
Abstract
Background
With improved cardiac surgical outcomes, attention has shifted to patient-centred outcomes, including cosmetic appearances of surgical scars. Minimally invasive cardiac surgery (MICS) is often promoted for its cosmetic benefits, yet empirical evidence remains limited. This study aimed to systematically evaluate scar-specific outcomes comparing MICS to conventional full median sternotomy (FMS) in adult cardiac surgery.
Methods
A systematic review and meta-analysis was conducted following PRISMA guidelines. PubMed, Embase, Central, and Scopus were searched from inception to August 2025. Studies comparing MICS to FMS, reporting scar-related patient-reported outcomes, wound complications, or cosmetic satisfaction, were included. The primary outcome was scar assessment using validated instruments. Random-effects models calculated standardised mean differences (SMD) and risk ratios (RR) with 95% confidence intervals.
Results
Twenty-two studies comprising 3131 patients (1459 MICS, 1672 FMS) met inclusion criteria. MICS demonstrated significantly better scar assessment scores (SMD −0.74, 95% CI −1.27 to −0.22; p < 0.01; I2 = 88%, six studies), higher patient satisfaction rates (RR 1.42, 95% CI 1.21–1.66; p < 0.001; I2 = 84%, 12 studies), and reduced wound complications (RR 0.31, 95% CI 0.20–0.47; p < 0.001; I2 = 0%, nine studies). Only six studies reported validated scar assessment scores, highlighting limited integration of these measures. Substantial heterogeneity was observed due to diverse assessment tools and surgical techniques.
Conclusions
MICS can offer significant advantages in scar-specific outcomes compared to FMS in carefully selected patient populations. Cosmetic outcomes should be interpreted within the context of overall effectiveness and may support shared decision making only when clinical outcomes between surgical approaches are comparable. The lack of standardised scar assessment protocols and limited reporting of cosmetic outcomes represent critical gaps. Future research should prioritise standardised scar evaluation tools and expand cosmetic outcome reporting across all cardiac surgical procedures.
Keywords
Introduction
Within conventional adult cardiac surgery, median sternotomy (MS) has long been established as the gold-standard approach, offering central access to intracardiac structures and accommodating complex procedures.1,2 The evaluation of its success has primarily focused on perioperative outcomes, serving as key quality measures and guiding the adoption of operative techniques. 3 With continued advances in surgical technique, anaesthesia, and patient care, outcomes have improved significantly. In the United States, age-adjusted cardiovascular mortality declined by 56% between 1950 and 1996 (from 307 to 135 deaths per 100,000), 4 and by nearly 75% overall to fewer than 150 deaths per 100,000 by 2023. 5 This decrease has also been observed across other countries, including Australia, Canada, France, and Germany. 5 More recent institutional data indicate a reduction of in-hospital mortality for adult cardiac surgery, falling from 3.3% in 2007 to 1.1% in 2019, 6 reflecting sustained improvements in surgical safety and perioperative management.6,7
With short-term outcomes now less limiting, immediate survival and complication rates are not the sole determinant of surgical success. Instead, attention has shifted towards longer-term, patient-centred dimensions of recovery. Among these, the appearance and impact of surgical scars have gained increasing recognition as important factors influencing patient quality of life across multiple surgical specialties, including cardiac surgery.8,9
MICS offers an alternative approach to traditional median sternotomy, developed to reduce surgical trauma whilst preserving the safety and effectiveness of conventional open heart surgery. Previous meta-analyses and systematic reviews suggest that MICS is associated with reduced perioperative morbidity, shorter intubation and intensive care unit (ICU) stays.10,11 Evidence also indicates that MICS facilitates a quicker return to baseline well-being, although long-term outcomes remain comparable between both approaches. 10 Beyond these endpoints, cosmetic benefit is often cited as an advantage with MICS. 12 Yet, studies specifically evaluating scar-specific patient-reported outcome measures (PROMs) remain limited, meaning the proposed cosmetic advantage is more often assumed than empirically substantiated.
Earlier scar assessment relied on clinician-reported scales such as the Vancouver Scar Scale (VSS), Manchester Scar Scale (MSS), and the Stony Brook Scar Evaluation Scale, offering structured parameters for evaluation, such as vascularity, pigmentation, thickness, and height. However, these tools failed to incorporate the patient’s perspective and often demonstrated variable validity and inter-rater reliability.13,14 To address these limitations, development of the Patient and Observer Scar Assessment Scale (POSAS) broadened assessment protocol by integrating both clinician and patient ratings. 14 Unlike earlier scales, POSAS explicitly captures patient-reported symptoms and perceptions, such as pain, itching, and overall opinion, alongside clinician evaluation of scar morphology, covering both objective and subjective aspects of scarring14. More recently, the Scar Cosmesis Assessment and Rating (SCAR) Scale was introduced in 2016 as a surgery-specific tool for linear post-operative scars, combining clinician scoring with brief patient questions. 15 Collectively, these instruments enable a more nuanced and clinically relevant approach, progressing from clinician-only observations to incorporating patient symptoms and perspectives, establishing a more comprehensive, patient-centred framework to evaluate scar outcomes in MICS.
This study therefore aims to empirically evaluate the cosmetic effect of MICS compared to median sternotomy by synthesising the current evidence on scar-specific outcome measures, either patient-reported or clinician-reported, focusing on validated instruments such as POSAS and SCAR. Other quantifiable outcomes, such as patient satisfaction and wound complications, are also discussed.
Methods
Search strategy and study selection
This systematic review and meta-analysis was conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines 16 and registered with PROSPERO (registration number CRD420251114624).
A systematic search was conducted across PubMed (Medline), Embase, Cochrane CENTRAL, and Scopus from database inception to August 2025. Search terms included combinations of “cardiac surgery,” “sternotomy,” “minimally invasive,” “robotic,” “thoracotomy,” and “scar outcomes,” as well as validated scar tools such as “POSAS” and “SCAR.”
Two independent reviewers screened all titles and abstracts, followed by full-text review of potentially eligible studies. Disagreements were resolved by discussion or referral to a third reviewer. Bibliographies of included studies were also searched for additional eligible articles. Only full-text, peer-reviewed human studies were included.
Eligible studies met the following criteria
(1) (2) (3) (4)
Studies were excluded if they included paediatric patients, urgent/emergent procedures, or did not compare minimally invasive procedures with full sternotomy.
Data extraction and quality assessment
Data extraction was performed independently by two reviewers using a pre-designed spreadsheet. Extracted variables included participant demographics (age, sex), surgical procedure and approach, study design, sample size, and outcomes of interest. The primary outcome was patient-reported scar assessment scores using validated tools. Secondary outcomes included patient satisfaction scores, satisfaction rate, and wound complications. Risk of bias was assessed independently by two authors using the Cochrane RoB-2 tool for RCTs and ROBINS-I for non-randomised studies. Disagreements were resolved by discussion between the joint first authors. Publication bias was evaluated using funnel plot visual inspection and Egger’s regression test where ≥10 studies were available.
The certainty of evidence for each outcome was graded using the GRADE approach across risk of bias, inconsistency, indirectness, imprecision, and publication bias.
Endpoints and subgroup analyses
The primary endpoint was scar assessment using validated PROMs instruments. Secondary endpoints included objective scar characteristics (length, width, area), patient satisfaction scores, satisfaction rate, and wound complication rate. Pre-specified subgroup analyses included: study design (RCT versus observational) and type of minimally invasive approach (mini-sternotomy, mini-thoracotomy, robotic).
Statistical analyses
All analyses were performed using R (version 4.3.4) with the “meta” package. For continuous outcomes (POSAS, SCAR, NRS and other satisfaction scores measures), standardised mean differences with 95% confidence intervals were calculated. For binary outcomes (satisfaction rate and wound complication rate), risk ratios with 95% confidence intervals were calculated. Where necessary, standard errors, confidence intervals, or P values were converted to standard deviations using Cochrane-recommended formulae. When only medians and interquartile ranges were available, means and standard deviations were approximated using established methods.
Study heterogeneity was quantified using the I2 statistic, Cochrane’s Q test, and Tau2. I2 values over 60% were considered significant, and for these outcomes, influential diagnostic analysis was undertaken in R. A random-effects model was used for all analyses to account for anticipated clinical and methodological heterogeneity.
Where ≥10 studies were available for a given outcome, small-study effects and publication bias were assessed using funnel plots and Egger’s regression test. Forest plots were used to visually display effect sizes and heterogeneity.
Results
Study selection and characteristics
The initial search resulted in 2834 records. After removal of duplicates, 1907 unique records were screened, and 92 full-text articles were assessed for eligibility; 22 studies met the inclusion criteria (Figure 1). One study (Nesbitt et al., 2017) lacked sufficient data for quantitative synthesis and was summarised descriptively.
17
PRISMA flow diagram of study screening and selection.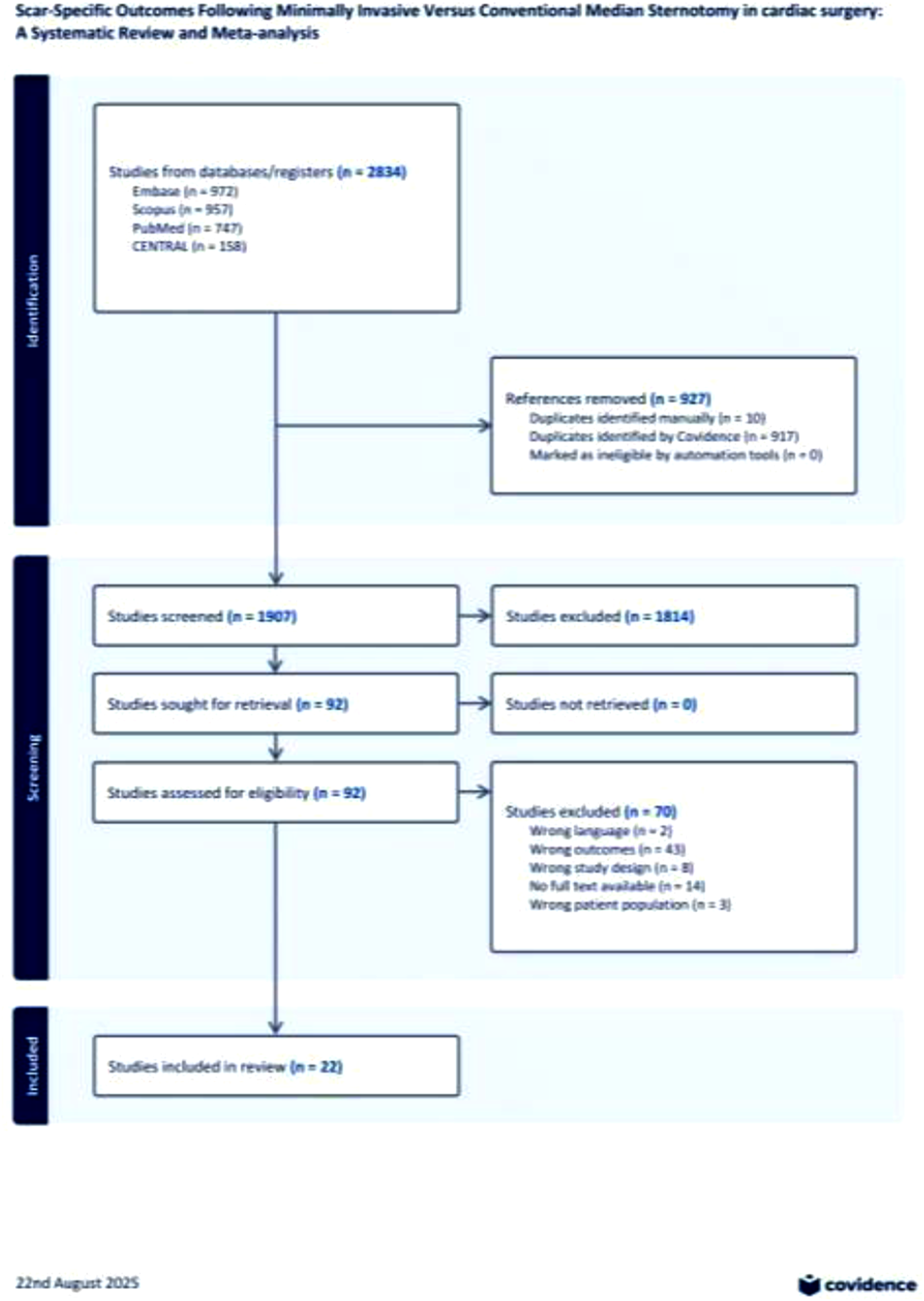
Study characteristics.
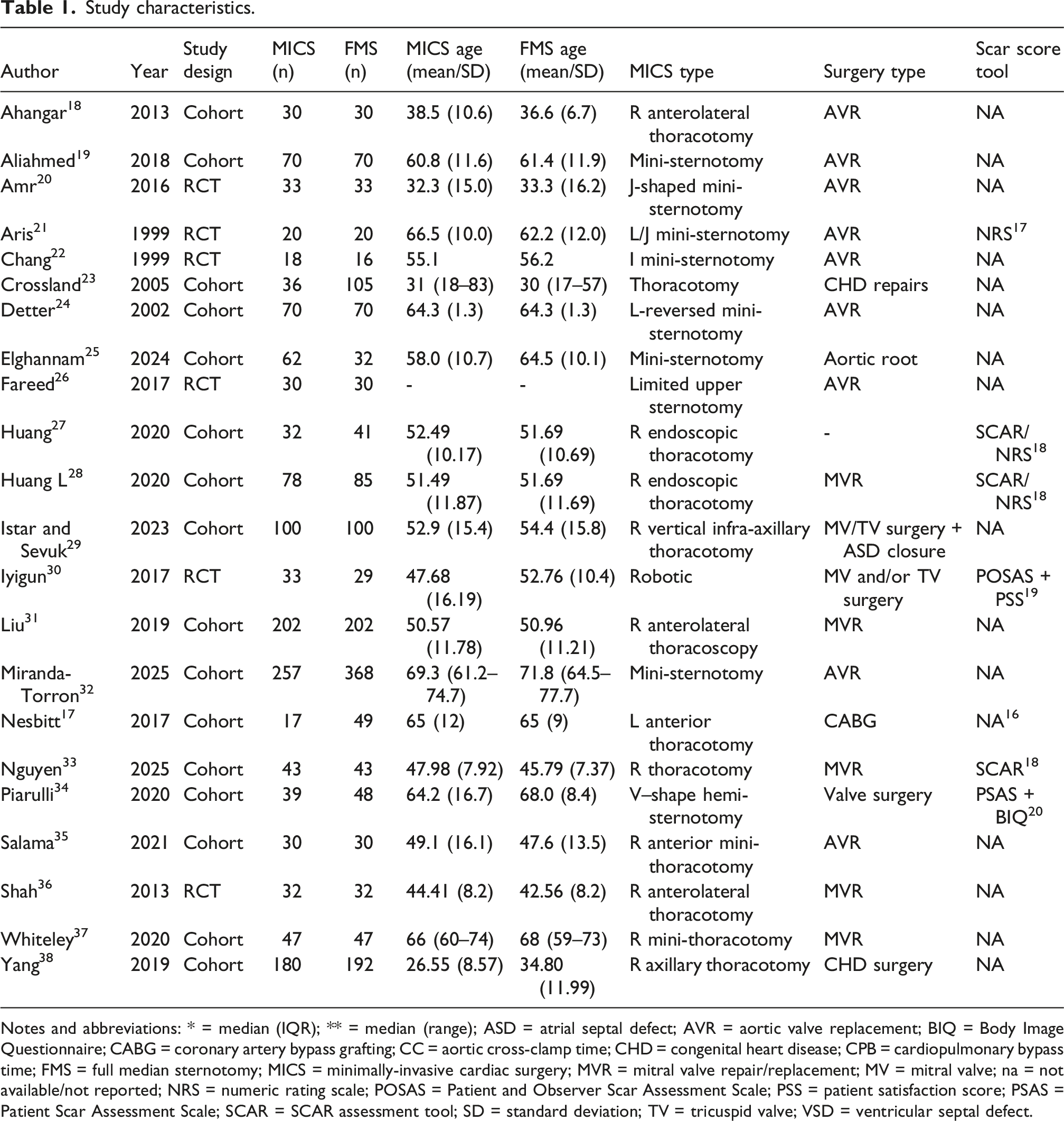
Notes and abbreviations: * = median (IQR); ** = median (range); ASD = atrial septal defect; AVR = aortic valve replacement; BIQ = Body Image Questionnaire; CABG = coronary artery bypass grafting; CC = aortic cross-clamp time; CHD = congenital heart disease; CPB = cardiopulmonary bypass time; FMS = full median sternotomy; MICS = minimally-invasive cardiac surgery; MVR = mitral valve repair/replacement; MV = mitral valve; na = not available/not reported; NRS = numeric rating scale; POSAS = Patient and Observer Scar Assessment Scale; PSS = patient satisfaction score; PSAS = Patient Scar Assessment Scale; SCAR = SCAR assessment tool; SD = standard deviation; TV = tricuspid valve; VSD = ventricular septal defect.
Scar outcomes were assessed with validated instruments: the Numerical Rating Scale (NRS), POSAS, and the SCAR scale. Six studies contributed to scar assessment scores, four to continuous satisfaction scores, 12 to satisfaction rate, and nine to wound complications.
Pooled analysis of outcomes
Scar assessment scores
Our meta-analysis of six studies demonstrated better scar assessment scores with MICS versus full median sternotomy (FMS) on POSAS, SCAR or NRS scale (SMD −0.74, 95% CI −1.27 to −0.22; p < 0.01; I2 = 88%, Figure 2.) An influential diagnostic is carried out in view of the high probability of heterogeneity which showed that the direction and statistical significance were both preserved irrespective of which single study was omitted, with no study shown to have a significant influence on the level of heterogeneity (Supplemental Figure 1). Scar assessment comparison between minimally invasive cardiac surgery (MICS) and full median sternotomy (FMS). Random-effects (Inverse Variance) model. SD = standard deviation; SMD = standardised mean difference. Lower scores indicate better scar cosmetic outcome on POSAS/SCAR/NRS.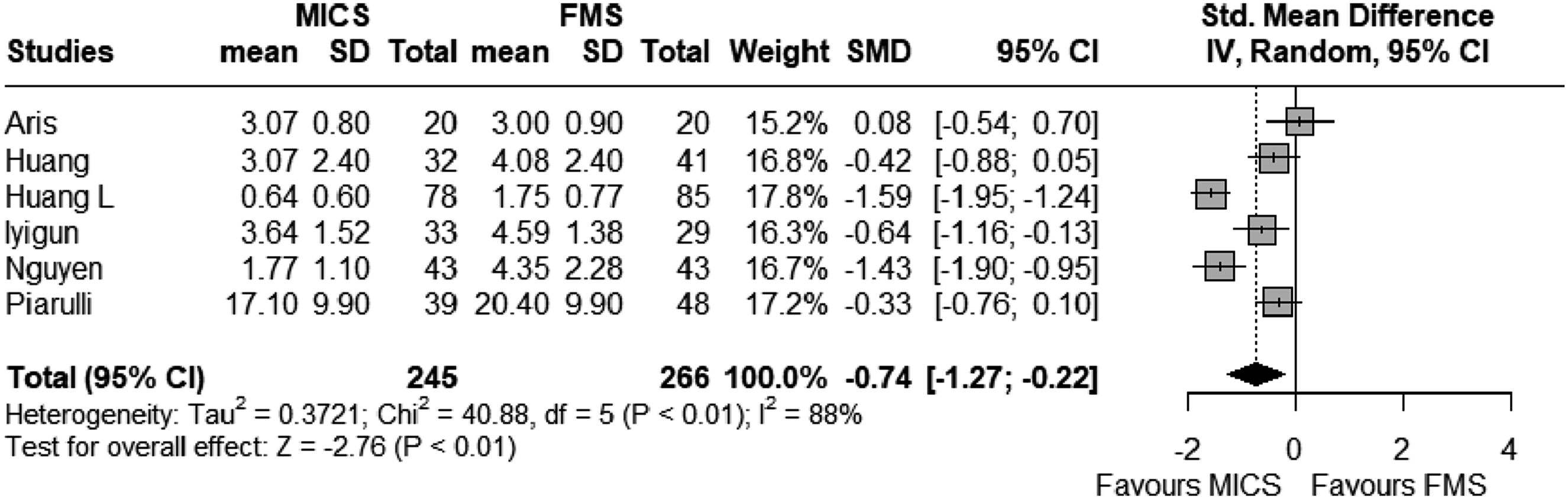
Descriptive analyses of scar aesthetics, satisfaction, and wound outcomes.
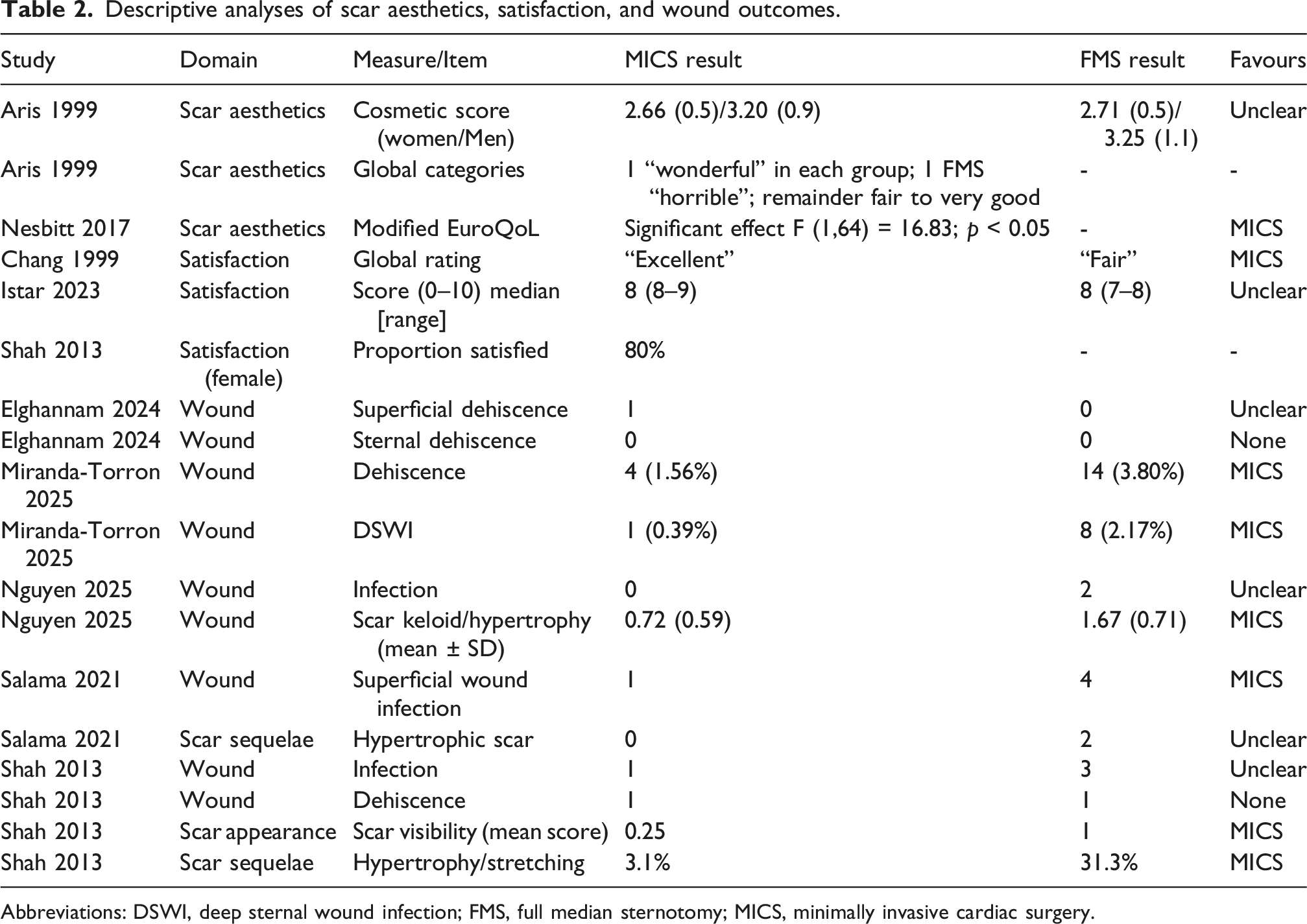
Abbreviations: DSWI, deep sternal wound infection; FMS, full median sternotomy; MICS, minimally invasive cardiac surgery.
Satisfaction rates/scores
Four studies reported satisfaction scores in our systematic review and overall showed a higher satisfaction after MICS compared with FMS (SMD 0.6, 95% CI 0.37–0.83; p < 0.01; I2 = 0%, Figure 3). The tools used to measure satisfaction scores included a 4 point Likert scale (n = 1), scar opinion score extracted from the POSAS data (n = 2), and the “overall impression” category within SCAR assessment (n = 1), Patient satisfaction score comparison between MICS and FMS. Random-effects (Inverse Variance) model. SD = standard deviation; SMD = standardised mean difference.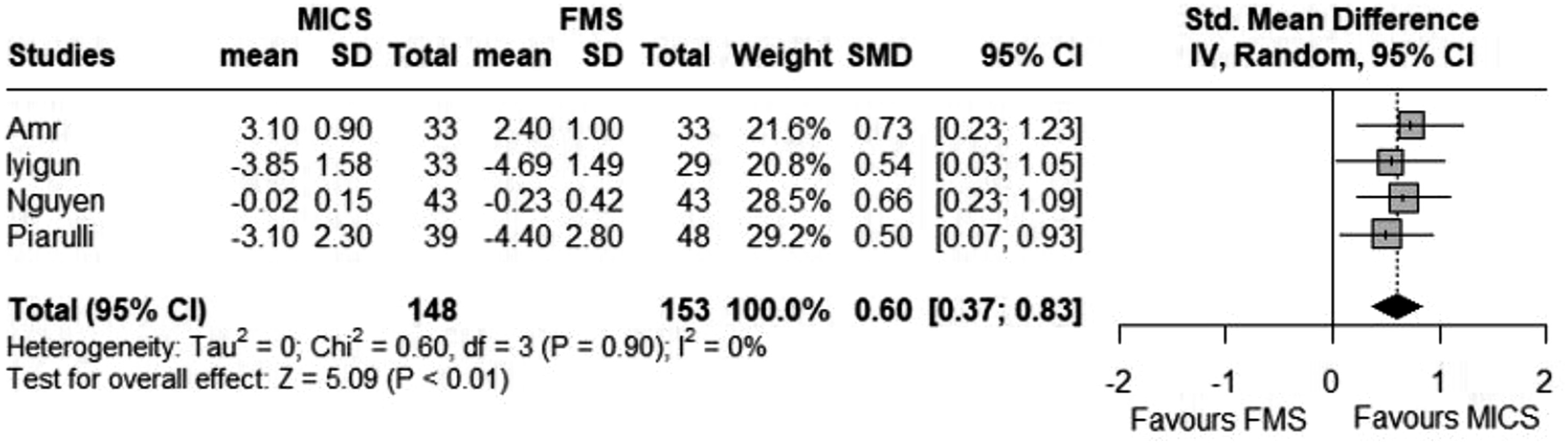
In addition, 12 studies reported satisfaction rate instead of scores. Similarly, they demonstrated that MICS is associated with a higher rate of satisfaction when compared to FMS (RR 1.42 (95% CI 1.21–1.66; p < 0.001; I2 = 84%, Figure 4). Patient satisfaction rate comparison between MICS and FMS. Random-effects model. RR = Risk ratio. MH = Mantel-Haenszel method.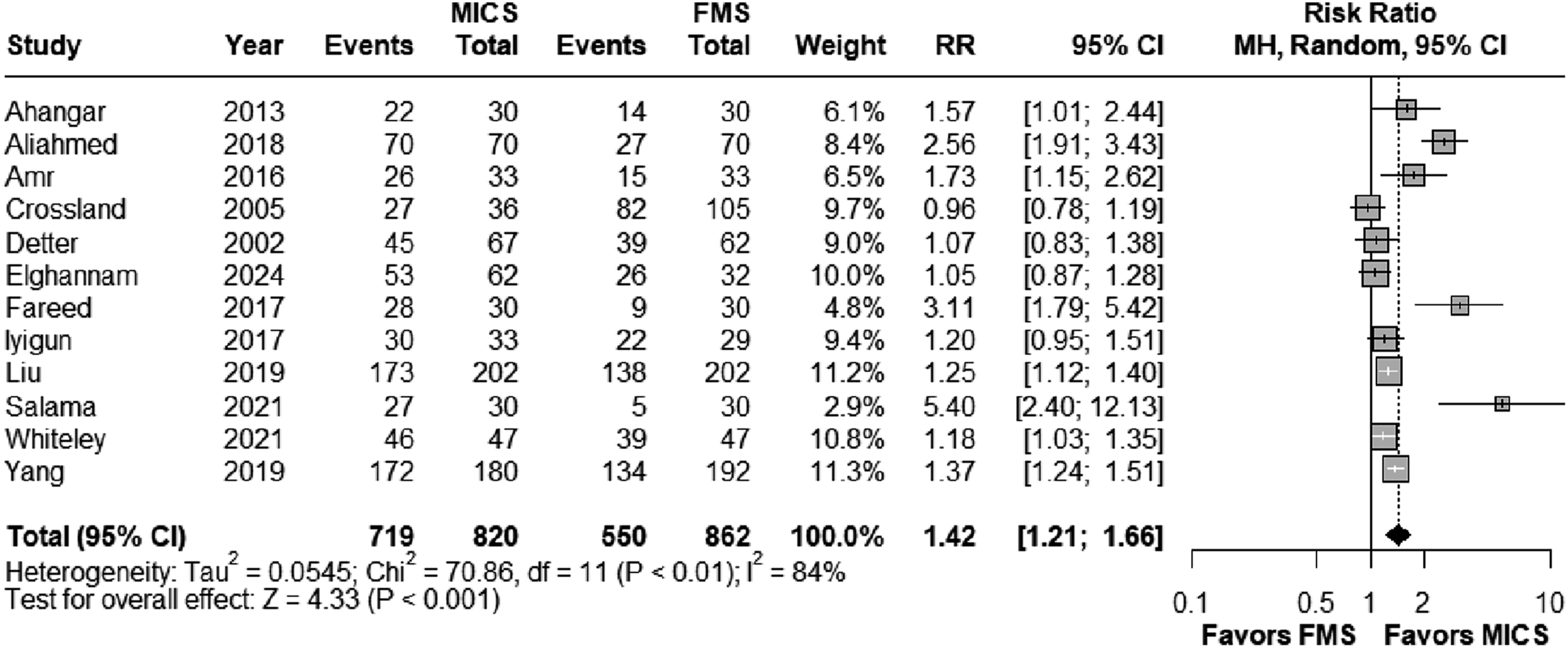
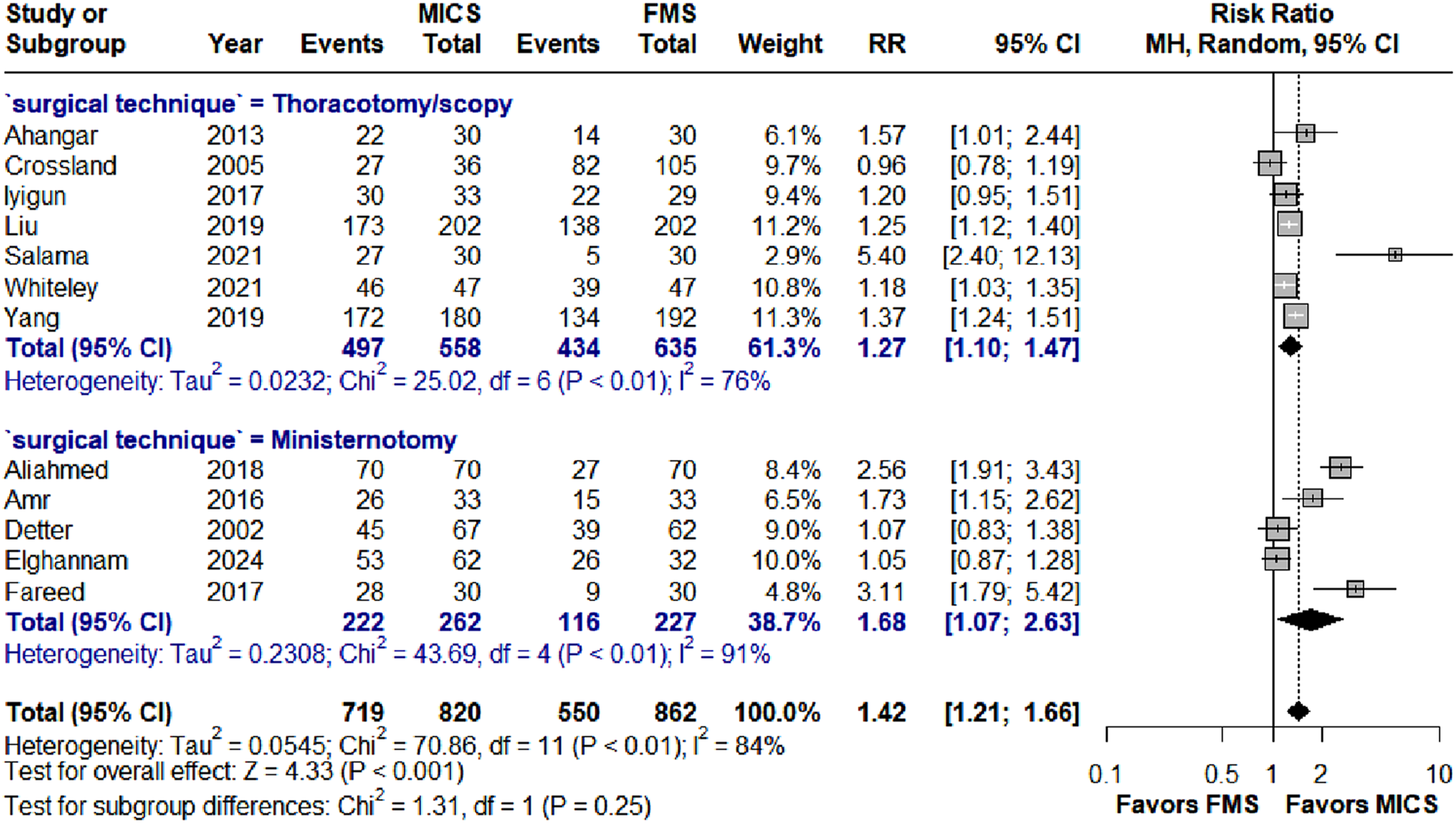
Additional subgroup analyses for satisfaction rate were carried out to determine whether there is any subgroup difference by study design or by surgical approach. Analyses stratified by study design showed consistent outcomes favouring MICS - observational subgroup has a risk ratio of 1.35 (95% CI 1.14–1.60; I2 = 86%) and RCT subgroup has a risk ratio of 1.79 (95% CI 0.99–3.24; I2 = 86%), with no evidence of subgroup difference (p = 0.36, Figure 5). Surgical approaches were categorised into 2 subgroups - ministernotomy or thorocotomy/scopy. Both subgroups favoured MICS - for the thoracotomy/scopy group the pooled effect was RR = 1.27 (95% CI 1.10–1.47; I2 = 76%), while for the ministernotomy group the pooled effect was RR = 1.68 (95% CI 1.07-2.63; I2 = 91%). There was no evidence of subgroup difference (p = 0.25, Figure 6). Satisfaction rate subgroup analysis by study design. Satisfaction rate subgroup analysis by surgical approach.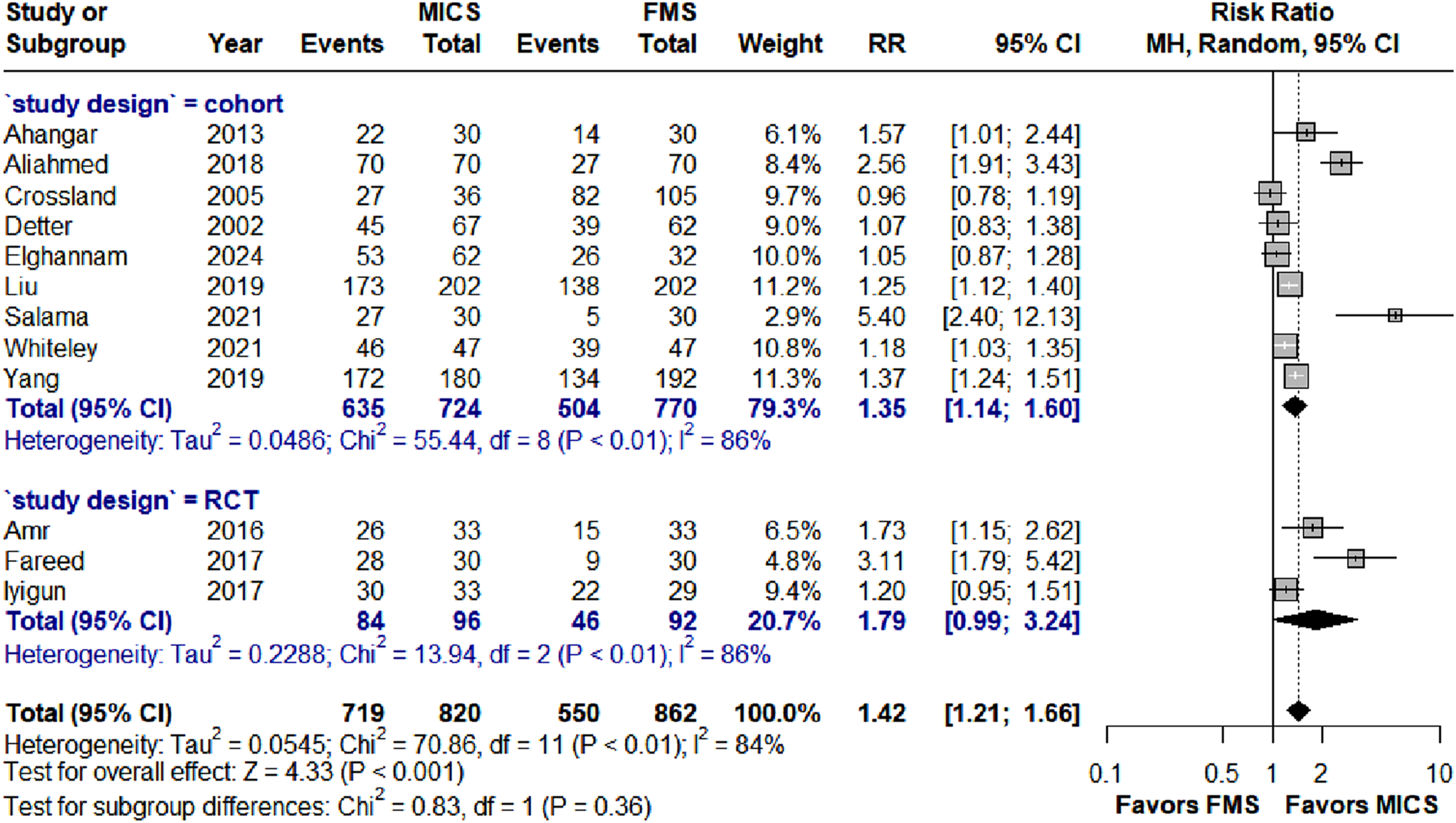
Several studies reported satisfaction outcomes not amenable to pooling and are summarised descriptively. Chang et al. (1999) reported global satisfaction as “excellent” in the mini-sternotomy group versus “fair” after full sternotomy. 22 Istar and Sevuk. (2023) presented median satisfaction scores with ranges - right infra-axillary vertical thoracotomy scored 88,9 versus full sternotomy 87,8,29 Shah et al. (2013) observed 80% satisfaction among female patients in the thoracotomy group. 36 These data are collated in Table 2.
Wound complications
Nine studies reported wound complications in our systematic review and overall showed fewer complications after MICS compared with FMS (RR 0.31, 95% CI 0.20–0.47; p < 0.001; I2 = 0%, Figure 7). The type of wound complications reported include wound infection (superficial or deep), wound dehiscence (superficial or sternal), and hypertrophic/keloid scars. Wound complication rate compared between MICS and FMS. Random-effects model. RR = Risk ratio. MH = Mantel-Haenszel method.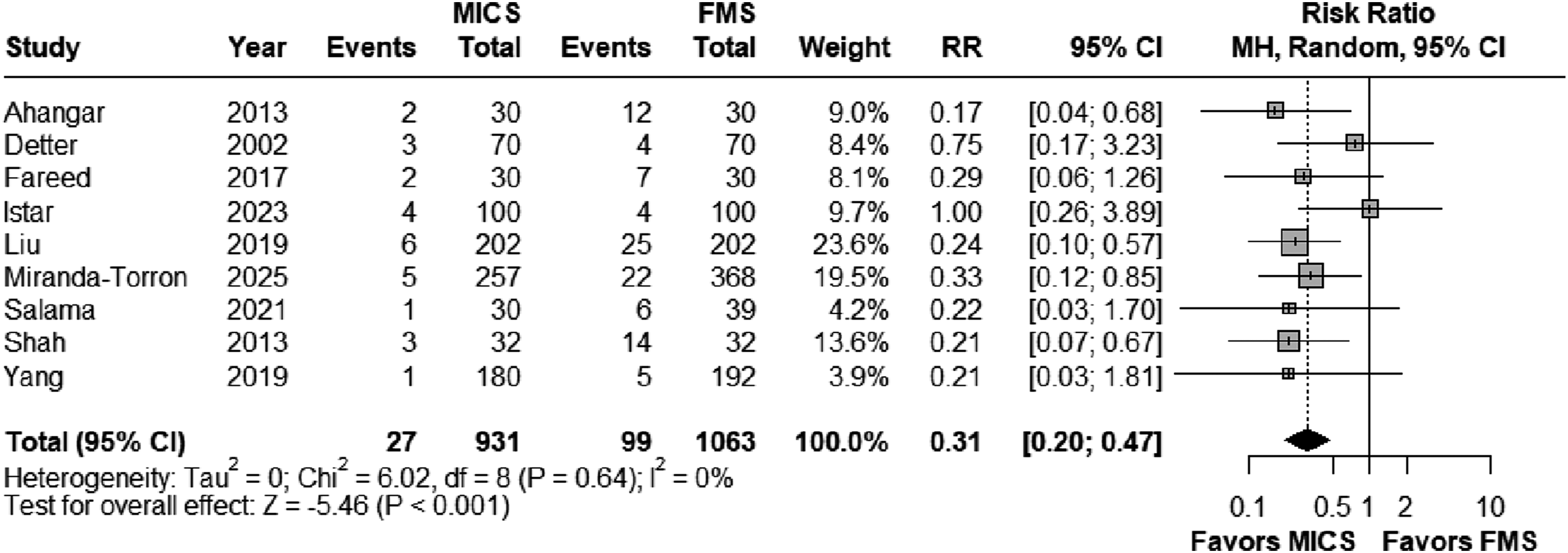
Additional subgroup analyses for wound complications were carried out by surgical approach. Both subgroups favoured MICS - thoracotomy/scopy subgroup showed a risk ratio of 0.27 (95% CI 0.16–0.46; I2 = 0%), and mini-sternotomy subgroup with a risk ratio of 0.38 (95% CI 0.19–0.78; I2 = 0%). There was no evidence of subgroup difference (p = 0.45, Figure 8). Wound complication rate subgroup analysis by surgical approach.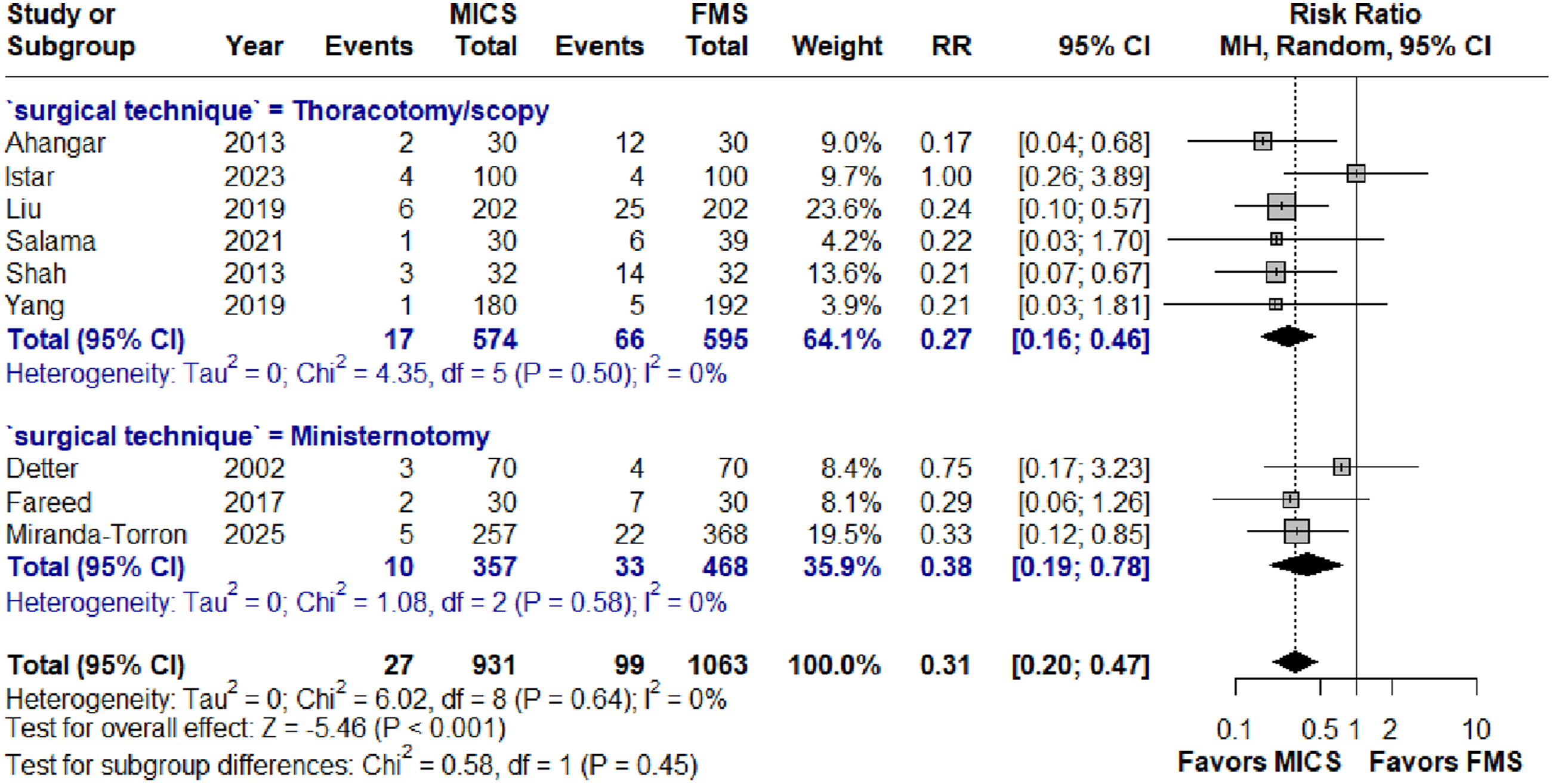
Several studies reported wound outcomes not amenable to pooling and are summarised descriptively. Aris et al. (1999) observed no wound or sternal complications in either group. 21 Elghannam et al. (2024) reported 1 superficial wound dehiscence in the MICS group and 0 in FMS, and no sternal dehiscence in either group. 25 Miranda-Torron et al. (2025) reported 4 cases of dehiscence in MICS (1.56%) versus 14 cases in FMS (3.80%), and 1 deep sternal wound infection in MICS group (0.39%) versus 8 in FMS (2.17%). 32 Nguyen et al. (2025) recorded 0 infection versus 2 and lower SCAR keloid/hypertrophy scores after MICS 0.72 (SD 0.59) versus FMS 1.67 (SD 0.71). 33 Piarulli et al. (2020) found no dehiscence in either group. 34 Salama et al. (2021) noted superficial wound infection in 1 versus 4 and hypertrophic scar in 0 versus 2 between MICS and FMS group. 35 Shah et al. (2013) reported detailed data on wound infection, dehiscence, scar visibility, and scar hypertrophy/stretching. 36 These data are collated in Table 2.
Quality assessment
The Risk of Bias (RoB-2) tool is used to assess the risk of bias in randomised studies included in the paper. Each bias domain is evaluated and discussed between 2 authors (AS, AS) to come up with an overall risk of bias judgment of low risk, some concerns, or high risk (Supplemental Table 1-4).
For non-randomised studies, the ROBINS-I tool (Risk of Bias in Non-randomised Studies – of Interventions) was utilised, and the overall risk of bias judgement is categorised as low/moderate/serious/critical/NI (Supplemental Table 5-7). Additionally, the GRADE checklist was used to evaluate study quality with five domains and scores of “Yes,” “No,” or “Unclear” for each (Supplemental Table 8).
Publication bias
No significant publication bias was detected by visual inspection of funnel plots on all four outcomes (Supplemental Figures 2-5). Egger’s test for satisfaction rate (p = 0.13) and wound complications (p = 0.81) also showed no indication of funnel plot asymmetry, but was underpowered (n < 10) to utilise for scar assessment and satisfaction scores.
Discussion
This systematic review and meta-analysis of 22 studies comprising 3131 patients provides, to our best knowledge, the first comprehensive synthesis of scar-specific outcomes in cardiac surgery. Our study demonstrated that minimally invasive cardiac surgery (MICS) is associated with significantly improved scar assessment scores, higher patient satisfaction rates and reduced wound complications compared to conventional full median sternotomy (FMS). These scar-related benefits can play a role in shared decision-making with patients, but only when core outcomes such as survival and complication rates are equivalent between approaches. However, the substantial heterogeneity and limited use of validated scar assessment tools constrain how confidently these findings can be interpreted, therefore limiting the extent to which cosmetic outcomes alone should influence surgical approach selection. Critically MICS is not universally feasible for all patients. Those with obesity, diabetes, frailty, or anatomical constraints are frequently directed toward FMS, meaning scar-related comparisons must be interpreted with this fundamental selection difference in mind.
Median sternotomy, first introduced by Julian in 1957, has remained the gold standard approach for cardiac surgery due to its excellent exposure and proven long-term outcomes. 39 The safety and efficacy of cardiac surgery have improved dramatically, with in-hospital mortality for adult cardiac surgery declining from 3.3% in 2007 to 1.1% in 2019, reflecting sustained improvements in surgical safety and perioperative management.6,7 With perioperative outcomes increasingly optimised, patient-centred outcomes in the long term, including cosmetic and psychological impact of surgical scars, have been gaining increasing attention. MICS appears to be associated with significant aesthetic differences, which could in turn affect a patient’s psychological wellbeing and overall quality of life, emphasising the clinical relevance of this topic but only when patients are highly selected considering factors such as appropriate anatomy and the correct clinical indication. 34
Importantly, cosmetic and aesthetic outcomes must be considered within the broader context of overall patient care. Although scar appearance and patient satisfaction contribute meaningfully to patient centred outcomes, they should not supersede important endpoints such as mortality, major morbidity or long-term procedural durability. Only when surgical approaches are deemed to have comparable clinical effectiveness, cosmetic outcomes may play a role amongst other factors in guiding shared decision making and reflecting individual patient preferences.
While the summary findings showed a higher scar assessment scores in MICS, it is worthy to notee there there is a substantial risk of heterogeneity in the pooled outcomes of scar assessment scores across studies (I2 = 88%). Furthermore, only six of our 22 included studies reported validated scar assessment scores, highlighting the limited integration of these measures into cardiac surgery research. The studies utilized various assessment tools including the Patient and Observer Scar Assessment Scale (POSAS), Scar Cosmesis Assessment and Rating (SCAR) scale, and Numerical Rating Scale (NRS), each with different scoring systems and validation criteria.
This lack of standardization creates significant barriers to meaningful synthesis and clinical application. The Patient and Observer Scar Assessment Scale (POSAS) is widely used for measurements of scar quality, and recent developments include POSAS 3.0, which incorporates enhanced patient input. 40 However, none of the existing validated scales were specifically developed for cardiac surgery populations, potentially limiting their applicability to sternotomy and thoracotomy scars. The SCAR scale has been successfully applied to evaluate cosmetic outcomes of thoracoscopic cardiac surgery, with satisfactory validity and reliability, suggesting its potential utility in cardiac surgery contexts. 27
The heterogeneity observed likely reflects not only assessment tool diversity but also differences in surgical techniques, patient populations, and follow-up timing. Studies varied considerably in their approach to minimally invasive surgery, including mini-thoracotomy, mini-sternotomy, and robotic approaches, each potentially producing different scar characteristics. Furthermore, the timing of scar assessment ranged from early postoperative periods to long-term follow-up, which is particularly relevant given that scar maturation continues for up to 2 years postoperatively.
Our analysis also revealed that patient satisfaction is significantly higher in the MICS group but once again associated with high risk of heterogeneity (I2 = 84% for satisfaction rates). There are several factors beyond cosmetic outcomes that contribute towards overall patient satisfaction. This aligns with the multifaceted nature of surgical recovery, where scar appearance represents only one component of the patient experience. Patient satisfaction after cardiac surgery is also be influenced by preoperative health, physical recovery, and other postoperative outcomes, indicating the need for more comprehensive assessment approaches. 41
The relationship between wound complications and patient satisfaction represents an important but understudied area. Our findings of significantly reduced wound complications in the MICS group (infection, dehiscence, and hypertrophic scarring) likely contribute to, but do not wholly explain, improved satisfaction scores. These complications are usually associated with prolonged healing, increased pain, diminished quality of life, and poorer cosmetic outcomes. For example, surgical site infections and wound dehiscence have been shown to significantly reduce patient satisfaction and quality of life scores for months after surgery.42,43 Hypertrophic scarring negatively affects patient mental health, self-esteem, and social functioning, with scar severity correlating to patient-reported satisfaction.44,45 Despite this, the current literature largely lacks detailed correlation analyses between specific wound complications and patient-reported satisfaction scores, limiting our understanding of the mechanisms underlying patients’ perceptions. This gap is particularly significant. Establishing the independent contribution of wound complications to patient satisfaction would allow surgeons to identify specific perioperative interventions (including wound closure techniques and infection prophylaxis) that could improve patient-reported outcomes. Future studies should therefore focus on correlation and mediation analyses, for example, investigating whether reductions in infection or dehiscence rates result in satisfaction scores improvements to better determine these relationships. Furthermore, recent studies have demonstrated that improved wound healing interventions not only reduce complications but also enhance cosmetic outcomes and patient satisfaction, reinforcing the clinical importance of minimising wound complications. 46
While the pooled effect size for wound complications showed low risk of heterogeneity, as listed in our table a variety of complications type and rate could be observed across studies, which could be attributed to numerous patient-specific and procedural factors that influence scar formation. Studies have shown that patient characteristics including age, sex, smoking status, diabetes, and genetic predisposition significantly impact wound healing and hypertrophic scar development.13,14 In addition, we should also take into consideration of perception/expectation differences in different population - for instance women may consistently demonstrate greater concern about scar appearance compared to men, as evidenced by the sex-stratified cosmetic scores reported by Aris et al., where women rated worse cosmetic scores in both MICS and FMS groups. 21
Despite clear evidence that fibroproliferative scars disproportionately affect individuals with darker skin, none of the included studies had stratified outcomes for sternotomy scar assessment by Fitzpatrick skin phototype or ethnicity. Fibroproliferative scars are most prevalent in Fitzpatrick types IV–VI, with a demonstrated correlation between higher phototype and increased risk of keloid and mixed scar formation, underscoring an up to 16% incidence among darker skin compared to 0.1% in type I.44,47,48 Yet, original sternotomy cohorts uniformly omitted patient skin phototype and ethnicity from demographic data, precluding analyses of scar outcomes across phototypes. Furthermore, comparisons of minimally invasive versus full sternotomy approaches also ignored skin type, limiting the generalisability of findings to populations at greatest keloid risk. To address these gaps, future studies should collect Fitzpatrick skin phototype (I–VI) and ethnicity data beforehand to evaluate whether less invasive approaches mitigate scar burden in skin of colour. This stratification would ensure that surgical recommendations promote equitable outcomes for all phototypes.
Several studies included in this review reported keloid and hypertrophic scar formation as part of wound complication outcomes, though keloid scars were less frequently documented. Notably, Detter et al. reported keloid formation in two cases within the minimally invasive group, and Shah et al. observed a single keloid case in the sternotomy group.24,36 Pain was a commonly recorded symptom, with multiple studies indicating significantly higher postoperative pain scores in patients undergoing median sternotomy compared to minimally invasive approaches. Itching or pruritus was less commonly reported but was noted in some studies, often with lower intensity in minimally invasive or thoracoscopic groups. These findings highlight that symptomatic evaluation beyond scar appearance, particularly regarding pain and itching, is relatively limited in the existing literature. Given the clinical importance of these symptoms to patient quality of life, further research should aim to systematically assess and report on sensory symptoms associated with keloid and hypertrophic scars.
Surgical technique variations may also contribute to differences in outcomes. Factors such as incision placement, tissue handling, closure methods, and postoperative care protocols can significantly influence scar formation. The learning curve associated with minimally invasive techniques may further contribute to variability in outcomes, particularly in centres with less experience.49,50
Of note, our analysis predominantly included valvular surgery procedures (17 of 22 studies), with limited representation of other cardiac surgeries such as coronary artery bypass grafting (CABG). This raises important questions about the generalizability of our cosmetic findings to minimally invasive CABG procedures. While minimally invasive CABG techniques have demonstrated non-inferiority for clinical outcomes, there is a notable absence of scar-specific outcome reporting in these studies. 11 This lack of cosmetic outcome assessment in other minimally invasive cardiac procedures represents a significant gap, particularly given that some of these procedures often target younger patients (like adult congenital heart surgery, for example) with longer life expectancies who may be particularly concerned about aesthetic outcomes. Future studies examining scar-specific outcomes should aim to include other types of minimally invasive cardiac surgeries to improve generalisability.
Future research could also explore the correlation between scar characteristics and broader quality of life measures, as the psychological impact of surgical scars extends beyond their physical appearance. The development of cardiac surgery-specific scar assessment tools may provide more relevant and sensitive measures than currently available general instruments. Long-term follow-up studies are needed to assess scar evolution and patient satisfaction over time, as initial cosmetic advantages may change with scar maturation.
Limitations
Several limitations constrain the interpretation of our findings. The predominance of observational studies (16 of 22) introduces potential selection bias, as patients undergoing MICS may represent a healthier cohort with different baseline characteristics. In practice, the choice of surgical approach frequently is confounding by the indication. Surgeon preference, anatomical suitability, frailty, and comorbidity burden influence selection, with higher-risk patients, including those with diabetes and impaired wound healing, more often directed toward FMS. Conversely, MICS cohorts tend to represent a healthier, more selected population. These baseline differences may inflate the apparent cosmetic benefits of MICS and underestimate complication risks, limiting causal interpretation. Future studies should report key confounders including age, BMI, diabetes, smoking status, COPD among others and consider propensity-based statistical methods to better adjust for baseline differences. The retrospective nature of most studies limits the ability to establish causal relationships between surgical approach and scar outcomes. Randomised controlled trials directly comparing MICS and FMS focused on cosmetic endpoints are very difficult to conduct. Major barriers include operator learning curve, centre as well as patient preference and crucially, procedural eligibility constraints that preclude many patients from MICS. Therefore, the lack of trial evidence, further emphasises the importance of standardised outcome reporting in observational studies to produce the best available evidence for decision-making. Inconsistent use of validated scar assessment tools across studies represents a critical limitation for evidence synthesis, with only six studies contributing to our primary outcome.
The substantial heterogeneity observed across outcomes likely reflects genuine differences in populations, techniques, and assessment methods rather than statistical artifact. This heterogeneity, while limiting the precision of our estimates, may actually reflect the real-world variation in practice and outcomes across different centres and populations. This is another reason to reinforce the development of standardised protocols for scar assessment, ideally incorporating both objective measurements and patient-reported outcomes, to facilitate more comparisons across studies and surgical approaches. 51
Conclusions
This systematic review provides compelling evidence that minimally invasive cardiac surgery may offer advantages in scar-specific outcomes compared to conventional median sternotomy. These benefits, however, must be contextualised within the reality that MICS is not suitable for all patients. The inherently selected nature of MICS cohorts are typically younger, fitter, and metabolically healthier than the typical patient undergoing heart surgery. Such cosmetic advantages should only be considered in shared decision-making when hard clinical outcomes, including mortality, major morbidity, and procedural durability, are deemed comparable between approaches. Additionally, While minimally invasive cardiac surgery did have higher patient satisfaction rates, this should not be conflated with scar outcomes alone. Patient satisfaction is inherently shaped by a broader interplay of factors including postoperative recovery, procedural experience and overall clinical trajectory. The significant level of heterogeneity in assessment methods and the limited number of studies reporting validated scar outcomes highlight the urgent need for standardized approaches to cosmetic outcome assessment in cardiac surgery. In addition, the absence of stratification by skin phototype and ethnicity represents an important limitation that future studies should address through standardised reporting.
As the field continues to evolve toward patient-centred care, the integration of standardized scar assessment tools and the expansion of cosmetic outcome reporting to all cardiac surgical procedures will be essential for informed surgical decision-making and optimal holistic patient care. The development of cardiac surgery-specific assessment instruments and the establishment of long-term outcome databases will be crucial steps toward achieving these goals. While scar outcomes meaningfully empower patient-centred decision-making, it is important to note they must remain secondary to the clinical outcomes that fundamentally govern surgical safety and effectiveness.
Supplemental material
Supplemental material - Scar-specific outcomes following minimally invasive versus conventional median sternotomy in cardiac surgery: A systematic review and meta-analysis
Supplemental material for Scar-specific outcomes following minimally invasive versus conventional median sternotomy in cardiac surgery: A systematic review and meta-analysis by Karanjot Chhatwal, Anthony On Chun Siu, Sammy Arab, Ahmed Salih, Aishwarya Shah, Arian Arjomandi Rad, Gordon Lap Wai Chong, Monjur Showkat, Sangeeta Punjabi and Prakash Punjabi in Perfusion
Footnotes
Acknowledgments
The authors would like to thank all colleagues and institutional library staff who supported the literature search and retrieval of full-text articles for this review.
Ethical considerations
This study is a systematic review and meta-analysis of previously published studies and did not involve the collection of new data from human participants. In accordance with institutional and national guidelines, formal research ethics committee approval and individual patient informed consent were therefore not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
This systematic review and meta-analysis used data extracted from previously published studies. All data supporting the findings of this work are contained within the article and its supplementary material.
Supplemental material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.