
Abstract
Introduction
Refractory cardiac arrest carries a poor prognosis. Extracorporeal cardiopulmonary resuscitation (ECPR) can be lifesaving but is associated with high morbidity and mortality. We report a likely underdiagnosed complication — non-occlusive mesenteric ischemia (NOMI) — following ECPR, emphasizing the diagnostic challenges and the role of early endoscopic evaluation and an interdisciplinary assessment of these patients.
Case Presentation
A 48-year-old man presented with ST-elevation myocardial infarction and developed refractory cardiac arrest due to ventricular fibrillation. ECPR was initiated, and extracorporeal membrane oxygenation (ECMO) flow was achieved after 77 min of cardiopulmonary resuscitation. Early after arrest, the patient passed bloody stool, raising suspicion of mesenteric ischemia. Computed tomography was inconclusive, but colonoscopy revealed ischemic bowel injury. Given the fatal potential of untreated NOMI, prompt colectomy was performed. The patient stabilized postoperatively, recovered progressively, and was discharged from the intensive care unit in good condition after 14 days.
Conclusion
NOMI should be considered in ECPR patients presenting with gastrointestinal bleeding, even when cross-sectional imaging findings are inconclusive. Early colonoscopy enables timely diagnosis and surgical intervention, potentially improving survival in this high-risk setting.
Keywords
Introduction
Non-occlusive mesenteric ischemia (NOMI) is a rare but often lethal complication in critically ill patients.1–3 Excessive vasopressor use contributes to its development by maintaining systemic arterial pressure at the expense of mesenteric microcirculation.2,4
Recent evidence indicates that NOMI may also occur after cardiopulmonary resuscitation (CPR) and is likely more frequent in patients undergoing extracorporeal cardiopulmonary resuscitation (ECPR). 5 Possible mechanisms include ischemia during prolonged CPR, post-resuscitation hypoperfusion, and high-dose vasopressor administration. NOMI may often be underdiagnosed in critically ill patients as diagnosis is challenging, particularly under ECMO support. Early computed tomography (CT) after CPR may suggest bowel ischemia6–8 but definitive diagnosis typically requires endoscopic and/or surgical assessment. 9 NOMI carries a high mortality risk and therefore, early diagnosis is essential. 5
We report a case of prolonged low-flow cardiac arrest managed with ECPR, complicated by NOMI, in which timely diagnosis and surgical intervention led to full recovery.
Patient information and clinical findings
Cardiac arrest
A 48-year-old man with no known medical history experienced acute chest pain and contacted emergency medical services. Shortly thereafter, he suffered a witnessed cardiac arrest. No bystander cardiopulmonary resuscitation (CPR) was initiated. Advanced life support (ALS) was started by paramedics after an estimated no-flow time of 5 minutes. The initial rhythm was ventricular fibrillation. Immediate defibrillation was performed but no return of spontaneous circulation (ROSC) could be achieved.
ECPR initiation after arrival in hospital
The patient was diagnosed with refractory cardiac arrest and transported under ongoing mechanical CPR to the nearest hospital that was able to initiate extracorporeal cardiopulmonary resuscitation. In our regional ECPR provider network, selected hospitals are designated as ECPR initiation sites, equipped and staffed for rapid ECMO priming and cannulation. When feasible, the ECMO retrieval team from our tertiary center performs cannulation; however, in refractory arrest, local initiation is often required to minimize low-flow time.
In the initiation hospital, ECMO (CARL, Resuscitec GmbH, Freiburg, Germany) flow was established 77 min after cardiac arrest. Post-ECPR electrocardiography revealed ST-segment elevation in the anterior leads. Emergent coronary angiography identified an occlusion of the left anterior descending artery. Percutaneous coronary intervention with placement of a 4.0 × 22 mm drug-eluting stent was successfully performed. In accordance with our local ECPR protocol, the patient was subsequently transferred to the ECMO center at University of Freiburg Medical Center, Germany, for post-resuscitation management. Before transport, the patient passed bloody stools without the need of immediate blood transfusions and without signs of major lower intestinal bleeding.
First day after ECPR
According to local standards, a full body post resuscitation CT-scan was performed before admission to our ICU showing signs of pulmonary aspiration and a sternal fracture but no other resuscitation-related complications. The cerebral CT-scan showed no signs of hypoxic-ischemic encephalopathy. Upon ICU admission, the patient was intubated requiring invasive respiratory support and catecholamines (norepinephrine and epinephrine) in high doses. A targeted temperature management at 33°C for 24 h was initiated.
Non-occlusive mesenteric ischemia
As the patient developed bloody stools, suspicion of mesenteric ischemia was raised although the initial CT scan showed no definite signs of manifest intestinal ischemia. The colon appeared mildly hypoperfused, with possible chronic post-inflammatory fatty infiltration. Early ischemic alterations could not safely be excluded.
Serum lactate increased to 15 mmol/L within the first 9 h of treatment, despite adequate ECMO flow. Given the inconclusive CT findings, the limited sensitivity of CT for early mesenteric ischemia, and the marked rise in lactate, early bedside colonoscopy was indicated. Endoscopy was selected over laparoscopic exploration because it was considered to entail lower procedural risk and was feasible at the bedside. Coloscopy showed transmural ischemia of the right hemicolon (Figure 1(A) and (B)), establishing the diagnosis of NOMI. A and B: Colon ischemia. Both pictures show an intraluminal view during bedside colonoscopy on the ICU.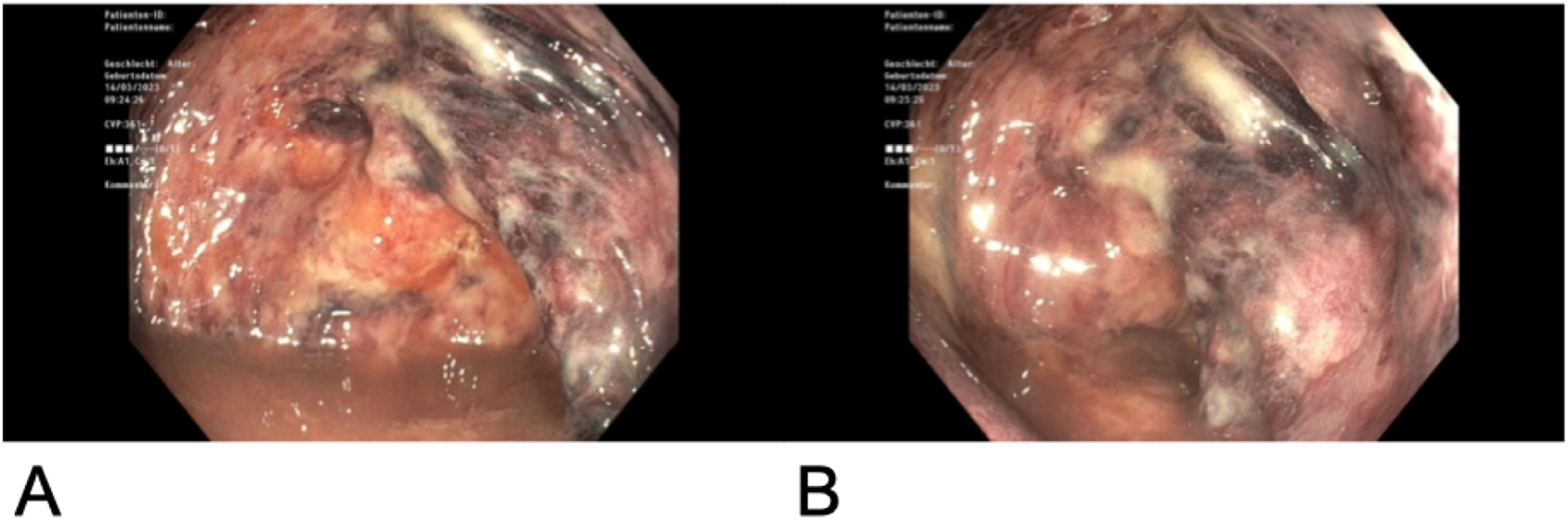
An interdisciplinary discussion involving gastroenterology, intensive care, anesthesiology and abdominal surgery teams evaluated the risks of operative intervention — namely bleeding under ECMO support and dual antiplatelet therapy — against the lethality of untreated NOMI. Despite the uncertain neurological prognosis, surgery was recommended.
Right hemicolectomy with terminal ileostomy and blind closure of the transverse colon was performed. Postoperatively, bowel motility recovered with neostigmine and laxatives, and defecation normalized promptly.
Further course on ICU
ECMO was maintained for 7 days until decannulation (for parameters, see Table 1). Initial transthoracic echocardiography demonstrated a left ventricular ejection fraction (LVEF) of 38% without additional structural abnormalities. Due to the risk of malignant ventricular arrhythmias, a wearable cardioverter-defibrillator (LifeVest, Zoll Medical, Cologne, Germany) was prescribed pending definitive assessment for implantable cardioverter-defibrillator (ICD) implantation.
Acute renal failure secondary to tubular necrosis required renal replacement therapy for 5 days before full recovery of renal function. The high-output ileostomy was effectively managed with opioid therapy.
After rewarming, the patient developed transient hemiplegia and delirium; both resolved spontaneously, with delirium improving rapidly through reorientation measures. After 14 days, the patient was discharged from the intensive care unit and transferred back to the ECPR initiation hospital. At discharge, he was fully conscious and neurologically recovered (Cerebral Performance Category 1).
Follow-up
VA-ECMO parameters from initiation of ECPR to decannulation on day 7, with all corresponding parameters recorded throughout the support period.
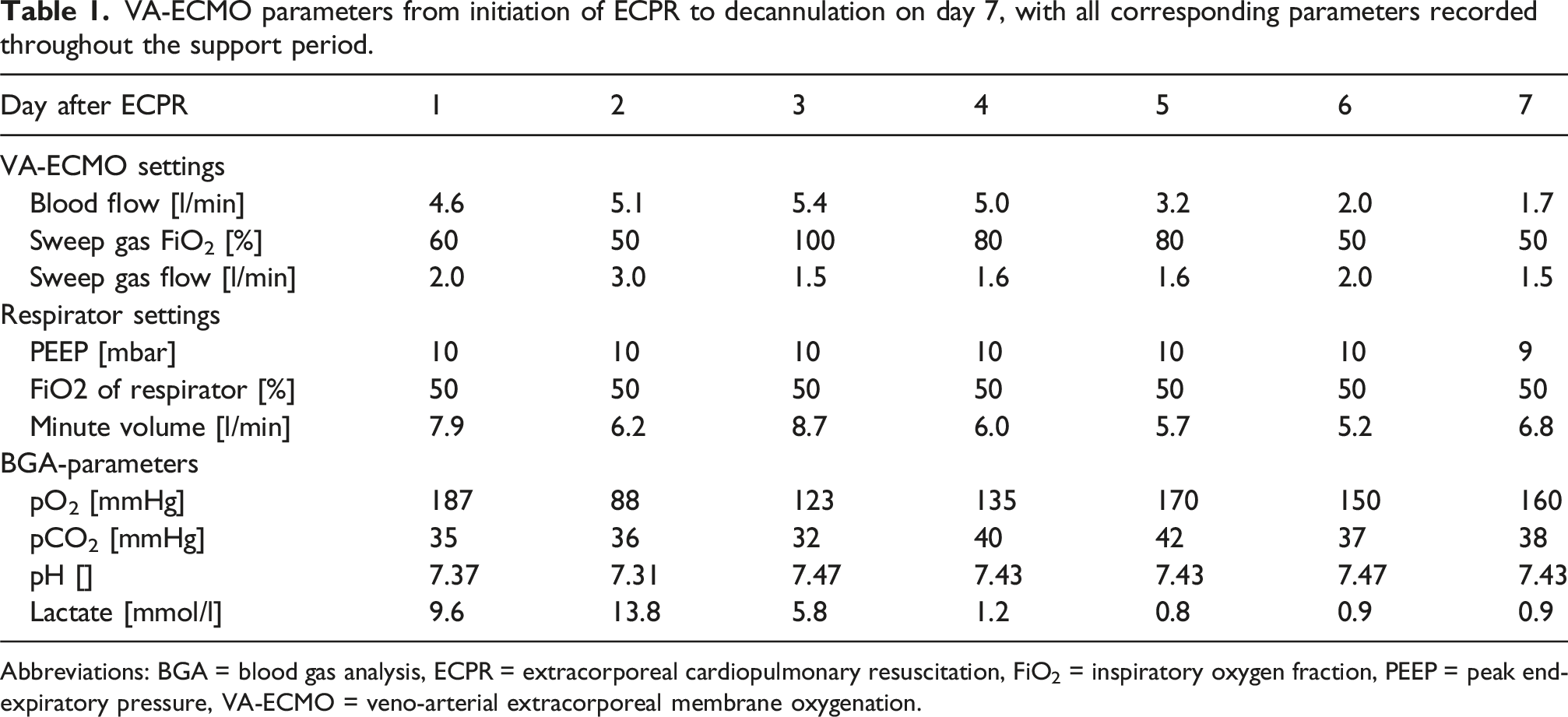
Abbreviations: BGA = blood gas analysis, ECPR = extracorporeal cardiopulmonary resuscitation, FiO2 = inspiratory oxygen fraction, PEEP = peak end-expiratory pressure, VA-ECMO = veno-arterial extracorporeal membrane oxygenation.
Discussion
We describe a case of NOMI following ECPR) that was successfully managed by right hemicolectomy. This case illustrates that, even after prolonged low-flow time and severe systemic insult, meaningful recovery is possible when NOMI is recognized early and treated surgically.
First, the time to ECMO in this case was prolonged (77 min) due to logistical and anatomical factors that were not anticipated at the time ECPR was indicated. Whether NOMI resulted from this extended low-flow period, or could have been prevented by earlier ECMO initiation, cannot be established from this case report. Nevertheless, substantial evidence indicates that shorter low-flow durations improve outcomes in ECPR, and minimizing time to ECMO should remain the priority, independent of NOMI.10,11 Without operative intervention, transmural ischemia most likely would have been fatal as in NOMI mortality exceeds 70%.1,9 In accordance to the patient’s presumed wishes, laparotomy and bowel resection was performed.
The diagnosis of NOMI remains a major challenge in post-ECPR patients.2,3,6 In this case, despite a multiphasic CT including scans in arterial and portalvenous phase performed several hours after the first bloody stool, imaging failed to reveal intestinal ischemia. Elevated lactate levels were observed but are nonspecific in ECPR, as global hypoperfusion and metabolic stress are common. Recent data from a secondary analysis of the Prague OHCA study 5 suggest that clinical signs such as diarrhea and abdominal distension are also unreliable, yet NOMI occurred in over half of ECPR patients and was associated with poor neurological outcomes in 89%. Previous reports have highlighted the limited sensitivity of CT for detecting NOMI. 8 Based on these findings, our center now performs early colonoscopy in post-ECPR patients with gastrointestinal symptoms to ensure timely diagnosis and resection when indicated.
Surgical management in ECPR patients is complex. Coagulopathy and bleeding are common and aggravated by extracorporeal circulation 12 and concurrent anticoagulation or dual antiplatelet therapy after coronary intervention. In addition, the requirement for anticoagulation on V-A ECMO conflicts with the need for adequate coagulation during abdominal surgery. 13 Therapeutic anticoagulation is necessary to prevent thromboembolism. 12 On the other hand critical bleeding during surgery is not uncommon. 13 In our case, bleeding was minimal despite dual anti platelet therapy. Vasoplegia, capillary leak, and the need for high-dose vasopressors after CPR further increase perioperative risk and may be aggravated by ECMO. 14 Additionally, neurological prognosis is often uncertain in the early post-ECPR phase, complicating surgical decision-making. 15
A legitimate ethical concern arises regarding the appropriateness of major abdominal surgery in patients with potentially severe hypoxic brain injury. The decision to pursue or withhold surgery must balance the risk of futility after potentially severe hypoxic brain injury against the possibility of recovery. In this case, multidisciplinary consensus, and the absence of radiological evidence of cerebral injury supported the decision to operate.
Conclusion
This case demonstrates that NOMI after ECPR, though often fatal, can be survivable with good neurological outcome after early recognition, endoscopic confirmation and timely surgical intervention. CT imaging alone may be insufficient, and routine early colonoscopy in symptomatic patients should be considered. Multidisciplinary decision-making and individualized evaluation of neurological prognosis are critical for optimizing outcomes.
Footnotes
Consent for publication
The patient gave informed consent for publication of all clinical details and accompanying materials published in this case report.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: FAR, GS, MAS, KMP and PD declare no conflicts of interest. DB declares Lecture fees from Falk Foundation and W. L. Gore & Associates, Travel Grants from Gilead Science and Research grants from Dr Rolf M. Schwiete-Stiftung and German Research Foundation (DFG). VZ received travel support from Orion Pharma and lecture honoraria from Medela and AstraZeneca. AS declares a research grant, lecture honoraria and travel support from CytoSorbents Europe, lecture honoraria from AstraZeneca and Getinge, and travel support from Artcline. TW received lecture honoraria or travel support from Abbot Medical, AstraZeneca and Boston Scientific. DLS received lecture honoraria or travel support from Abiomed, AstraZeneca, Dahlhausen, Getinge, Medtronic, Orion Pharma, and was part of a dual lumen advisory board by Medtronic.