
Abstract
Sweep gas nitric oxide (sNO) is emerging as an adjunctive therapy, which may have positive impacts on thrombosis and inflammation during ECMO treatment. sNO is administered to the gas phase of the ECMO oxygenator with the aim of reducing contact activation of blood when flowing through and over artificial surfaces. NO delivery devices have gas flow requirements that are above the sweep gases requirements of smaller patients supported on ECMO. To facilitate sNO delivery in patients requiring a sweep flow rate below the required bias flow rate of NO delivery devices, varying sNO delivery setups have been described. Here, we describe three systems for safe and reliable sNO delivery.
Introduction
Extracorporeal membrane oxygenation (ECMO) treatment induces a pronounced systemic inflammatory response syndrome (SIRS), endothelial activation and coagulopathy, leading to significant morbidity and mortality.1,2 Nitric oxide (NO) has multisystem effects, among them inhibition of platelet activation (via cyclic GMP increases), inhibition of tissue factor expression and inhibition of coagulation pathways as well as anti-inflammatory effects via inhibition of leukocyte adhesion and migration, inhibition of pro-inflammatory cytokine production and scavenging of reactive oxygen species. These multisystem effects make NO an ideal candidate to treat the aforementioned ECMO induced SIRS, endothelial activation and coagulopathy and has led to investigations of its role as an adjuvant treatment during ECMO.2–6
Nitric oxide (NO) can be administered to the lungs via inhalation (iNO) using well-established clinical delivery systems. A less common, and comparatively underdeveloped, approach involves the administration of NO to the oxygenators of ECMO circuits by blending NO into the sweep gas (sNO). 7 This method presents a range of legal, ethical, regulatory, and environmental challenges, which are discussed within this manuscript. This review specifically addresses the practical aspects of sNO delivery and neither explores the dose-response characteristics of NO nor outline the underlying pathophysiological rationale for employing sNO in ECMO. These topics have been comprehensively reviewed by Brinkley et al. (published in Perfusion) and Chiletti et al.2,8
Most NO delivery systems require a minimum bias flow of 2–4 L/min for reliable NO delivery, while ECMO sweep flows, especially in children, can be as low as 100 ml/min to avoid excess CO2 removal from the blood stream. To address the mismatch between bias and sweep flow requirements, various setups have been reported.6,9,10
Legal and regulatory considerations
NO is approved by major regulatory agencies—including the U.S. Food and Drug Administration (FDA), the European Medicines Agency (EMA), and the Australian Therapeutic Goods Administration (TGA) —for the treatment of term or near-term neonates with hypoxic respiratory failure, with or without evidence of pulmonary hypertension.11–13 In addition, the EMA has approved NO for the management of peri- and postoperative pulmonary hypertension in patients undergoing cardiac surgery, an indication not approved by the FDA.12,13 The TGA indications are largely consistent with those of the EMA. The use of NO within extracorporeal membrane oxygenation (ECMO) circuits is not approved by any major regulatory body and must therefore proceed under established off-label use frameworks. 8
A detailed discussion of off-label use processes is beyond the scope of this review; however, such use requires adherence to institutional and regulatory policies. These typically include consultation with an Institutional Review Board (IRB) or Pharmacy and Therapeutics (P&T) Committee, obtaining and documenting informed consent and recording of the rationale for off-label use in the patient’s medical record. 14 Adverse events should be reported to the relevant pharmacovigilance authority (e.g., FDA MedWatch, TGA Database of Adverse Event Notifications). Furthermore, any improvised combination of equipment to enable delivery of sNO may be considered a novel medical device by regulatory agencies and may require additional device-specific approval prior to clinical use. 15
Environmental considerations
Clinical use of NO needs to consider safety measures, as uncontrolled exposure to NO or its reaction products may pose risks to healthcare personnel. 16 In ambient air, NO can undergo rapid oxidation to nitrogen dioxide (NO2), a highly toxic gas that is corrosive and irritating to the eyes, respiratory tract, and mucous membrane. 8 Occupational exposure limits have been established by regulatory bodies such as the U.S. Occupational Safety and Health Administration (OSHA), which specify a permissible exposure limit (PEL) for NO of 25 ppm for an 8-h time-weighted average (TWA) and a ceiling limit of 1 ppm for NO2.16,17 Consequently, even direct exposure to sweep gas containing 20 ppm NO would remain below the OSHA TWA for NO. NO2 formation has been shown to be around 1.15% of the NO dose when the FiO2 is > 0.95, i.e. for a dose of 20 ppm the resulting NO2 formation would be 0.23 ppm, making exposures beyond the OSHA limits very unlikely. 18 Consequently, NO scavenging is not performed during inhaled use, nor in any of the systems described below.
NO delivery systems
Commercially available NO delivery devices rely on three different technologies: Cylinder based gases, ionization-based NO systems and cassette-based NO systems. Cylinder-Based Systems use pressurized cylinders of NO gas, connected to a flow regulator, to deliver a controlled dose of NO to the patient’s breathing circuit. Ionization-Based Systems generate NO from air using an electrical discharge and splitting air into NO, nitric dioxide (NO2) and ozone (O3). 19 While NO2 and ozone are scavenged, NO is delivered to the patient. Cassette-Based Systems use pre-filled cassettes containing NO, which is mixed with air before delivery to the patient.
Delivery of NO in ventilator bias flow
All nitric oxide delivery systems are primarily designed to facilitate iNO delivery via mechanical ventilators. They rely on a defined bias gas flow to assure both adequate mixing of iNO into ventilator gasses, and sampling of this gas mix after the injection port to monitor oxygen, NO and NO2 concentrations. 7 To assure a defined iNO concentration, the bias flow is measured in the injector module, and, depending on flow, a defined amount of NO is injected into the gas flow. To confirm the dose of NO, distal to the injection a defined amount of gas (sampling flow) is aspirated from the bias flow. The required minimum bias flow varies between systems, from 100 mls to 2 L per minute (LPM). Equally, the sampling flow varies between around 130 to 300 mls/min.
Nitric oxide delivery into sweep gas of ECMO systems (sNO)
Providing sNO into ECMO systems, while technically easily achievable, presents challenges, particularly in pediatric patients, where the required sweep gas flow rate may be lower than the minimum bias flow that is required for effective NO delivery by the respective NO delivery device. Three setups have been described in the literature to facilitate reliable and safe sNO in children.
Royal children’s hospital Melbourne, Australia
The system used at RCH Melbourne was described previously.
20
A wall oxygen and air supply is blended in a Sechrist blender (Sechrist, Anaheim, CA, USA), which subsequent downregulation of the gas flow via a flow regulator (IR2000, SMC Pneumatics, Yorba Linda, USA) which is set to 55 mmHg. This flow regulator prevents excessive pressure transduction into the INOMax DSIR™ system. NO is then delivered via the INOMax DSIR™ injection module into the air/O2 sweep gas flow. The resulting air/NO/O2 mix then flows through a filter, where it is sampled and particles, which may lead to the indicator bobbin of the second flow meter getting stuck, are filtered. The flow regulator (IR2000) may contain aluminum, which in the past has been deemed to carry a risk of aluminum fires. More recently, this risk has been deemed extremely low, and many ventilators contain aluminum parts that may come into contact with oxygen. This system has been in place since 2018, and after treatment of >300 patients has proved to be safe (Figure 1). sNO delivery at RCH Melbourne using the INOMax DSIR NO delivery system (Courtesy S Horton).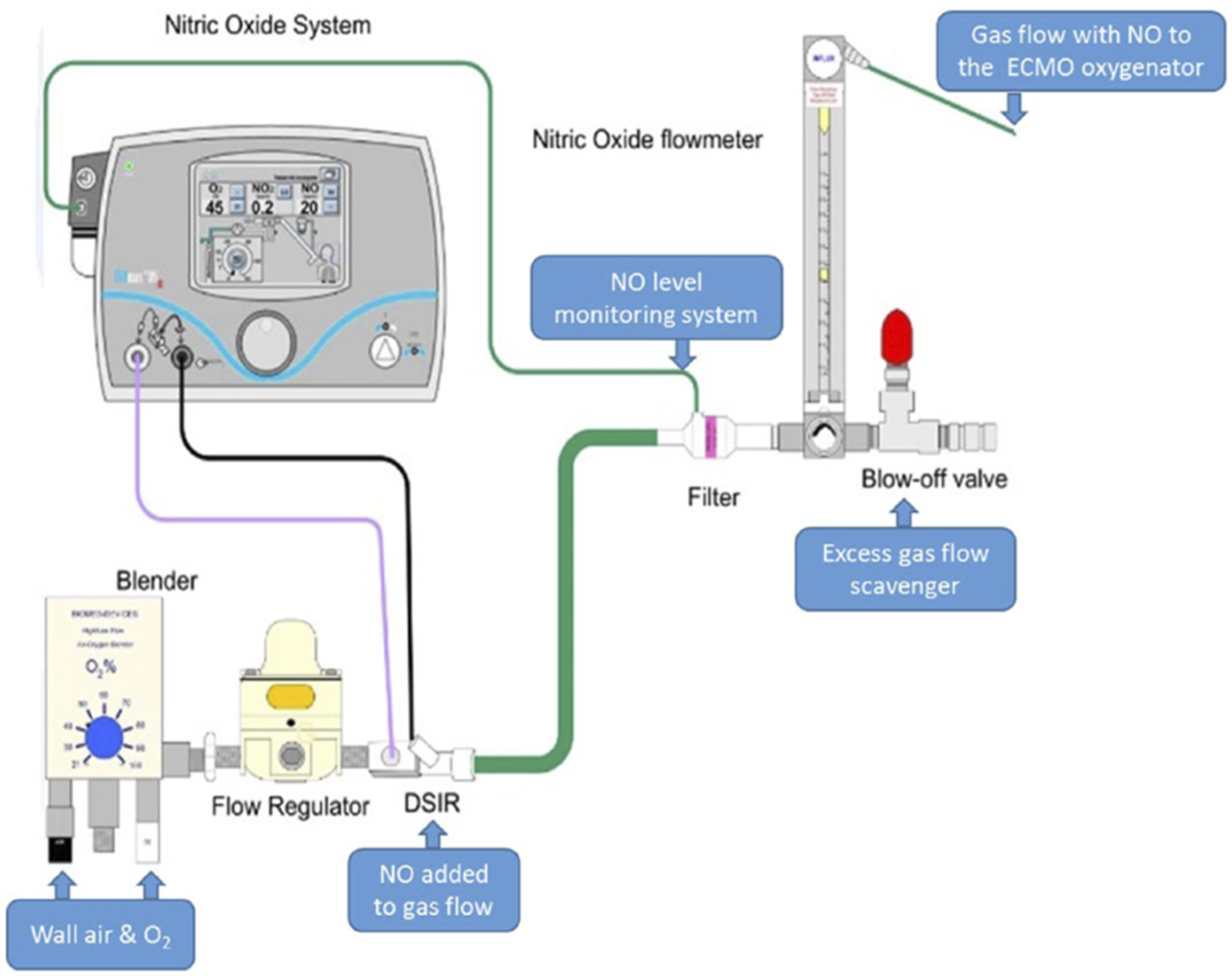
Children’s of Alabama, Birmingham, Alabama, USA & Congenital Heart Center, University of Florida, Gainesville, Florida, USA
The system used at UF Florida was described previously.
5
For patients requiring a sweep gas flow rate of 2 LPM, the wall supply oxygen and air, respectively, are mixed and downregulated in a Sechrist blender/flow meter combination (Sechrist Industries, Anaheim, USA), providing the desired sweep gas flow. The INOMax DSIR sNO delivery at the Congenital Heart Center, University of Florida (Courtesy of G Peek).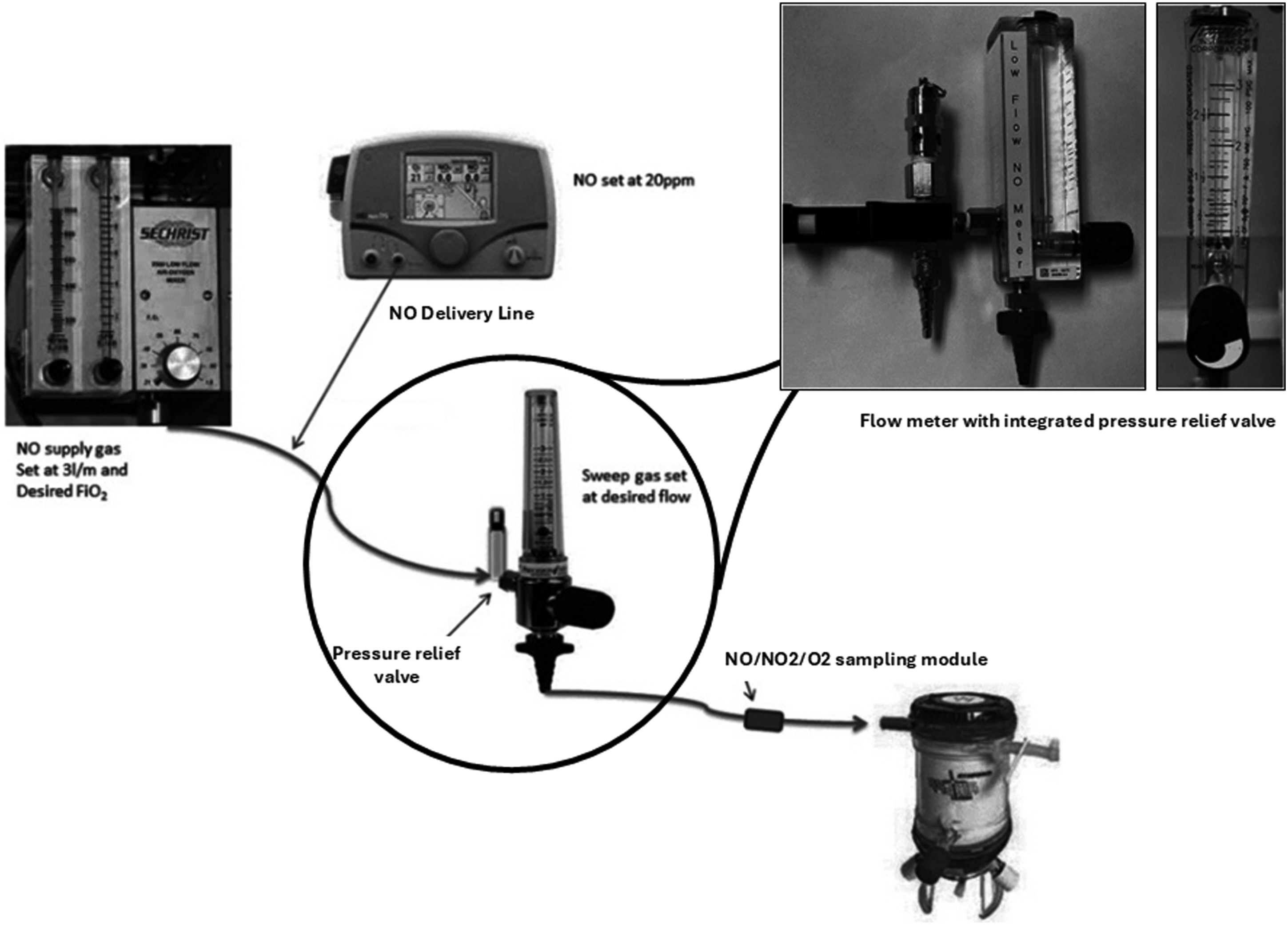
Queensland children’s hospital, Brisbane, Australia (The NECTAR trial)
The system used at QCH Brisbane was described previously.
10
The wall supply oxygen and air, respectively, are mixed and downregulated in a Sechrist blender/flow meter combination, providing the desired sweep gas flow. The SoKINOX sNO delivery for the NECTAR trial.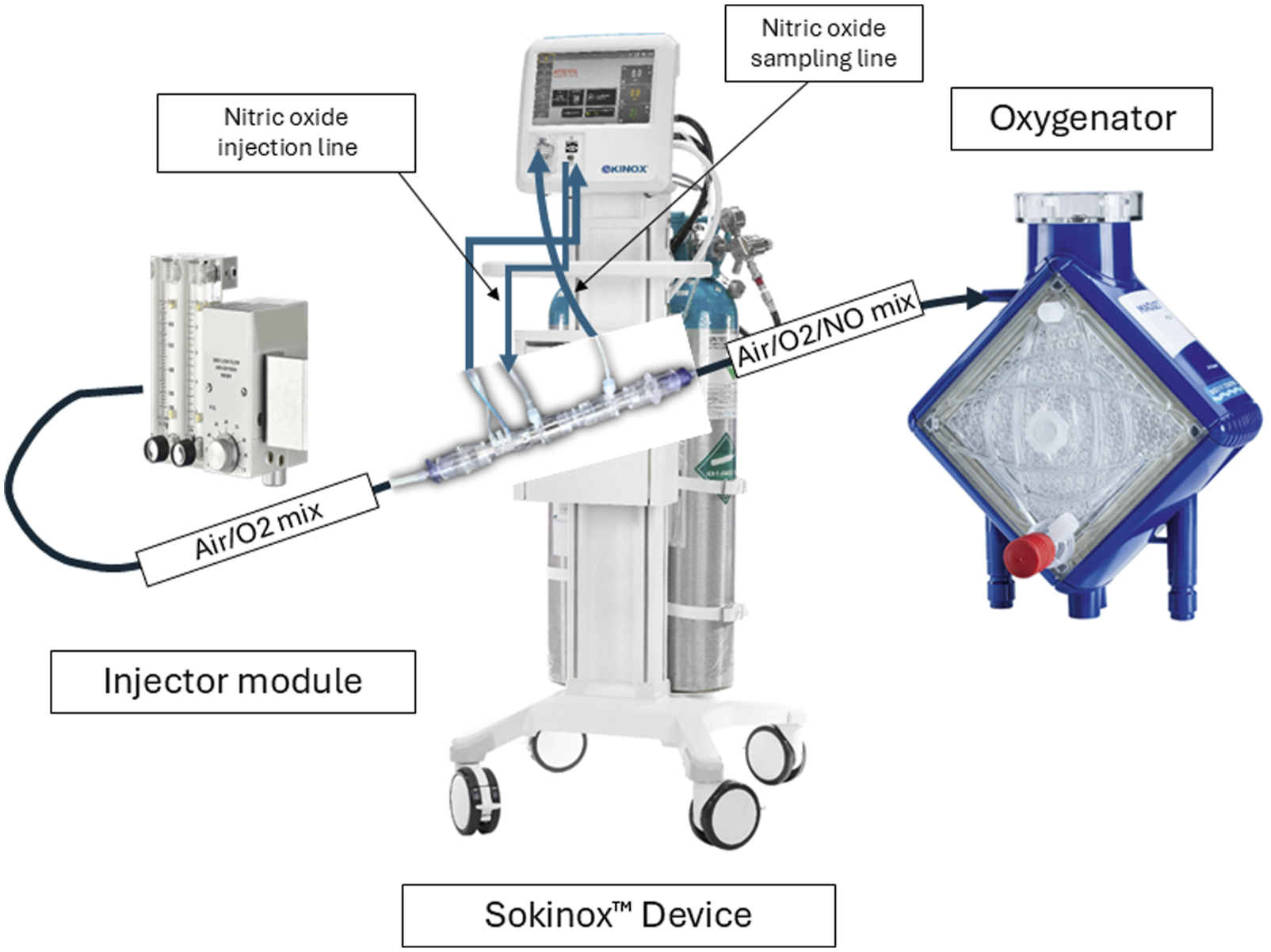
Discussion
Nitric oxide may be a beneficial adjunctive therapy for ECMO in children and continues to both be used in clinical practice as a standard of care, as well as investigated in clinical trials. Providing sNO has challenges due to the mismatch between NO delivery machine bias flow and desired sweep flow requirements. sNO has been used in CPB setups where, when very low sweep gas amounts were needed, CO2 is added to compensate for excess CO2 removal. 3 Addition of CO2 to the sweep gas in ECMO systems however, while feasible, carries a high risk of large CO2 variations, which is associated with neurological morbidity. 21 Therefore, designing systems that don’t rely on CO2 addition to sweep flow is desirable.
We describe three systems previously reported in the literature, each demonstrating that sNO can be delivered safely and reliably, albeit with varying technical configurations and associated challenges. The SoKINOX™ is the simplest setup and avoids ad hoc changes to existing equipment. The clinical safety of the system has been tested and – as a NO delivery device - it has been approved by regulatory bodies, whereas the other two described systems do not have regulatory approvals. At very low sweep gas requirements the SoKINOX device however will fail to deliver sNO reliably, as it is not possible to reduce sNO to less than 170 ml/min, as unlikely a requirement this may be in clinical practice.
sNO treatment remains an off-label use of NO, which may require special institutional approvals, as well as patient consent. Currently, there is no system with regulatory approval available on the market that allows for very low sweep flows. It could, however, be easily designed by increasing the NO sampling rate to the same amount as the minimum bias flow requirement of the NO injection system. In such a system, effective sweep flow rates below 200 ml/min could be achieved without any complex setups that allow for such low sweep flow rates.
Footnotes
Ethical consideration
No Human Ethics and Research approval was required for the work described in this manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Adrian C Mattke conducted the NECTAR trial, which was supported by Air Liquide™ in kind with provision of nitric oxide, as well as the SoKINOX™ machine.