
Abstract
Extracorporeal membrane oxygenation (ECMO) during cardiac arrest resuscitation (E-CPR) is the last resort therapy in case of refractory cardiac arrest. Despite promising results in intra-hospital cardiac arrest (IHCA), the prognosis of extra-hospital cardiac arrest managed with E-CPR remain controversial, especially in children. We report a rare case of prolonged extra-hospital refractory cardiac after intentional drowning, in a region far from all ECMO center. The child was supported by veno-arterial (VA) ECMO after three and a half hours of CPR. VA ECMO switched to veno venous ECMO on day three. VV ECMO was weaned on day nine. Brain MRI identified a right frontoparietal ischemia and mild hemorrhage. Clinical follow-up 3 years after cardiac arrest showed a mild motor delay with paresis of the left lower limb. This case supports the necessity to take into consideration the possibility to propose E-CPR in refractory cardiac arrest after accidental drowning.
Introduction
Extracorporeal membrane oxygenation (ECMO) is used during refractory cardiac arrest (CA) resuscitation to restore systemic blood flow. While encouraging outcomes have been reported for intra-hospital cardiac arrest (IHCA), the prognosis of out of-hospital cardiac arrest (OHCA) treated with extracorporeal cardiopulmonary resuscitation (ECPR) remains controversial, particularly in pediatric a population. Olson et al. 1 recently published a large analysis from the ELSO database focusing on pediatric OHCA. The overall survival rate was 43% with a significantly better prognosis observed in patients with a primary cardiac and arrhythmogenic reason for arrest. Prolonged E-CPR has been described in cases of accidental hypothermia; reports of cardiac arrest durations exceeding 3 hours are rare.2,3 We report an exceptional case of a prolonged refractory cardiac arrest following drowning in a one-year-old child, successfully managed with ECPR.
Case report
We report a case of a one-year-old child weighing 10 kg who experienced a refractory OHCA following freshwater drowning at 6°C. The drowning occurred in the context of an attempted collective family suicide. The child was retrieved from the water in cardiac arrest (asystole) after 30 min of search activity, corresponding to an estimated no-flow time of 30 min. Bystander conventional cardiopulmonary resuscitation (CPR) was initiated immediately after extraction from the water. Professional CPR was started 10 min later. Tracheal intubation was performed 15 min after CPR initiation. At 17 min of resuscitation, the child developed ventricular fibrillation which was treated by a single external electric shock. The rhythm subsequently deteriorated to pulseless electrical activity. The child was located more than 90 min by road from the nearest ECMO center, and no air medical support was available. The child arrived at the ECMO center after 162 min of CPR. During CPR, he received two boluses of sodium bicarbonate and calcium gluconate, as well as six boluses of epinephrine followed by a continuous infusion at 0.2 µg/kg/min. On admission, the child presented with moderate hypothermia, with a core temperature of 28°C. End-tidal carbon dioxide (EtCO2) monitoring was not available throughout the period of CPR. However, clinical examination revealed spontaneous respiratory movements and preserved pupillary reactivity during CPR. The initial cardiac rhythm on admission was pulseless electrical activity, with a heart rate at 10 per minute. The HOPE score estimated the probability of survival at admission to be 5%.
4
In light of the presence of signs of life during CPR and moderate hypothermia on arrival, extracorporeal cardiopulmonary resuscitation (ECPR) using veno-arterial (VA) ECMO via neck cannulation was initiated. VA ECMO support was achieved 25 min after arrival in the pediatric intensive care unit (PICU), using a 14 Fr venous cannula and a 12 Fr arterial cannula, both from Medtronic® (Figure 1). We used a Deltastream DP7 from Xenios®. Initial ECMO settings included a blood flow of 57 ml/kg/min and a sweep gas flow of 600 ml/min with a fraction of delivered oxygen of 100%. Higher ECMO blood flow could not be achieved due to severe capillary leak syndrome, which required substantial volume resuscitation and limited effective venous drainage. Initial blood gas analysis revealed a pH below 6.8 and lactate level of 11.4 mmol/l, both of which normalized within the first 24 h of ECMO. The first 24 h of ECMO were marked by a severe capillary leak syndrome, requiring massive volume and high-dose vasopressor support. Controlled rewarming was performed using ECMO over 13 h, at a rate of 1°C per hour until 32°C, followed by 0.5°C per hour until normothermia. Acute kidney injury necessitated continuous renal replacement therapy for 4 days. The patient developed severe disseminated intravascular coagulation, which resulted in multiple bleeding sites (gastrointestinal, pulmonary, and cutaneous) and required multiple transfusions of packed red blood cells, fresh frozen plasma, and platelets. On day 1, the patient developed left-sided seizures, which were successfully treated with phenobarbital and phenytoin. After 3 days of VA ECMO, left ventricular function recovered. Ongoing hypoxemic respiratory failure due to massive aspiration and the presence of dual circulation prompted conversion to veno-venous (VV) ECMO. A 14 Fr arterial cannula from Euroset® was percutaneously inserted into the right femoral vein, allowing transition to jugular-femoral VV ECMO. Extracorporeal support was weaned after 6 days of VV ECMO. Neurological assessment revealed an isolatedmotor deficit. Brain magnetic resonance imaging demonstrated a right frontoparietal ischemic lesion associated with a mild hemorrhagic component. Invasive ventilation was discontinued on day 11, and the child was discharged from PICU 17 days after CA. At 3-years follow-up, neurological evaluation showed an isolated mild motor delay, corresponding to a Pediatric Cerebral Performance Category (PCPC) score of 2. The child entered school at the expected age with minimal assistance, primarily related to residual motor impairment. Time line of the cardiac arrest prior ECMO initiation.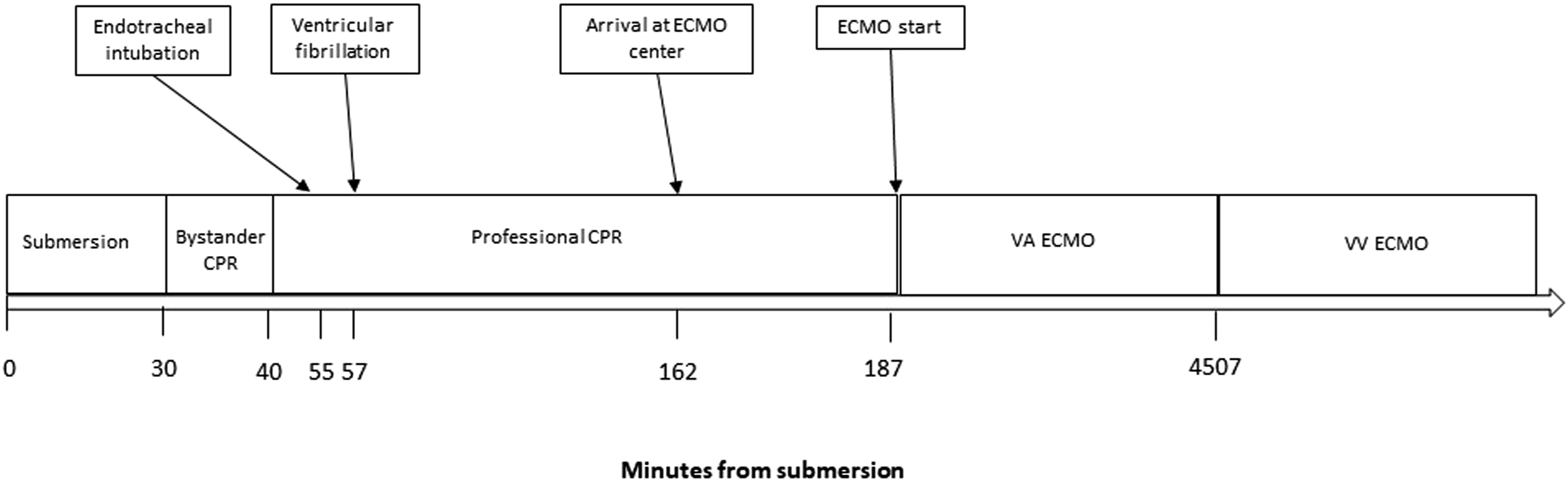
Written informed consent for publication of this case report was obtained from both legal guardians of the child.
Discussion
Out-of-hospital refractory cardiac arrest in children remains a devasting clinical event associated with a poor prognosis. Over recent years, the use of ECMO during cardio-pulmonary resuscitation has increased, with outcomes dependent on the duration of the no-flow and low-flow prior to ECMO initiation, as well as on the underlying etiology of cardiac arrest. While survival after IHCA supported with ECPR has been reported to reach 41 %, 5 a recent analysis from Olson et al., 1 using the ELSO registry reported an overall survival rate of 30% for pediatric OHCA. An initial shockable rhythm was associated with improved outcomes; however, accidental hypothermia was not specifically addressed in this analysis. Recently, ELSO published specific guidelines on the use of ECMO for accidental hypothermia, 6 proposing a structured selection process to identify appropriate candidates for ECMO. This case highlights that favorable survival with acceptable neurological outcome may be achieved despite prolonged cardiac arrest duration when cardiac arrest is associated with accidental hypothermia. Hypothermia-induced reduction in cerebral metabolic demand likely extends the window of reversibility, even in the presence of prolonged low-flow states. In such contexts, cardiac arrest duration alone may be an insufficient criterion to preclude E-CPR. Instead, hypothermia, the presence of signs of life during CPR, and access to timely extracorporeal support in experienced centers should be integrated into decision-making. Our findings support current ELSO recommendations advocating for aggressive resuscitation and extracorporeal rewarming in selected hypothermic cardiac arrest patients, including children. During patient management, our decision-making was partially aligned with ELSO recommendations, particularly regarding accidental hypothermia, cardiac arrest, and the presence of signs of life during cardiopulmonary resuscitation. However, the estimated HOPE score below 5% was less consistent with these recommendations.
In the present case, survival may be partly explained by the high quality of initial CPR. The effectiveness of pre-ECMO CPR is a major determinant of outcome following ECPR. Several studies have demonstrated that resuscitation performed by trained bystanders is associated with improved outcomes compared with CPR initiated by untrained individuals, likely due to earlier recognition of cardiac arrest and higher-quality chest compressions. 7 In addition, simulation-based training programs for emergency medicine and critical care providers have shown to improve team performance, coordination, and technical proficiency during ECMO implantation and resuscitation, and their systematic implementation is strongly encouraged.8–10 Conversely, CPR performed using a “scoop-and–run” strategy may be less effective than resuscitation in a dedicated room, due to vehicle movement and safety constraints. Nevertheless, a recent study from Yates et al. 11 did not identify a significant association between the early hemodynamic parameters obtained during high quality CPR and outcomes, highlighting the complexity of prognostication in prolonged cardiac arrest.
Conclusion
Accidental hypothermia represents a potentially acceptable indication for ECPR for OHCA, even in children.
Footnotes
Author’s note
All authors have not signed an agreement with any sponsor that might compromise the impartial reporting of data.
Ethical considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent for publication
Both parents consent for publication.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.