
Abstract
Vasoplegic shock syndrome (VS) occurs in up to 20% of patients undergoing cardiac surgery with cardiopulmonary bypass (CPB) and is associated with increased morbidity rates and poor prognosis. Here, we report a case of severe refractory VS with high aortic-radial pressure gradient following cardiac surgery. A 46-year-old female underwent metal mitral valve replacement, tricuspid valve plasty, and left atrial thrombectomy exhibited refractory peripheral hypotension during rewarming on CPB. Central aortic pressure measurement revealed a significant aortic-radial pressure gradient. By increasing perfusion flow and the administration of vasoactive medications, the aortic pressure gradually normalized but VS still existed, and then weaning from CPB under the guidance of transesophageal echocardiography (TEE). After the patient was transferred to the cardiac intensive care unit (CICU), pulse indicator continuous cardiac output (PICCO) was implanted to guide the maintenance of cardiac function, volume expansion and stable hemodynamics, and the dosage of vasoactive medications was gradually reduced. The patient was discharged on postoperative day 10. A significant aortic-radial pressure gradient was considered an early sign of VS. Early recognition, combined with advanced hemodynamic monitoring and assessment of oxygen metabolism indicators, is crucial for optimizing perioperative management and improving outcomes in patients undergoing CPB.
Keywords
Introduction
Vasoplegic shock syndrome (VS), a perioperative circulatory disturbance, is characterized by a triad of hemodynamic criteria: cardiac index (CI) exceeding 2.2 L/(min·m2), systemic vascular resistance (SVR) below 800 dyne·s/cm5, and persistent mean arterial pressure (MAP) < 60 mmHg despite high-dose vasopressor support (norepinephrine equivalent ≥0.2 µg/kg/min). 1 VS is frequently observed during CPB and affects up to 20% of individuals undergoing cardiac surgical procedures. 2 A higher incidence of this syndrome has been observed in specific patient populations. 2 The occurrence of VS is associated with increased surgical risk and poor prognosis, 3 which adversely affects survival rates, length of hospital stay, and early 30-days readmissions. 4 Although there is no effective method to prevent VS currently exists, a reasonable strategy to identify modifiable risk factors and implementing timely interventions.
Under physiological conditions, pulse pressure is amplified due to the gradual narrowing of peripheral arteries and an increased vascular stiffness, resulting in systolic blood pressure (SBP) in peripheral arteries being higher than in the aorta. When peripheral SBP and MAP are significantly lower than those in the aorta, this phenomenon is called aortic-radial pressure gradient, defined as ΔSBP >25 mmHg and/or ΔMAP >10 mmHg for >5 min. 1 The gradient is relatively common during CPB, with recent literature reporting an incidence of 34% to 45% in the perioperative period of cardiac surgery.5,6 The potential causes include cardiac insufficiency and altered vascular tone. Altered vascular tone encompasses excessive either vasoconstriction or vasodilation, with the latter most commonly associated with vasoplegia under non-physiological perfusion conditions during CPB. 7
Accurate monitoring of both peripheral and aortic pressures is essential for the early identification of the aortic-radial pressure gradient. Once other potential etiologies have been ruled out, this gradient may indicate the initial stages of VS. Such monitoring is crucial for optimal treatment, and thus reducing the risks associated with multiple organ dysfunction and perioperative mortality in patients.8,9 This article reports a case from West China Hospital of Sichuan University involving a patient who experienced an aortic-radial pressure gradient and subsequently developed vasoplegic shock syndrome during cardiac surgery with CPB.
Case description
A 46-year-old female with a 10-years history of exertional dyspnea and fatigue had rheumatic heart disease and pulmonary hypertension with severe mitral regurgitation (MR), severe tricuspid regurgitation (TR), and chronic atrial fibrillation. A preoperative transthoracic echocardiogram showed a left ventricular ejection fraction of 64% and a thrombus in the left atrium. Metal mitral valve replacement, tricuspid valve plasty, and left atrial thrombectomy were scheduled under general anesthesia with CPB.
Combined intravenous-inhalation anesthesia was administered. Following induction, the right radial artery pressure was 112/85 mmHg (mean 94 mmHg). Anesthesia was maintained with a continuous infusion of propofol. During CPB, a routine management was instituted with mild hypothermic CPB at temperatures ranging from 32°C to 34°C, a pump flow rate of 2.4-2.6 L/min/m2, and MAP maintained between 55 and 78 mmHg. During the rewarming period, the radial artery pressure began to decline, ranging from 35 to 43 mmHg. An increase in perfusion flow and the administration of intermittent metaraminol infusions proved to be ineffective.
After aortic unclamping, sinus rhythm resumed spontaneously. Despite an increased perfusion flow rate of 2.96 L/min·m2 and the administration of adrenaline at 0.03 µg/kg/min and noradrenaline at 0.05 µg/kg/min, there was no improvement in peripheral arterial blood pressure, which remained at 51/40 mmHg, accompanied by a progressive increase in lactate levels, rising from 1.3 mmol/L to 5.5 mmol/L. Rewarming was conducted to a temperature of 36.0°C-36.5°C, with warm extremities, and the dosages of adrenaline and noradrenaline were increased to 0.1 µg/kg/min and 0.15-0.2 µg/kg/min, respectively. A femoral artery puncture was performed, yielding a measured femoral artery blood pressure of 99/49 (65) mmHg. The aortic root pressure measurement was recorded at 109/59 (76) mmHg. While the peripheral arterial blood pressure remained very low at 77/56 (63) mmHg. That means a significant aortic-radial pressure gradient occurred (Figure 1). Intraoperative hemodynamic waveforms showing a significant aortic-radial pressure gradient. Radial artery pressure (77/56 mmHg) is substantially lower than concurrent femoral artery pressure (109/63 mmHg), indicating a pressure gradient of >25 mmHg.
Guided by TEE, gradual blood reinfusion and weaning from CPB were performed. After weaning from CPB, an aortic-radial pressure gradient persisted, with radial artery blood pressure at 73/54 (60) mmHg and femoral artery blood pressure at 117/59 (78) mmHg. By the end of the surgery, the total intraoperative fluid administered was 1250 ml,CPB priming solutions 1250 ml,and total urine output was 800 ml. The total operation time was 348 min, total anesthesia time was 418 min, and CPB time was 97 min.
Postoperatively, the patient was transferred to the CICU on continuous infusions of epinephrine (0.03 µg/kg/min), norepinephrine (0.03 µg/kg/min), and vasopressin (0.5 U/h), which had been initiated intraoperatively to treat suspected vasoplegic syndrome. Upon CICU arrival, the blood pressure gradient persisted, with radial and femoral artery pressures of 81/61 mmHg and 139/64 mmHg, respectively.
On the first postoperative day (POD 1), given the ongoing requirement for vasopressor support, a Pulse index Contour Continuous Cardiac Output (PICCO) catheter was inserted for advanced hemodynamic monitoring. At this time, approximately 24 h after the initial vasoplegic event, the PICCO measurements revealed a high systemic vascular resistance index (SVRI) and inadequate fluid status (Figure 2). This hemodynamic profile suggested that the initial low systemic vascular resistance (SVR) state, characteristic of vasoplegia, had been effectively reversed by the ongoing vasopressor therapy. As a result, vasopressin was discontinued, and blood gas analysis was repeated. Postoperative lactate levels peaked at 12 mmol/L. The patient was managed with active rewarming, volume expansion (1025 ml of fluid administered on POD 1), and correction of acid-base disturbances. By POD 2, the lactate level had normalized to 1.3 mmol/L. The dosages of vasoactive drugs were then adjusted based on the patient’s cardiac function and hemodynamic status, leading to a gradual reduction in dosage. The patient was moved to the general ward on POD 5 and was discharged on POD 10. Postoperative day 1 PICCO monitoring data. Systemic vascular resistance index (SVRI: 2486 dyn·s·cm-5 m2) is elevated, suggesting restored vascular tone after vasopressor therapy. Global end-diastolic index (GEDI: 832 mL/m2) indicates relative hypovolemia, guiding subsequent volume expansion.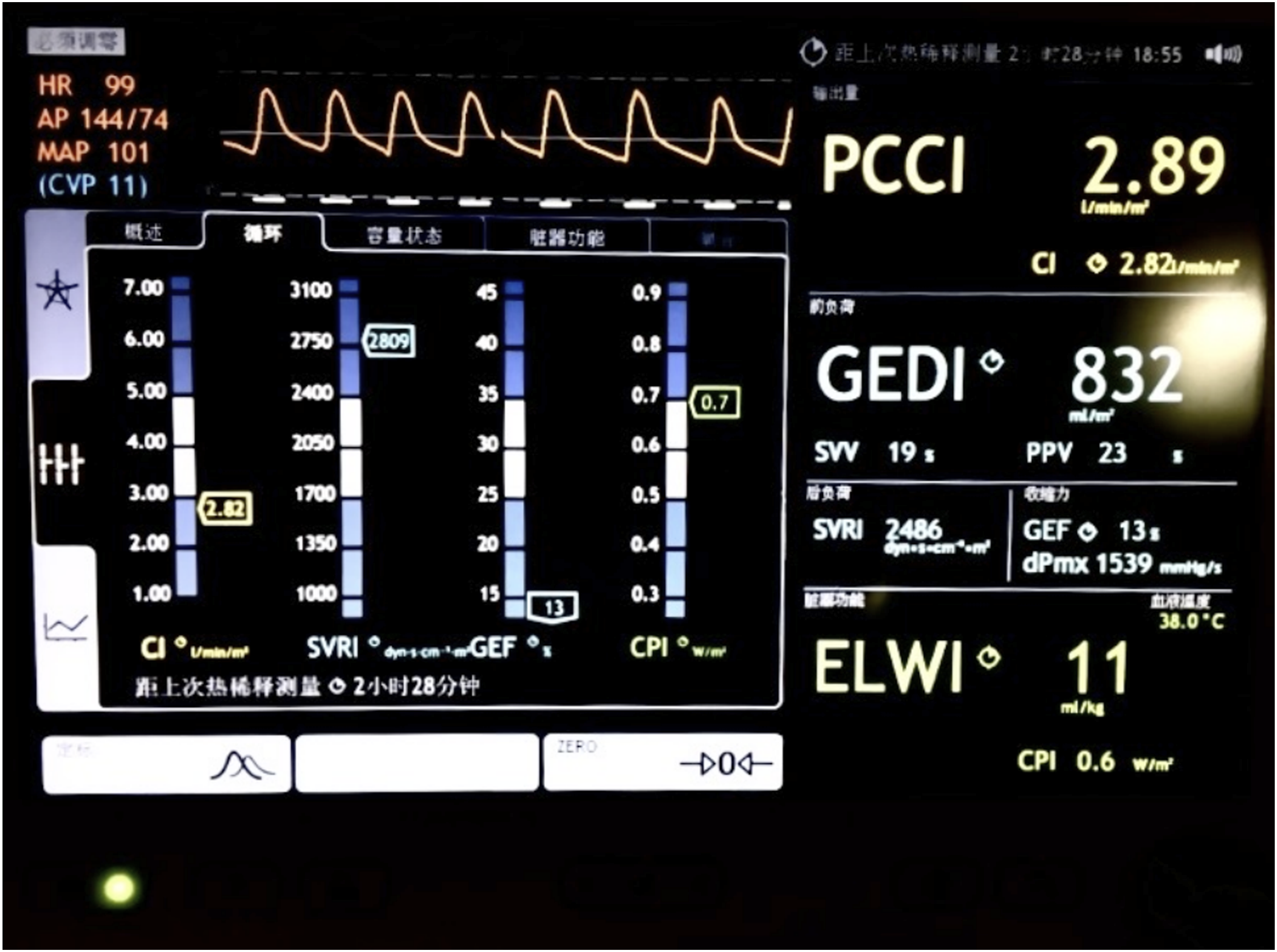
Discussion
The emergence of a significant aortic-to-radial artery pressure gradient during rewarming on CPB in this case highlights a critical limitation of peripheral arterial monitoring. Sole reliance on radial artery pressure may lead to substantial underestimation of true central aortic pressure, potentially prompting inappropriate vasoactive agents administration and complicating separation from CPB.6,10 This case reinforces the principle that peripheral arterial pressure is an unreliable surrogate for central pressure in critically ill patients following CPB 8 . Accordingly, a high index of suspicion for such gradients is warranted, particularly in patients with recognized risk factors including short stature, preoperative hypertension, prolonged bypass and complex surgical procedures.5,6,10 It further highlights the value of early central arterial access (e.g. femoral artery cannulation) for accurate blood pressure monitoring in high-risk populations.
In the present patient, reliance on misleading peripheral readings contributed to a delayed recognition of vasoplegic syndrome (VS). The diagnosis of VS was established immediately upon separation from CPB, based on refractory hypotension despite high-dose vasopressors, warm extremities, escalating lactate levels, and the presence of a significant aortic-radial pressure gradient—all in the absence of hypovolemia, tamponade, or bleeding as assessed by TEE.
Clarification of the temporal relationship between diagnosis and hemodynamic data is essential. The PiCCO catheter was not inserted until postoperative day 1, approximately 24 h after the acute hypotensive event. By this time, the patient had already received significant and sustained doses of multiple vasopressors, including vasopressin. Therefore, the findings of high systemic vascular resistance index (SVRI) and relative hypovolemia on PiCCO (Figure 2) do not represent the initial hemodynamic profile of VS, which is characterized by high cardiac output and low SVR1,11–13 . Instead, they reflect the post-resuscitation hemodynamic status following prolonged vasopressor support. This distinction is crucial for correct data interpretation: the delayed PiCCO data, while not capturing the pathognomonic low SVR state at onset, proved invaluable for guiding subsequent management. By demonstrating that SVR had been restored (likely due to vasopressin), it allowed for vasopressor de-escalation and highlighted the need for volume expansion to treat prevailing hypovolemia.
Advanced hemodynamic monitoring platforms, such as PiCCO, offer integrated, real-time assessment of cardiac function, volume status, and SVR, facilitating rational, goal-directed therapy. In any patient with suspected VS, therapeutic decisions should be guided by serial assessment of tissue oxygen metabolism, including mixed venous oxygen saturation (SvO2), central venous oxygen saturation (ScvO2), serum lactate, and the veno-arterial carbon dioxide gradient (Pv-aCO2). 14 This case underscores that when peripheral arterial monitoring proves unreliable, the integration of central aortic pressure measurement with comprehensive hemodynamic data is essential for accurate diagnosis and optimal perioperative management of vasoplegic shock. Furthermore, it highlights that the timing of advanced monitoring relative to the clinical event is paramount for correct data interpretation—clinical judgment remains the cornerstone of diagnosis during the acute phase, and even delayed hemodynamic assessment can provide critical information for optimizing ongoing care.
Conclusion
In conclusion, a significant aortic-radial pressure gradient can serve as an early clinical indicator of vasoplegic syndrome during cardiac surgery with CPB. Timely recognition of this gradient, combined with early central hemodynamic monitoring and assessment of oxygen metabolism, is essential for guiding perioperative management and improving patient outcomes.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by medical research funding from Science and Technology Department of Sichuan Province (2024YFFK0253).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.