
Abstract
Introduction
Mycotic thoracic aneurysms in children are rare and carry high mortality, particularly when complicated by erosion into adjacent pulmonary structures. Early recognition and surgical intervention are essential to prevent catastrophic outcomes.
Case Report
A 14-year-old presented with respiratory symptoms. Imaging revealed a large mycotic aneurysm of the aorta with compression of multiple mediastinal structures. During induction of anaesthesia, aneurysm rupture caused haemoptysis and hypovolemic arrest. Emergent femoral cannulation enabled initiation of cardiopulmonary bypass and novel use of endotracheal suction with autologous cell salvage facilitated surgical exposure and successful aneurysm repair.
Discussion
Thoracic mycotic aneurysms present diagnostic complexity and potential catastrophic outcomes. In this patient, rapid multidisciplinary coordination, dual-arterial cannulation and intraoperative blood-salvage techniques proved critical to restoring circulation and achieving surgical control.
Conclusion
Thoracic mycotic aneurysms in children require extreme vigilance and adaptable surgical strategies. This case demonstrates that survival is possible with innovative management in the face of life-threatening complications.
Introduction
Mycotic thoracic aneurysms in children require prompt surgical repair.1–3 Rupture into the airways can lead to massive haemoptysis and rapid demise. 4 We present a case salvaged by immediate initiation of cardiopulmonary bypass (CPB) and the use of novel perfusion techniques enabling repair via thoracotomy.
Case report
A 14-year-old female presented to a rural hospital with dyspnoea, cough and chest pain. Investigations revealed a suspicious mediastinal mass on X-ray, and high C-reactive protein and glucose levels. She was treated for suspected pneumonia and diabetic ketoacidosis before being transferred to our institution. Locally, a CT scan demonstrated a large saccular aneurysm of the proximal descending aorta with fat stranding along the lesser curvature, severe narrowing of the proximal right and mid left pulmonary arteries, occlusion of the left bronchus and oesophageal compression (Figure 1). Additional testing revealed elevated VDRL titres, suggestive of a syphilitic mycotic aneurysm. Given presence of symptoms, the patient was taken urgently to theatre for repair via a left thoracotomy. (a) CT demonstrating mycotic aneurysm of the proximal descending aorta. (b) CT showing 22 × 43 mm interposition graft.
In theatre, she was intubated with a 26Fr double-lumen (DL) endotracheal tube (ETT). There were low saturations, poor chest rise and no end-tidal CO2. Before tube placement could be confirmed, a large volume of blood was noted in the ETT, the DL ETT was replaced with a single lumed ETT to exclude the possibility of misplacement however bleeding became so brisk that it overcame the capacity to suction the ETT clear. A diagnosis of aneurysmal rupture into the airways was made, flooding the lungs and impairing ventilation. The ETT was clamped to limit blood loss, cardiopulmonary resuscitation was started, and the patient was urgently placed onto CPB via the right femoral vein and artery within 23 min of intubation. Haemodynamics were optimized on partial CPB while the remaining monitoring lines were placed.
Next, the patient was repositioned. A left thoracotomy was performed with difficult exposure of the descending aorta due to hepatisation of the lung parenchyma, which remained under arterial pressure. To control the aneurysm, a decision was made to unclamp the ETT, connect it directly to cell saver suction for processing, and re-transfuse this blood via the CPB circuit. With a reduction in intraparenchymal pressure, a clamp site was identified distally. However, it was still impossible to obtain proximal control without causing significant cardiac compression. Thus, the patient was cooled to 18°, the heart allowed to fibrillate without venting and an additional arterial limb spliced into the circuit to facilitate left carotid cannulation. With upper and lower body outflow cannula, dissection was completed, and the aneurysm was fully controlled.
A 22 mm interposition graft with a side arm was then sutured in place. Once the proximal anastomosis was complete, the carotid cannula was shifted to the side arm before resuming flow, rewarming the patient and performing the distal anastomosis. At 24°, sinus rhythm returned without ST changes. Due to difficult exposure, the aneurysm sac could not be entirely resected. The communication to the left bronchus was simply oversewn. The femoral artery was de-cannulated to avoid limb ischemia and support converted to extracorporeal membrane oxygenation (ECMO) to allow for lung rehabilitation. Haemostasis was eventually obtained after 4 h, allowing the thoracotomy to be temporarily closed, with the arterial ECMO cannula exiting through the 7th intercostal space.
On day 2, the patient underwent chest re-exploration and washout, and bilateral lung ventilation resumed without obvious leak. On day 7, she was de-cannulated, and her thoracotomy was fully closed. On day 9, she developed a transiently blown left pupil, but head CT remained normal. A follow-up MRI showed subtle features of early Wallerian degeneration in the cerebral peduncles, but no features of a global hypoxic injury. On day 25, she was transferred to her home hospital extubated and neurologically intact, although with ongoing critical illness polyneuropathy necessitating rehabilitation.
Discussion
We present a case of intrabronchial aortic aneurysm rupture after intubation. This represents an extremely rare and catastrophic complication. Nevertheless, the preparedness of our team with everyone present in the room at the start of the case, rapid identification of the issue, and collaborative problem-solving were key to the patient’s survival.
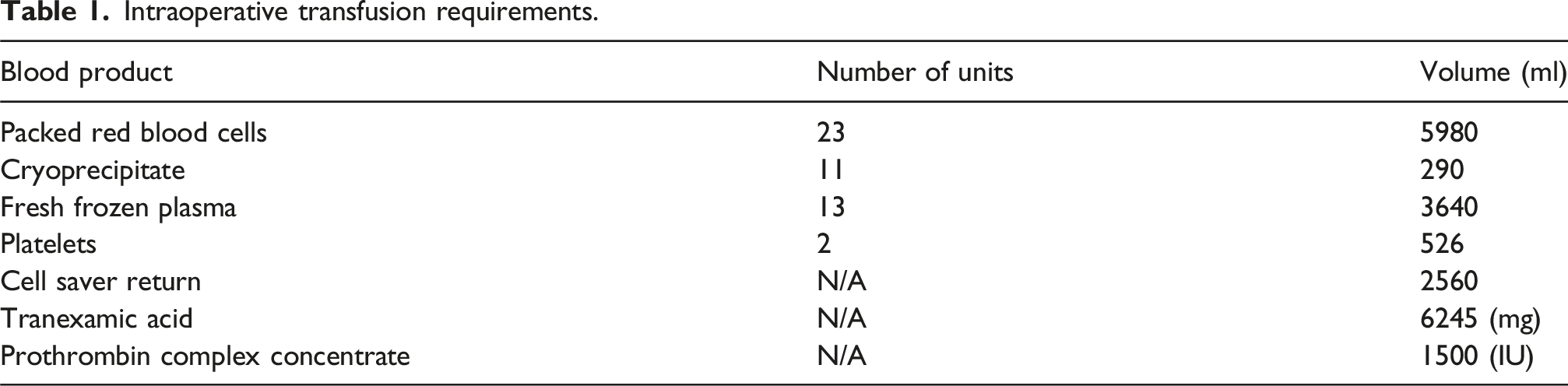
The innovative use of the endotracheal tube as an access point for cell saver suctioning represents an extreme salvage technique. However, it was essential to mitigate ongoing blood loss and maintain CPB flows. This approach also proved lifesaving by reducing lung parenchymal pressure, facilitating surgical exposure, and limiting our use of blood products (Table 1).
Although maintaining upper and lower body perfusion isn’t compulsory at 18°, it was the best option here considering the 23-min hypoxic time pre bypass. Furthermore, the case was technically challenging and could lead to longer aortic cross-clamp times than usual. Protecting the brain at all costs seemed necessary and worth the risk of carotid cannulation. The patient’s survival and intact cognitive function postoperatively reflect the success of aggressive resuscitation and cerebral protection strategies.
Intraoperative transfusion requirements.
Conclusion
Intrabronchial aortic aneurysm rupture represents a rare and catastrophic complication, which is best addressed with interdisciplinary collaboration and a flexible operative plan. Such cases require willingness to employ novel techniques when conventional approaches are insufficient, even in seemingly un-survivable scenarios.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.