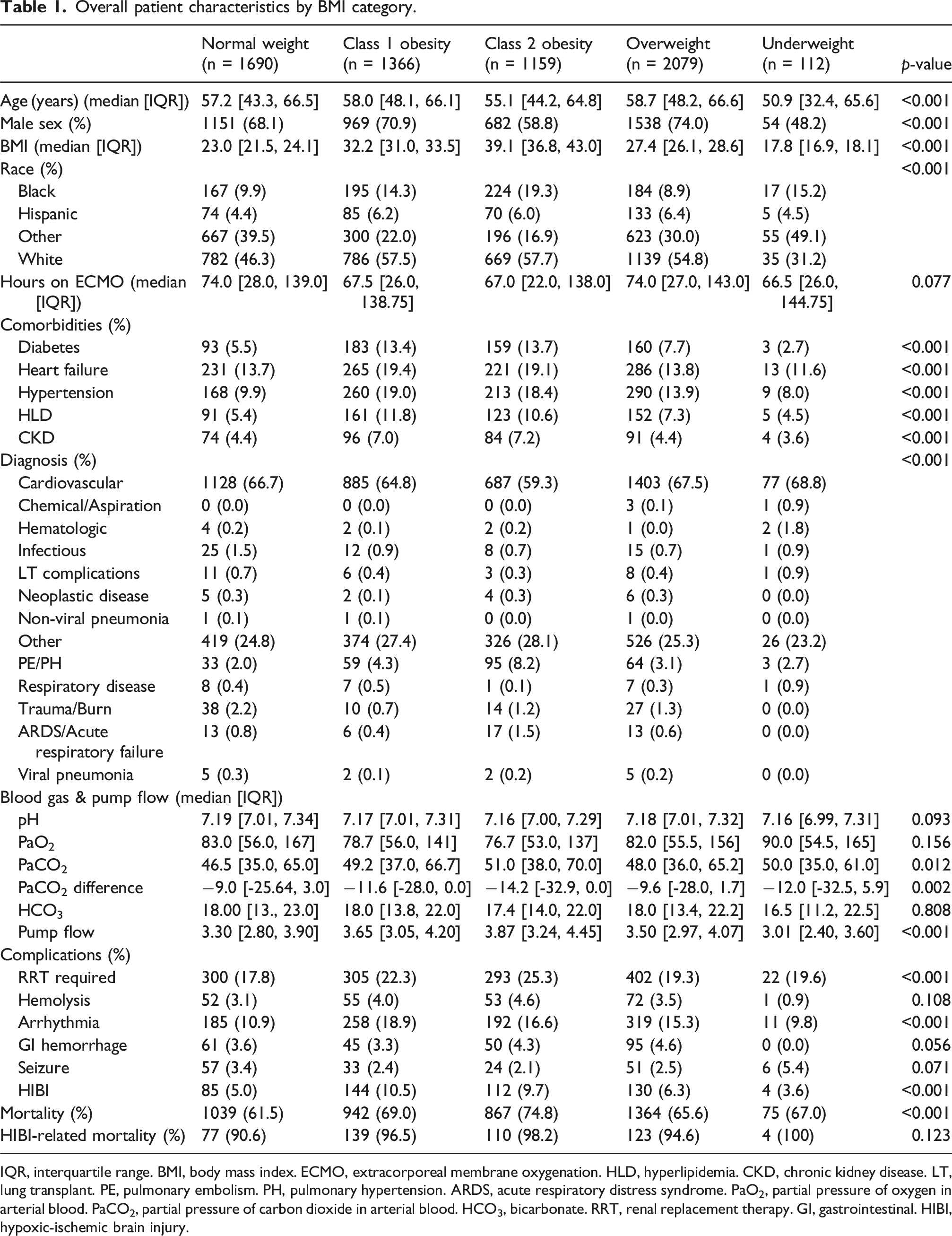
IQR, interquartile range. BMI, body mass index. ECMO, extracorporeal membrane oxygenation. HLD, hyperlipidemia. CKD, chronic kidney disease. LT, lung transplant. PE, pulmonary embolism. PH, pulmonary hypertension. ARDS, acute respiratory distress syndrome. PaO2, partial pressure of oxygen in arterial blood. PaCO2, partial pressure of carbon dioxide in arterial blood. HCO3, bicarbonate. RRT, renal replacement therapy. GI, gastrointestinal. HIBI, hypoxic-ischemic brain injury.
Normal Weight versus Class 1 Obesity Patient Characteristics Before and After Matching.
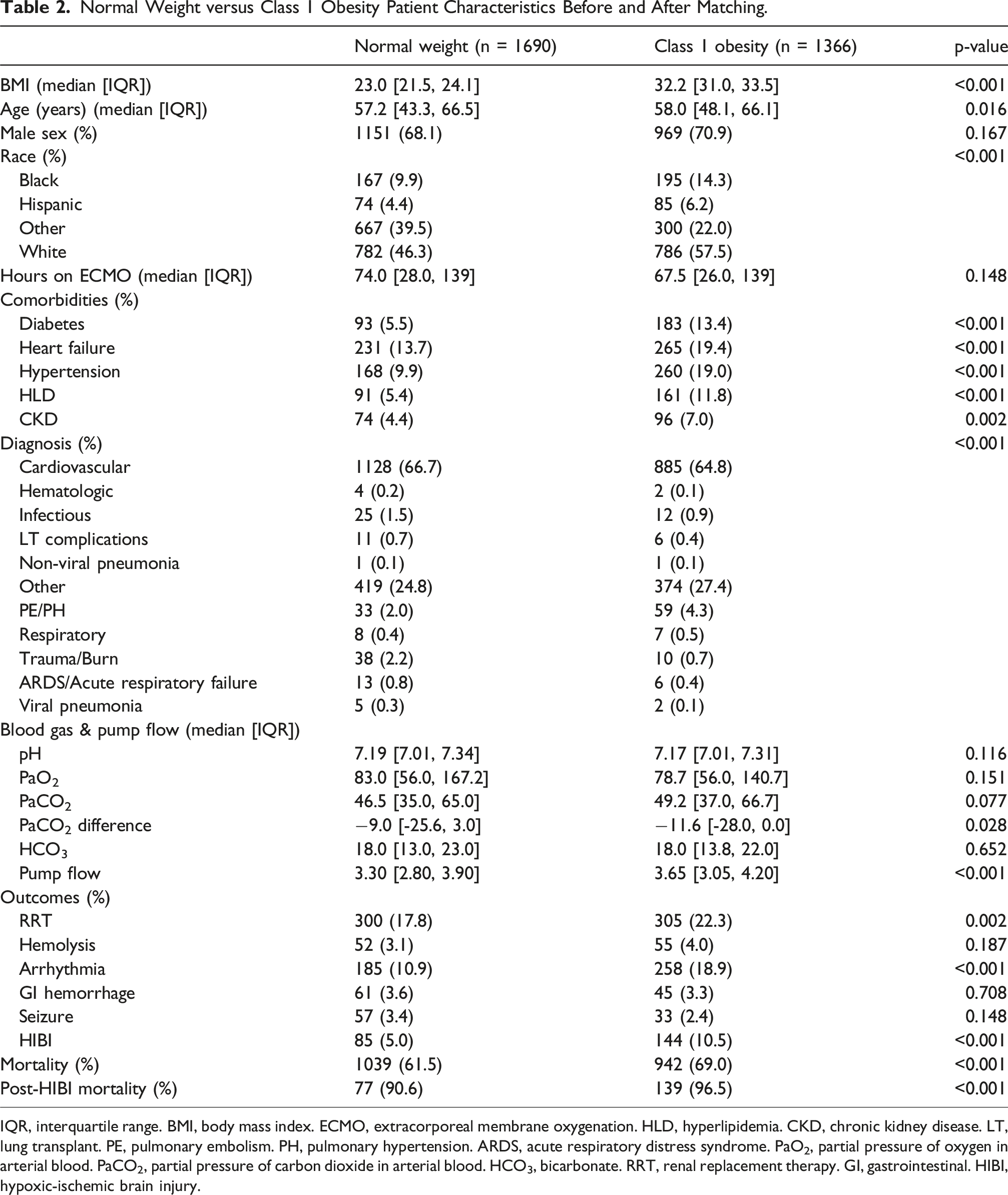
IQR, interquartile range. BMI, body mass index. ECMO, extracorporeal membrane oxygenation. HLD, hyperlipidemia. CKD, chronic kidney disease. LT, lung transplant. PE, pulmonary embolism. PH, pulmonary hypertension. ARDS, acute respiratory distress syndrome. PaO2, partial pressure of oxygen in arterial blood. PaCO2, partial pressure of carbon dioxide in arterial blood. HCO3, bicarbonate. RRT, renal replacement therapy. GI, gastrointestinal. HIBI, hypoxic-ischemic brain injury.
HIBI
Overall, 10.5% (n = 144) of Class 1 Obesity patients experienced HIBI, compared to 5.0% (n = 85) of Normal Weight patients, 9.6% (n = 112) of Class 2 Obesity patients, 6.3% (n = 130) of Overweight patients, and 3.6% (n = 4) of Underweight patients (p < 0.001). Supplemental Figure 1 shows the distribution of HIBI by BMI category.
GAM analysis showed a non-linear relationship between BMI and HIBI with highest predicted HIBI risk for Class 1 Obesity patients (Figure 1). This relationship was confirmed by multivariable logistic regression for Class 1 Obesity versus Normal Weight patients (adjusted odds ratio (aOR) = 1.86, 95%CI = 1.09, 3.20, p = 0.02) (Table 3). Multivariable regression did not reveal statistically significant differences in odds of HIBI for Underweight (aOR = 0.82, 95%CI = 0.12, 3.15, p = 0.80), Overweight (aOR = 1.24, 95%CI = 0.75, 2.09, p = 0.41), or Class 2 Obesity (aOR = 1.34, 95%CI = 0.73, 2.46, p = 0.34) patients compared to Normal Weight patients. Generalized additive model of effect of BMI on HIBI. The value on the y-axis indicates the contribution of BMI to the outcome after accounting for the smooth term in the model, representing the non-linear effect of BMI on risk of HIBI. The solid line represents the estimated effect, while the dashed lines show the confidence intervals around this effect. EDF, 4.87; p-value, 0.13. Multivariable logistic regression for HIBI by BMI category. ref, reference. CI, confidence interval. HIBI, hypoxic ischemic brain injury.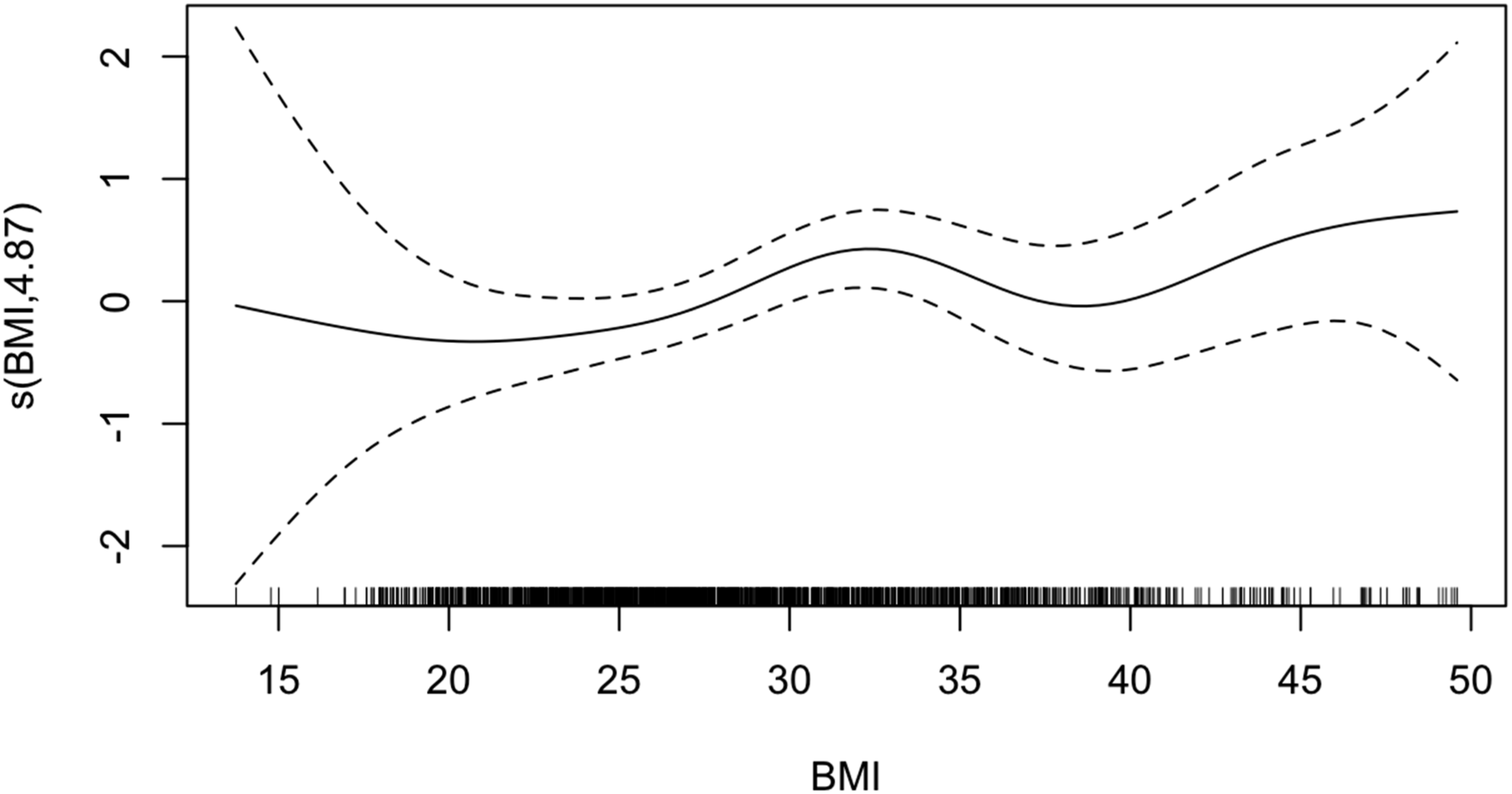
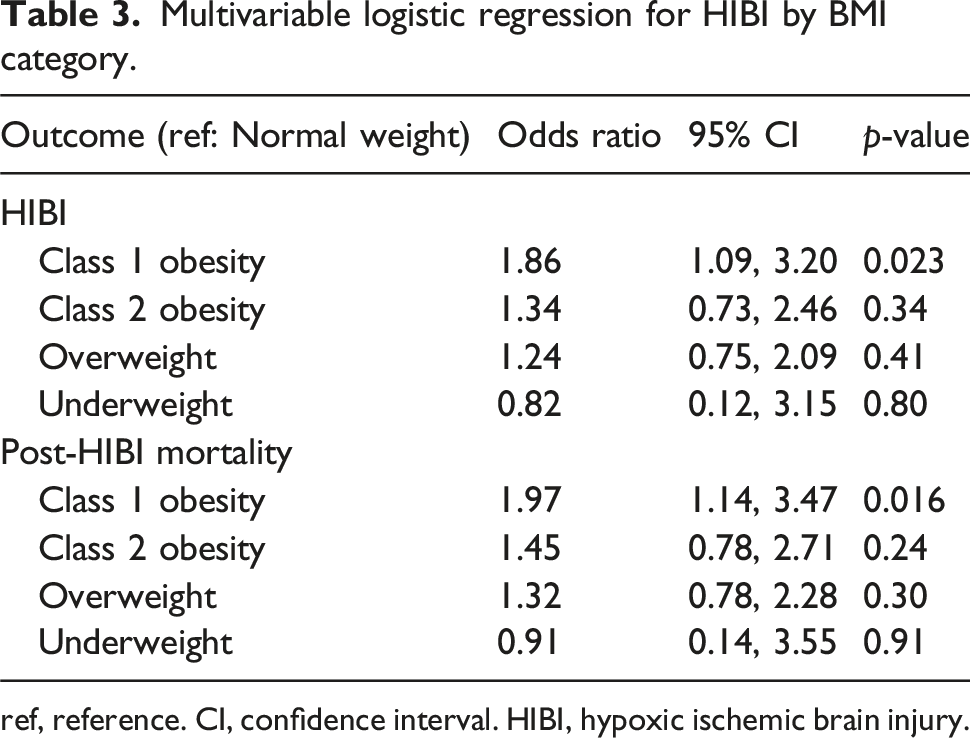
Post-HIBI mortality was greater than 90% for patients in all BMI categories (Table 1), and Class 1 Obesity patients also had increased odds of post-HIBI mortality compared to Normal Weight patients (aOR = 1.97, 95%CI = 1.14, 3.47, p = 0.016) (Table 3). No significant differences were found in post-HIBI mortality for other BMI categories.
Discussion
In this large multicenter ELSO registry analysis, we found that predicted HIBI risk was greatest for patients in the Class 1 Obesity BMI category compared to patients in the Normal Weight BMI category, and increased odds of both HIBI and post-HIBI mortality was confirmed by multivariable logistic regression. HIBI and post-HIBI mortality risk were comparable for Overweight, Class 2 Obesity, and Underweight patients compared to Weight patients.
The association between Class 1 Obesity and HIBI is particularly significant with respect to the high post-HIBI mortality of over 90% across all BMI categories. This is in line with a prior ELSO registry analysis on ECPR patients which demonstrated that neurological complications were one of the leading causes of withdrawal of life sustaining therapy including ECMO discontinuation. 14 Another recent ELSO analysis showed a non-linear relationship between stroke risk and BMI, revealing that class 1 obesity patients receiving ECPR may experience the highest risk of stroke compared to patients in other BMI categories including class 2 obesity or above. 15 Given that HIBI appears to be a near-fatal complication in ECMO patients, our findings highlight an urgent need to incorporate BMI as a factor in pre-ECMO risk assessment or models, and improve identification of markers of neurological vulnerability. Especially given that HIBI is likely to occur prior to ECMO cannulation, understanding the specific conditions that predispose patients to ischemic brain injury and associated mortality will be crucial for mitigating the risk of such complications.
While we hypothesized that patients with Class 1 Obesity may occupy a unique physiologic window in which metabolic factors and obesity-related burdens increase vulnerability to HIBI, our findings should not be interpreted as evidence that BMI itself is directly causative of ischemic brain injury. One plausible alternative is that obesity may contribute indirectly through technical and physiologic sequelae of resuscitation and ECMO, such as more difficult or prolonged cannulation, lower indexed flows, and greater challenges in delivering effective CPR in obese patients. These mechanisms may help explain why the association was strongest in Class 1 Obesity, and why no clear linear relationship across BMI strata was observed. Moreover, ECPR patients with obesity represent a preselected population, since those with significant comorbidities may be excluded from candidacy, which could influence both complication rates and outcomes. In light of the rising prevalence of obesity worldwide, these considerations further underscore the need to better delineate which factors – BMI itself versus its procedural and physiologic consequences – most strongly increase risk of HIBI.
This study has several limitations. Firstly, the ELSO registry gathers data on a voluntary basis, which could lead to selection bias of participating centers. Furthermore, while the ELSO registry encompasses a large and diverse patient cohort, variations in data reporting between participating centers could not be fully accounted for, which could affect the generalizability of our findings. As well, high and low BMI values are underrepresented in our sample. Secondly, despite robust adjustments for known confounders, the retrospective, observational nature of the dataset inherently limited our ability to infer causality from our findings. For example, obesity may not be a direct cause of ischemic brain injury, but could contribute to technical challenges such as difficult cannulation, prolonged no-flow times, and lower indexed flow in obese patients. Additionally, patients who died prior to imaging may have contributed to underestimation of HIBI incidence. Finally, challenges associated with imaging higher BMI patients while on ECMO may have led to underreporting of HIBI, particularly in patients with Class 2 Obesity. In this context, further studies with more granular data and improved standardization are necessary to refine our conclusions.
Conclusions
ECPR patients with Class 1 Obesity had increased odds of HIBI and post-HIBI mortality compared to Normal Weight patients after adjusting for clinically selected risk factors. Given that HIBI likely occurs prior to ECMO cannulation, further research regarding pre-ECMO risk factors is necessary to improve management of neurological outcomes in this vulnerable patient population. Additionally, future work should aim to clarify whether BMI itself contributes independently to HIBI risk, or whether observed associations are driven primarily by the procedural and physiologic challenges inherent in obesity – an urgent question in the context of increasing worldwide obesity rates.
Supplemental Material
Supplemental Material - Is body mass index associated with hypoxic-ischemic brain injury risk in extracorporeal cardiopulmonary resuscitation?
Supplemental Material for Is body mass index associated with hypoxic-ischemic brain injury risk in extracorporeal cardiopulmonary resuscitation? by Shi Nan Feng, Jin Kook Kang, Winnie L. Liu, Christopher J. Wilcox, Bo Soo Kim, Patricia Brown, Glenn J. R. Whitman, Sung-Min Cho in Perfusion.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental Material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.