
Abstract
Background
Utilization of extracorporeal membrane oxygenation (ECMO) has expanded substantially, yet structured training for surgical residents remain limited. We established a dedicated ECMO/mechanical circulatory support (MCS) fellowship for general surgery residents on dedicated academic time and evaluated its feasibility, educational impact, and association with institutional outcomes.
Methods
A single-center retrospective review was performed comparing ECMO activity and outcomes before and after fellowship implementation. . Institutional outcomes were compared across pre-fellowship and fellowship eras. Fellows’ clinical involvement was quantified through procedural logs and self-reported comfort levels. A multidisciplinary survey assessed perceptions of workflow, communication, and education using 5-point Likert scales and free-text feedback.
Results
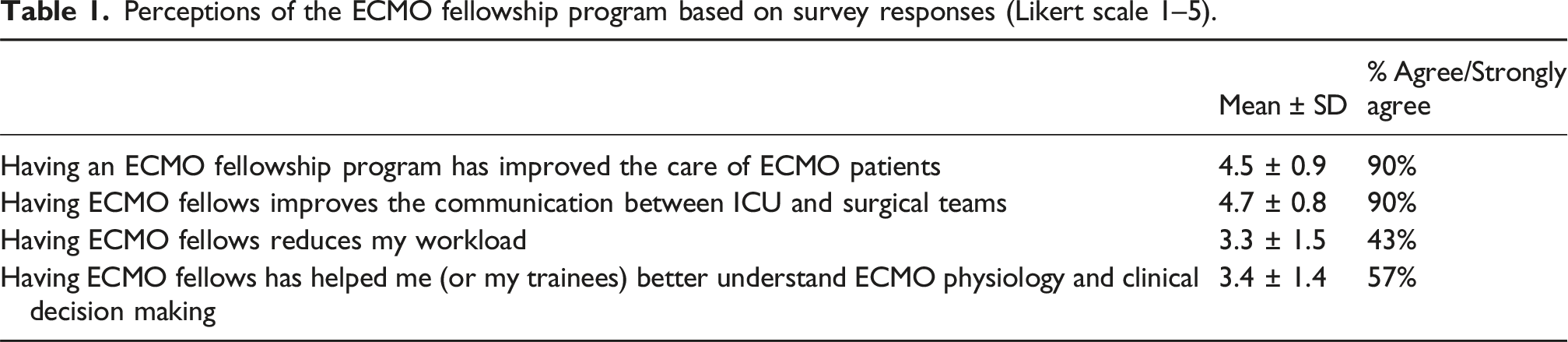
Two fellows completed the program during the study period. Since initiation, annual ECMO runs increased from 59 to 119 (+101%), with total ECMO hours rising 59%. The proportion of patients successfully weaned from ECMO improved significantly in 2025 compared with 2024 (59% vs 41%, χ2 = 6.12, p = 0.013), with a corresponding decline in on-support mortality (22% vs 37%). Two fellows matriculated, each participating in approximately 75 cannulations annually and reporting independent cannulation competency by year-end. Of approximately 70 eligible stakeholders, 30 responded (42%), with most agreeing the fellowship improved ECMO care (90%) and ICU–surgical communication (90%), though fewer endorsed reduced workload (43%). Open-ended feedback emphasized enhanced teamwork and continuity of care.
Conclusions
Early implementation of a dedicated ECMO/MCS fellowship for surgical residents was feasible and associated with increased program volume, improved interdisciplinary communication, and robust trainee experience. Early results suggest potential educational and institutional benefits, warranting longer-term evaluation.
Keywords
Introduction
Since the early 2000s, improvements in ECMO design and management has led to an increase in the use of ECMO, with duration extended from days to weeks and expansion of indications, including bridge to heart or lung transplant, and as periprocedural support for cardiopulmonary interventions.1–4 Landmark studies such as the CESAR trial established the utility of veno-venous (VV) ECMO for management of severe ARDS. 5 International health emergencies have reinforced the utility of this tool with VV ECMO for the management of ARDS skyrocketing during the H1N1 and the COVID 19 pandemics.6,7 National trends have also demonstrated a 23-fold increase in the use of ECMO for cardiogenic shock from 2002 to 2018.8,9 Overall, ECMO is being used more, for sicker patients, and with better outcomes.8,10,11 The increase in ECMO volume would suggest that increased exposure and training is needed for cardiothoracic surgery trainees.
Despite this, formal training or credentialling for EMCO remains inconsistent. Most ECMO cannulations are performed by cardiothoracic surgeons, but this is increasingly being performed by other specialists, including intensivists, cardiologists, and anesthesiologists.12–14 Credentialling requirements vary by institution, although about half of all ECMO centers in the United States do not require any specialized credentialling.15,16 Currently, there is no standardized certification or board requirement for ECMO training in cardiothoracic surgery.6,7 For non-surgeons, the bulk of training is simulation-based and while trainees report increased comfort with procedures following simulation-based training, high-fidelity simulations are resource-intensive, thereby limiting their accessibility.17,18
Concurrently with the increased utilization of ECMO over the past decade, there have been significant shifts in the training paradigms for cardiothoracic surgery. In response to decreasing numbers of applicants in the early 2000s, integrated 6-year training programs and a 4 + 3 model were created, reducing availability of traditional pathways.19,20 Cardiac surgery is no longer a required rotation in general surgery, further limiting early exposure. In this context, a surgical ECMO fellowship for residents on dedicated research time offers an opportunity to gain extensive experience in ECMO and MCS, while simultaneously increasing engagement with the field of cardiothoracic surgery. This study aims to (i) evaluate the impact of implementing a dedicated ECMO/MCS fellowship for general surgery residents on institutional ECMO volume and patient outcomes, (ii) quantify fellows’ clinical contributions through procedural participation and multidisciplinary involvement, and (iii) assess stakeholder perceptions of workflow, communication, and team effectiveness following integration of ECMO fellows.
Methods
Study design and institutional comparision
We conducted a single-center retrospective review at a tertiary academic medical center following the implementation of a dedicated ECMO/MCS fellowship for general surgery residents. Program and institutional outcomes were compared across the pre-fellowship and fellowship eras. To assess the experience of the ECMO fellows, data was collected on number of cannulations performed annually, participation in operative MCS cases (Impella, LVAD, RVAD, transplant), intensive care unit (ICU) procedures including tracheostomy, chest tube placement, wound care, and decannulation, and involvement in organ procurement. ECMO fellows self-reported their experiences. Before implementation of the fellowship, ECMO care was delivered collaboratively by cardiothoracic surgery fellows, surgeons, intensivists, and perfusionist. No dedicated trainee provided continuity across operative and ICU environments.
Fellowship experience
The ECMO/MCS fellowship is a structured year-long clinical and educational program designed to for general surgery residents during dedicated academic time. The curriculum combines formal didactic teaching, high-fidelity simulation and extensive clinical immersion. Fellows complete didactic training covering ECMO physiology, cardiopulmonary pathophysiology, ventilator and hemodynamic management, anticoagulation strategies, and the principles of mechanical circulatory support (Figure 1). Details about the creation and structure of our ECMO fellowship have been published separately.
21
The structure of the ECMO fellowship is shown below. The first year is primarily clinical with the second year allowing more time for scholarly activities. Didactics include completion of an ECMO bootcamp and asynchronous learning during the first 2 months, with recurring didactics continuing through both years. Clinically, the fellows cover the ECMO pager, triaging consults and assisting or performing cannulations and other types of MCS.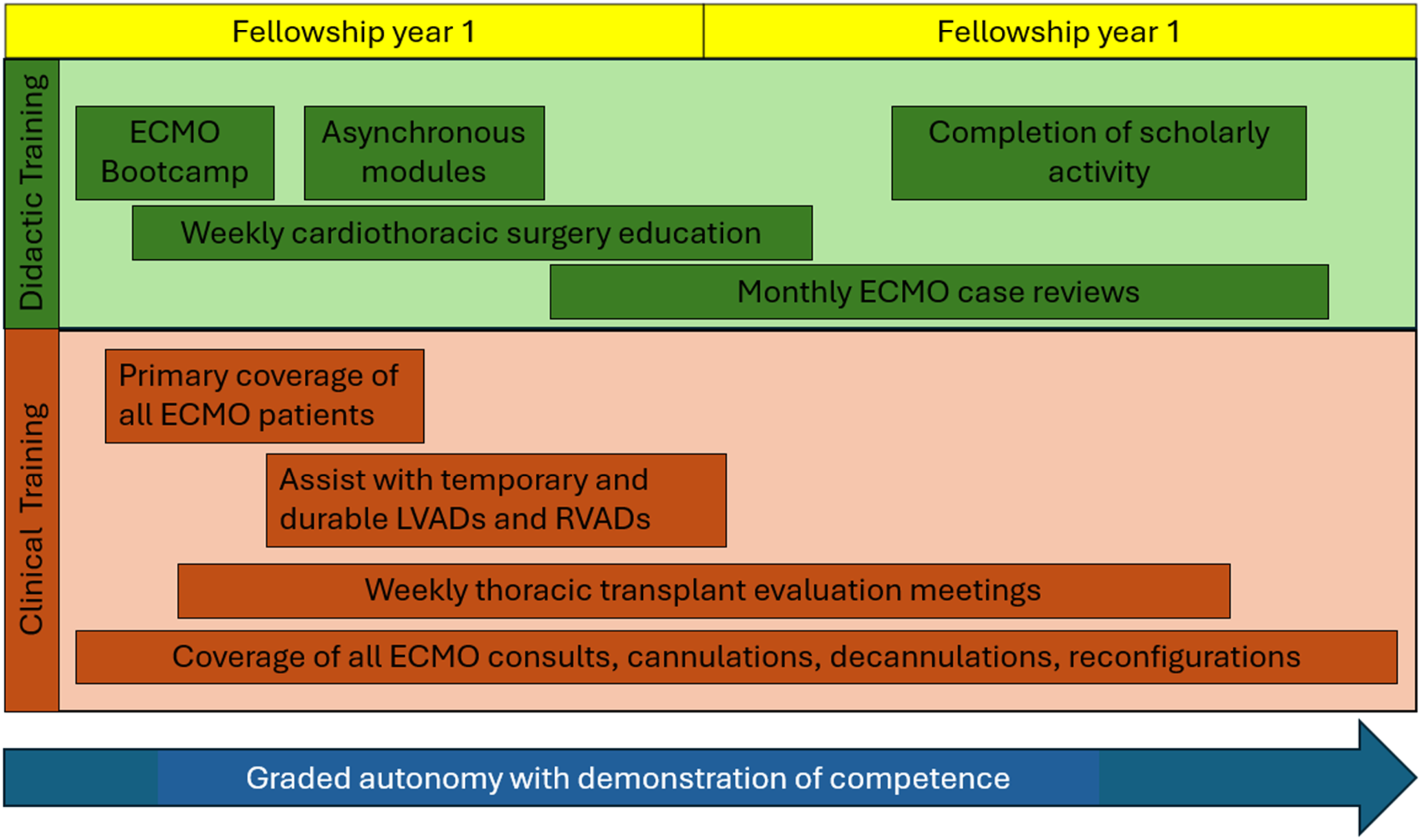
Survey methods
To assess the impact of the fellowship on ICU and operating room teams, a multidisciplinary survey was administered to cardiothoracic surgery faculty and fellows, CTICU providers, perfusionists, and nurses. The survey assessed perceptions of fellows’ impact on communication, workflow, education, and patient care using a 5-point Likert scale. Responses are summarized descriptively (agreement/strong agreement vs neutral/disagreement).
Institutional data was collected retrospectively on mortality trends before and after implementation of the fellowship. This was compared to national trends as reported by the Extracorporeal Life Support Organization (ELSO).
Statistical analysis
Statistical analyses were performed using descriptive and comparative methods. Continuous variables were summarized as means with standard deviations or medians with interquartile ranges (IQRs), while categorical variables were compared using chi-square tests. A p-value <0.0 was considered statistically significant. Analyses were conducted using SPSS (Version 31, IBMO, Armonk, NY).
Results
To date, we have matriculated two residents through our program. Both reported a positive experience, citing substantial grains in managing critically ill patients and a strong foundation in ECMO physiology, patient selection, circuit management, and perioperative care. Feedback from program director evaluations noted significant growth across all core competency domains, including technical proficiency, clinical knowledge, and evidence-based management of complex cardiopulmonary failure. On average, fellows participate in approximately 75 cannulations each year. Fellows self-report comfort with independent cannulation with attending back-up by the end of the first year.
Perceptions of the ECMO fellowship program based on survey responses (Likert scale 1–5).

Survey response from key stakeholders.
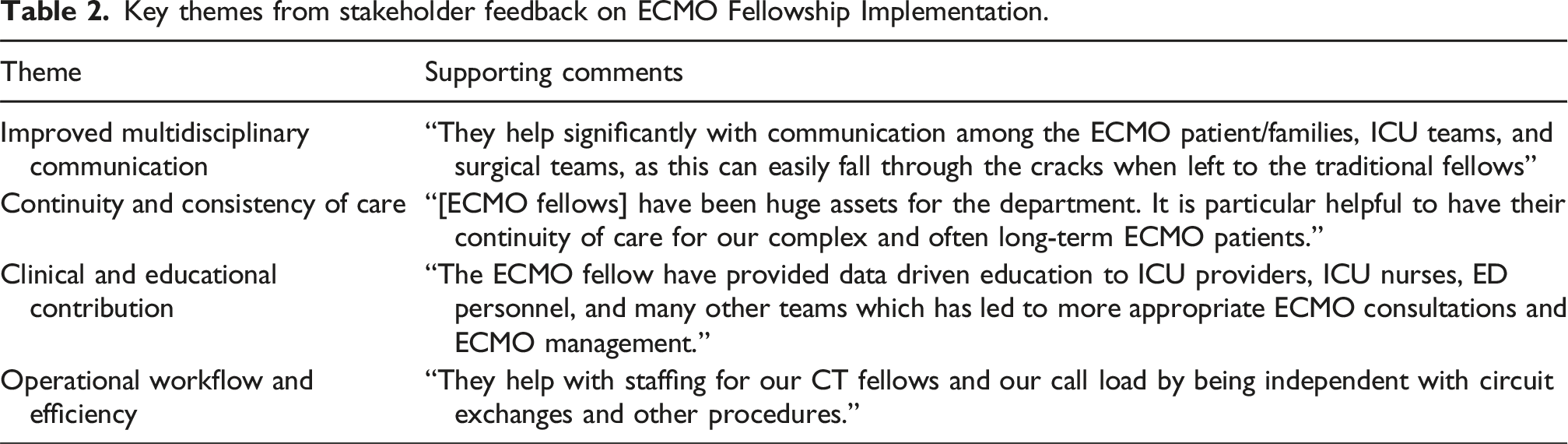
Key themes from stakeholder feedback on ECMO Fellowship Implementation.
Over the same time period, we saw significant program growth. The annual number of ECMO patients increased from 49 patients to 102 patients (108%) and the annual number of ECMO runs increased from 59 runs to 119 runs (101%). ECMO hours increased from 10,353 h to 15,648 h (59%). The proportion of patients successfully weaned from ECMO was significantly higher in FY25 compared with FY24 (59% vs 41%), with a corresponding reduction in mortality on support (22% vs 37%, χ2 = 6.12, p = 0.013). Compared to national ELSO registry data, overall mortality demonstrated a greater degree of month to month to variation but continued a downward trend following ECMO fellowship implementation. From 2020 to 2025, center mortality decreased at rate of 0.0041 per month (R2 = 0.11), compared with a smaller national decline of 0.001 per month (R2 = −040) (Figure 3). Average hospital length of stay increased from 22.8 days in FY23 to 28.1 days in FY24 (+22.8%) and remained stable in FY25 (27.7 days), while median LOS varied minimally (19–21 days), suggesting the observed changes were primarily driven by a small subset of patients with prolonged admissions. Case mix shifted over time, with cardiac support comprising 49% of cases in FY23, 57% in FY24, and 66% in FY25, reflecting a disproportionate growth in cardiac indications relative to pulmonary support (χ2 = 5.19, p = 0.075). Trends in overall ECMO mortality at the University of Colorado compared with national ELSO registry data (2020-2025).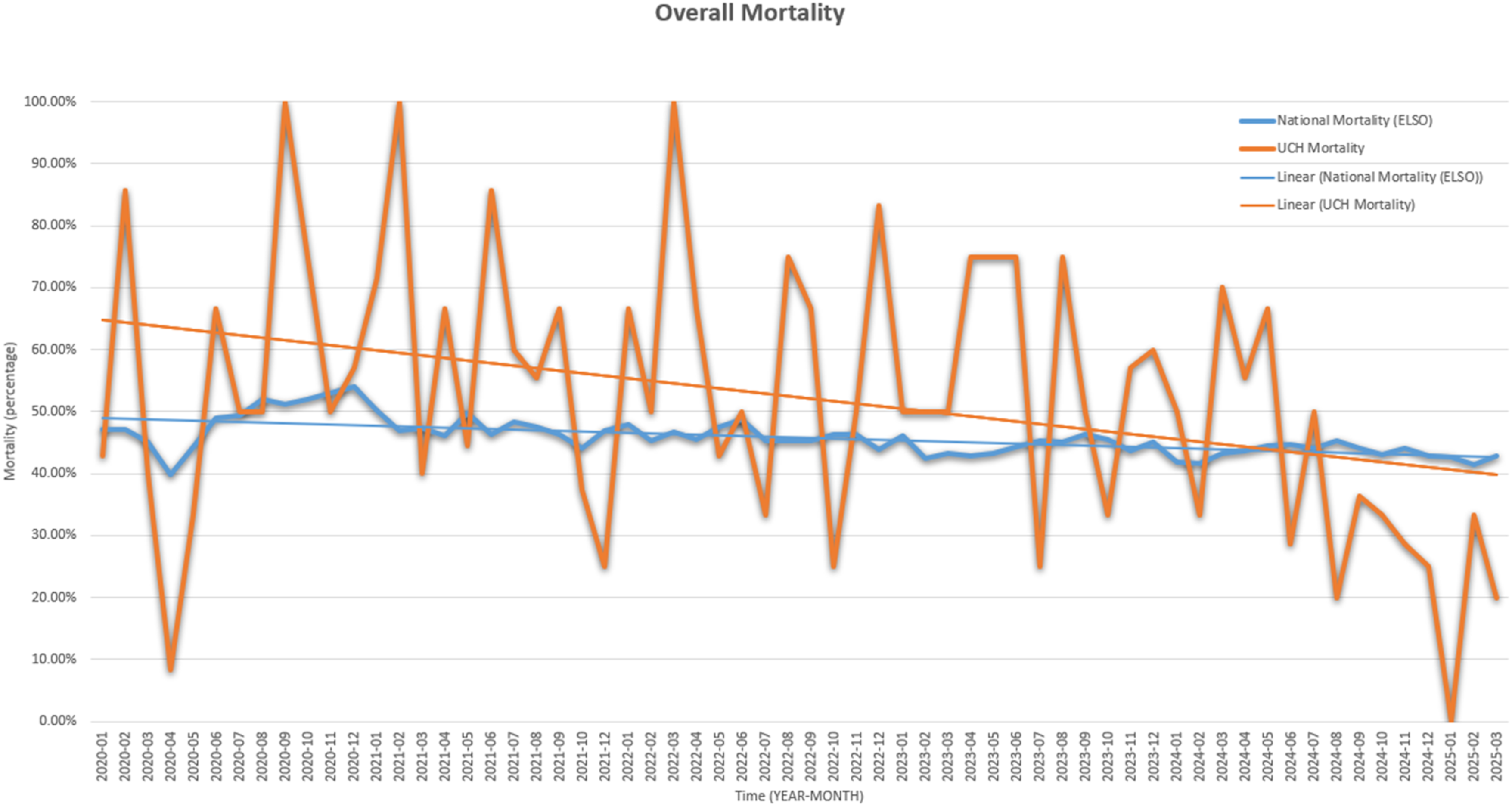
Discussion
Overall, our early experience suggests that an ECMO/MCS fellowship can offer robust clinical training, opportunities for research, and meaningful exposure to cardiothoracic surgery, while simultaneously offering institutional benefit by enhancing care of ECMO patients. We show significant program growth as well as improvement outcomes, although these trends likely reflect multiple concurrent factors. Survey responses indicated perceived improvement in interdisciplinary communication and workload distribution. From an educational standpoint, the fellowship delivers high-yield clinical experience, technical skill development, and structured mentorship. Fellows gain hands-on exposure to ECMO cannulation, troubleshooting, and perioperative decision-making. By participating in operative cases and ICU management, fellows build a foundation in both the technical and cognitive domains of cardiothoracic surgery. Research and quality improvement activities and mentorship further prepare trainees for academic careers. Fellows serve as a consistent point of contact for ECMO-related issues, which enhances continuity of care and fosters collaboration between the ICU, surgical teams, and perfusion. On an institutional level, the program has improved interdisciplinary communication and reduced the workload for traditional cardiothoracic fellows and mid-level providers.
Because this analysis include both experiential educational data and routinely collected institutional ECMO metrics, the findings should be interpreted within the context of these complementary perspectives. Survey responses were incorporated to capture perceptions of workflow and communication, whereas ECMO activity and performance trends reflect program outcomes. Together, these elements provide support of early feasibility rather than definitive causal conclusions.
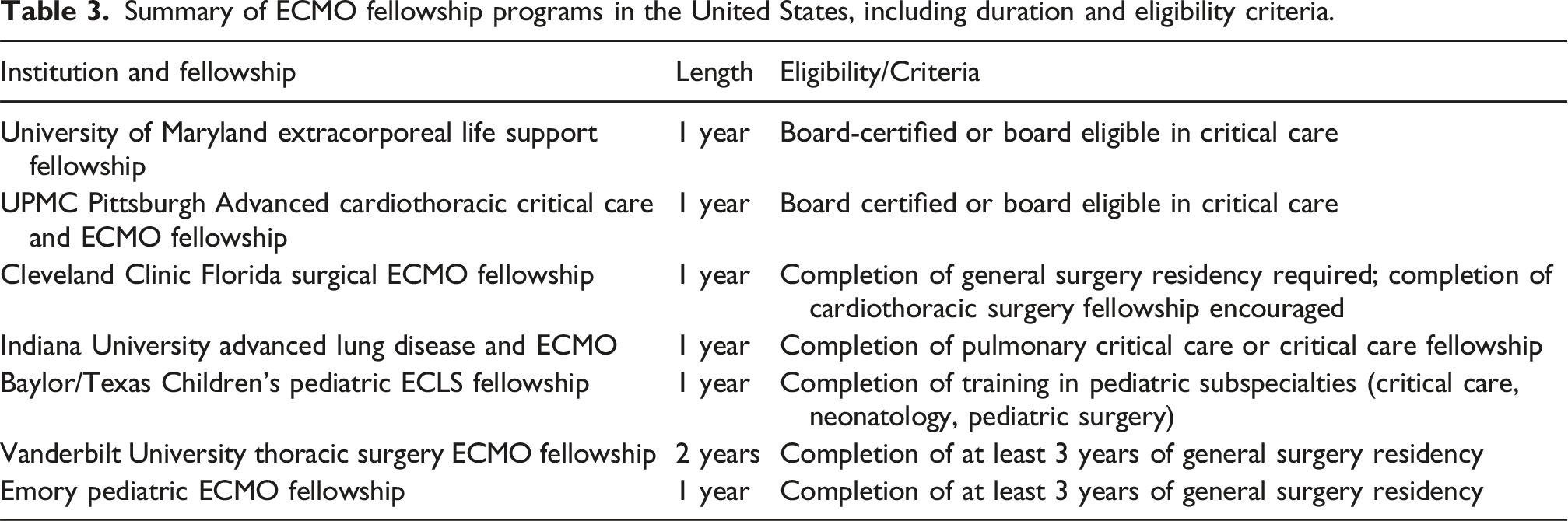
Summary of ECMO fellowship programs in the United States, including duration and eligibility criteria.
This study is not without limitations. Notably, we report very early outcomes in our program with an ECMO fellowship, which limits generalizability and supports interpretation of these findings as early feasibility data.. In addition, positive outcomes in our program, while correlating with the initiation of the fellowship, cannot be definitively attributed to the fellowship program. Although improvements in survival and program volume coincided with the implementation of the fellowship, ICU bed capacity, ECMO staffing models and call structure remained unchanged during the study period. Survey-based outcomes remain outcomes remain subjective and may introduce response bias. Longer term and multicenter evaluation including a larger number of trainees is necessary to determine the broader effectiveness and reproducibility of this training model. We also acknowledge the limited generalizability of this sort of program. While impactful for a high-volume tertiary care center, it is unlikely that there would be role for such a program at lower volume centers.
In conclusion, a structured ECMO fellowship may offer significant educational and institutional benefits. High-volume cardiothoracic programs should consider creating similar programs to provide early exposure in cardiothoracic surgery to general surgery residents, improve education in ECMO and MCS, and enhance institutional care of ECMO patients. Further research is needed to understand longer term impacts of this program.
Footnotes
Author contributions
EJB — Conception and design of the study, data collection and analysis, drafting of the manuscript, creation of figures and tables, and critical revision of all drafts.
TFO — Study conception, supervision of data collection, interpretation of results, and critical revision of the manuscript for important intellectual content.
JRRH— Oversight of study design and implementation, interpretation of institutional outcomes, and critical review of the final manuscript.
MTC— Interpretation of clinical data, contribution to study supervision of the fellowship program design, and critical manuscript revision.
NRT — Senior author; conception and design of the study, , interpretation of findings, and final approval of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.