
Abstract
Objectives
In acute type A aortic dissection (ATAAD) surgery requiring hypothermic circulatory arrest (HCA), substantial variation persists in cooling strategies, and the optimal target temperature before circulatory arrest remains debated. The objective of this study was to evaluate clinical outcomes associated with different hypothermia strategies in ATAAD surgery performed under HCA with antegrade cerebral perfusion (ACP).
Methods
This review followed PRISMA guidelines and a registered PROSPERO protocol. Comprehensive database searches identified comparative studies of hypothermia levels during ATAAD repair with ACP. After screening and quality assessment, data were extracted for meta-analysis using random-effects modeling, evaluating mortality, postoperative stroke, and the need of postoperative dialysis.
Results
The search yielded 11 eligible studies comprising 5996 patients. Most were observational and assessed mild–moderate temperature strategies. Meta-analysis showed reduced mortality and dialysis with warmer hypothermia, while the rates of postoperative stroke were similar. Heterogeneity was low except for postoperative dialysis, and publication bias was minimal to moderate across outcomes.
Conclusion
Across all evaluated outcomes, deeper hypothermia did not demonstrate superiority over warmer strategies regarding in-hospital mortality, postoperative stroke, or acute kidney failure requiring dialysis. A definitive optimal temperature threshold for ATAAD surgery requiring HCA and ACP remains to be established.
Introduction
The use of hypothermic circulatory arrest (HCA) remains essential in emergency surgical repair for acute type A aortic dissection (ATAAD). 1 Hypothermia decreases the metabolic demands of vital organs, prolonging their tolerance to ischemia and helping to preserve cellular and tissue integrity during interrupted blood flow. 2
Traditionally, deep levels of hypothermia have been used in cardiothoracic surgery to maximize this protective effect.1,2 However, with the increasing adoption and refinement of antegrade cerebral perfusion (ACP) techniques, many cardiothoracic surgical centers have moved toward a more liberal approach to hypothermia during aortic arch repair. The rationale for this shift includes evidence suggesting that higher target temperatures may reduce the time required on cardiopulmonary bypass for rewarming, diminish perioperative coagulopathy, and potentially contribute to improved overall clinical outcomes.3,4
ATAAD patients, however, present a wide spectrum of physiological and hemodynamic challenges that distinguish them from patients undergoing elective repair for isolated thoracic aortic aneurysms. In ATAAD, malperfusion syndromes involving cerebral, coronary, mesenteric, spinal, or limb vascular territories are often present and may entail stroke, hemodynamic shock, paraplegia or end-organ ischemia. 5 These physiological stressors may influence the optimal degree of hypothermia required to balance cerebral protection, organ preservation, and operative efficiency. Consequently, the target temperature for hypothermic management during ATAAD repair may differ significantly from that used during elective aortic surgery managed with HCA.
Existing literature has suggested that moderate hypothermia, typically defined as temperatures between 20 and 28°C, when combined with ACP, appears to offer superior outcomes compared to traditional deep hypothermia (<20°C) in the context of aortic arch surgery. Studies have demonstrated reductions in neurological complications, particularly stroke, as well as decreased in-hospital mortality with moderate hypothermic strategies. 4 These findings suggest that, with effective cerebral perfusion strategies such as ACP, moderate hypothermia may provide an optimal balance between organ protection and reduced procedure-related morbidity. Therefore, a comparison with deeper levels of hypothermia is now warranted, to help establish an evidence-based clinical practice.
The primary aim of this meta-analysis was to compare in-hospital mortality between two levels within moderate to mild hypothermia in ATAAD surgery performed under HCA with ACP. The secondary aim was to compare the incidence of postoperative stroke and postoperative dialysis, between the same groups.
Materials and methods
This content was reported according to PRISMA guidelines for systematic reviews. 6 The study protocol was registered in the International Prospective Register of Systematic Reviews in Health and Social Care (PROSPERO) (CRD420251234915) on the 18th of November 2025.
Search strategy
A literature search was performed in the following databases: Medline (Ovid), Embase (embase.com), Web of Science (Clarivate Analytics), Google Scholar (publish or perish). The last search was conducted on the 11th of September 2025.
The search strategy was developed in Medline (Ovid) in collaboration with on-site librarians from the Karolinska university library. For each search concept Medical Subject Headings (MeSH) terms and free text terms were identified. The search was then translated, in part using Polyglot Search Translator, 7 into the other databases. No language restrictions were applied. Databases were searched from inception. The strategies were peer reviewed by another librarian prior to execution. De-duplication was performed using Covidence. The full search strategies for all databases are available in Supplemental Table S1-S4.
Inclusion criteria
We included all peer reviewed cohort or randomized control studies comparing clinical outcomes after ATAAD surgery with ACP as neuroprotective strategy, ranging from 2010 until present, with different levels of hypothermia as the exposure. The levels of hypothermia were: moderate (20-28°C) to mild (>28°C) or low-moderate (20-24°C) to high-moderate (24.1-28°C), according to the 2023 writing committee consensus on hypothermic classification in aortic surgery.4 4 ATAAD was, as previously stated, 8 defined as a dissection that is diagnosed within 14 days after onset of symptoms.
Exclusion criteria
Abstracts, case reports, conference presentations, editorials, reviews, expert opinions or animal studies were not included, along with studies including pediatric populations. Studies using retrograde cerebral perfusion or no cerebral perfusion were also excluded.
Data extraction
Data and study characteristics from the included studies were independently extracted by two investigators (EB and MS) using separate, structured data collection forms to ensure methodological rigor. Any discrepancies identified during the extraction process were resolved through consensus. Extracted variables included the first author’s name, year of publication, study period, country of origin, definition of hypothermia, total sample size, the number of patients in the exposed and non-exposed groups and the number of patients in each group who developed the outcomes of interest.
Quality assessment
The Newcastle–Ottawa Scale (NOS) was used for quality assessment; it is specifically developed to assess the quality and risk of bias in observational studies. 9 NOS is based on a “star system”, whereby a study is rated according to three perspectives: the selection of exposed and non-exposed participants (maximum four stars), the comparability of the group (maximum two stars), and the assessment of outcomes (maximum three stars). The highest quality studies are awarded nine stars. For randomized control studies, the Cochrane risk-of bias tool (RoB 2) 10 was used to assess quality. Two reviewer authors (EB and MS) assessed the quality of the selected studies. Disagreements were resolved by consensus, with a senior reviewer (MS) acting as arbiter when necessary.
Outcomes
The primary outcome was in-hospital mortality, including intraoperative mortality.
Secondary outcomes were postoperative stroke and postoperative dialysis.
Statistical analysis
Unadjusted ORs were extracted from the selected articles by calculating raw data. To consider the clinical diversity and methodological variation among the studies, the random effects model was used to calculate the summary statistics and their 95% confidence intervals (CI). Results of meta-analyses were displayed in forest Plots, where exposure was defined as being subjected to the warmer definition of hypothermia for each study. Publication bias was assessed through the visual examination of a funnel plot and Egger’s test. Patient and procedural characteristics for all studies were described as frequencies for categorical variables and mean values for continuous variables, comparing the lower and higher temperature target for each study and were named “cold” and “warm” in the table. Student's t-test was used for continuous variables when comparing groups. Data management and statistical analyses were performed using R version 4.1.2 (R Foundation for Statistical Computing) with the metafor package. 11 P-values below 0.05 were considered statistically significant.
Results
Literature search process
A total of 6641 articles were identified in the literature search, and after 2848 duplicates were identified and discarded, 3793 remained. Finally, 11 studies remained after 126 abstracts had undergone assessment for eligibility. A flow chart of the screening process is shown in Figure 1. PRISMA Flow chart of search strategies.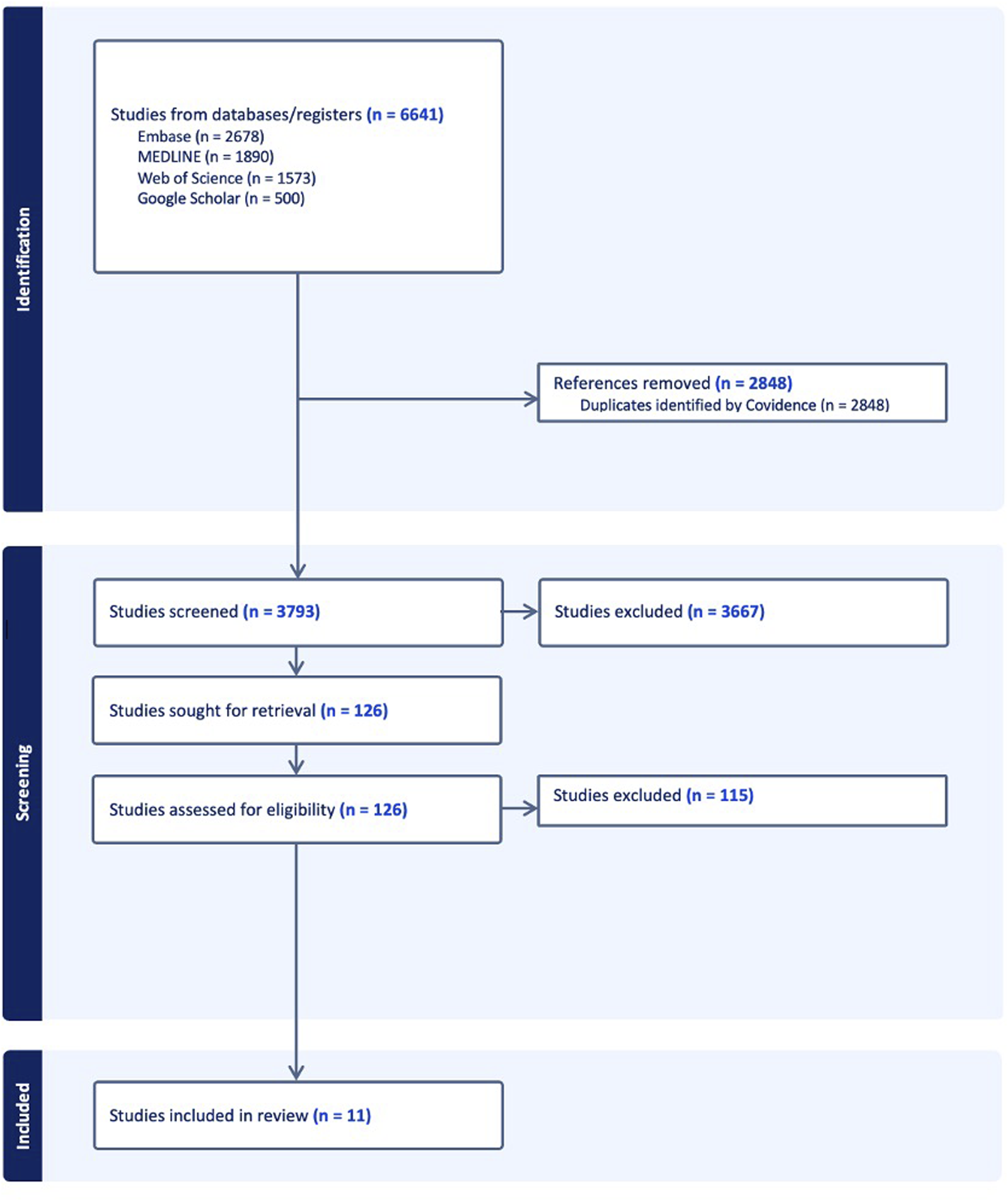
Study characteristics
Characteristics of included studies.
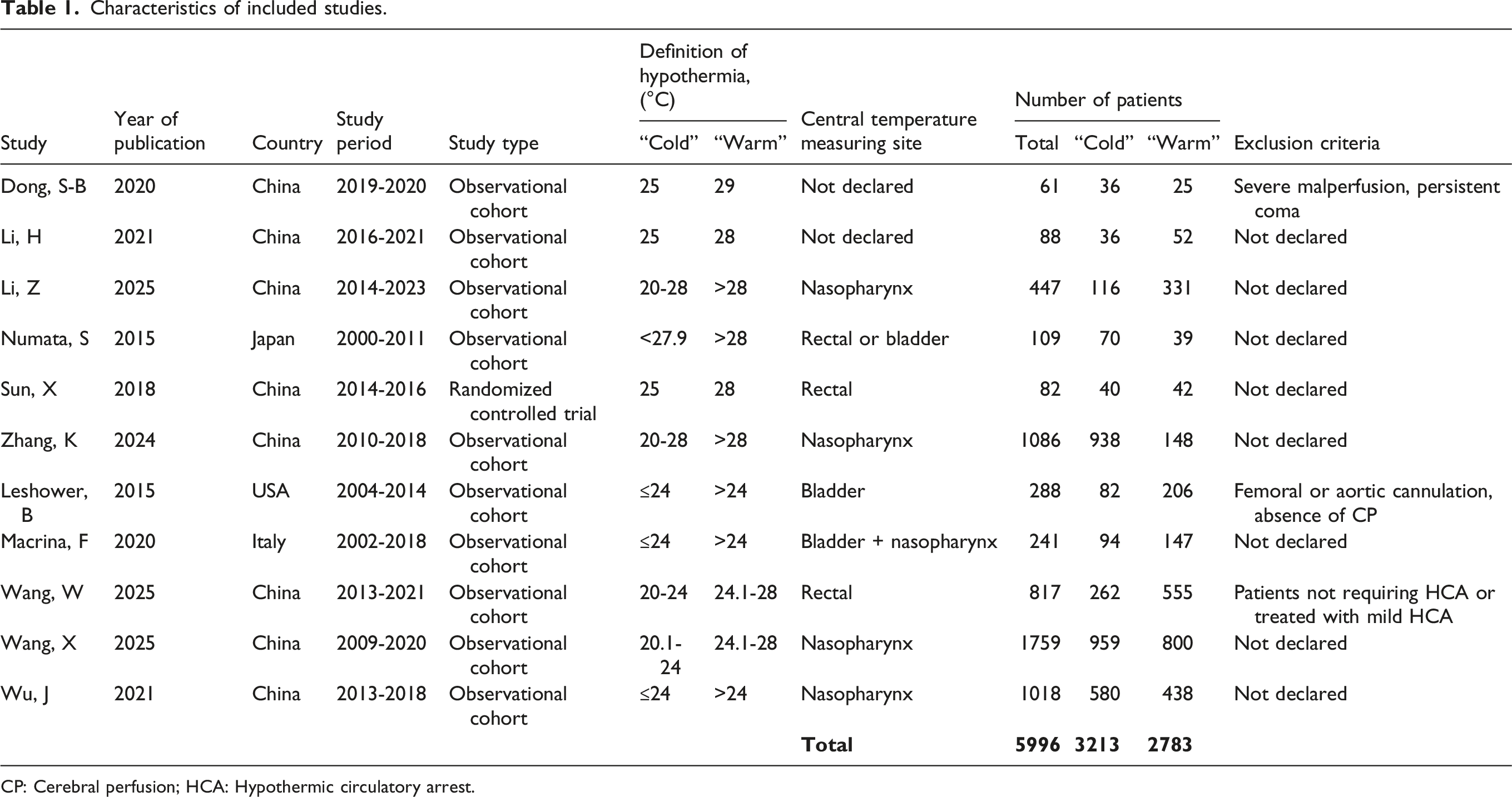
CP: Cerebral perfusion; HCA: Hypothermic circulatory arrest.
Surgical technique and perfusion data of included studies.
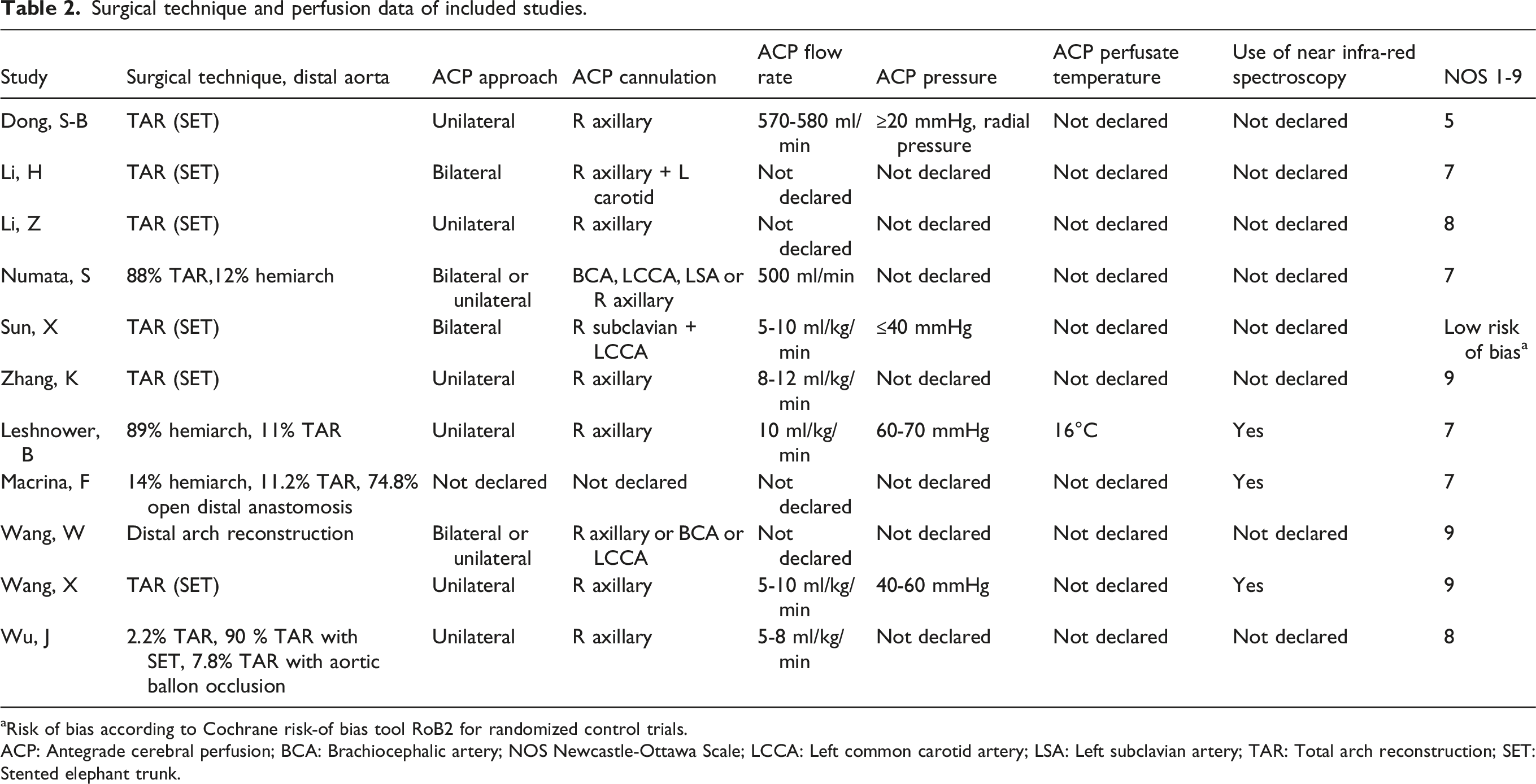
aRisk of bias according to Cochrane risk-of bias tool RoB2 for randomized control trials.
ACP: Antegrade cerebral perfusion; BCA: Brachiocephalic artery; NOS Newcastle-Ottawa Scale; LCCA: Left common carotid artery; LSA: Left subclavian artery; TAR: Total arch reconstruction; SET: Stented elephant trunk.
Surgical characteristics for each study are presented in Table 2. The most common surgical approach was total arch reconstruction (TAR) with stented elephant trunk (SET), and the right axillary artery was the most frequently used site for cerebral perfusion cannulation. The number of patients in the cold group was slightly higher than in the warm group (54% vs 46%). Seven studies reported ACP flow rates, and four studies reported pressure limits for ACP. Only one study reported the temperature of the cerebral perfusate.
Summary of patient and procedural data of included patients.
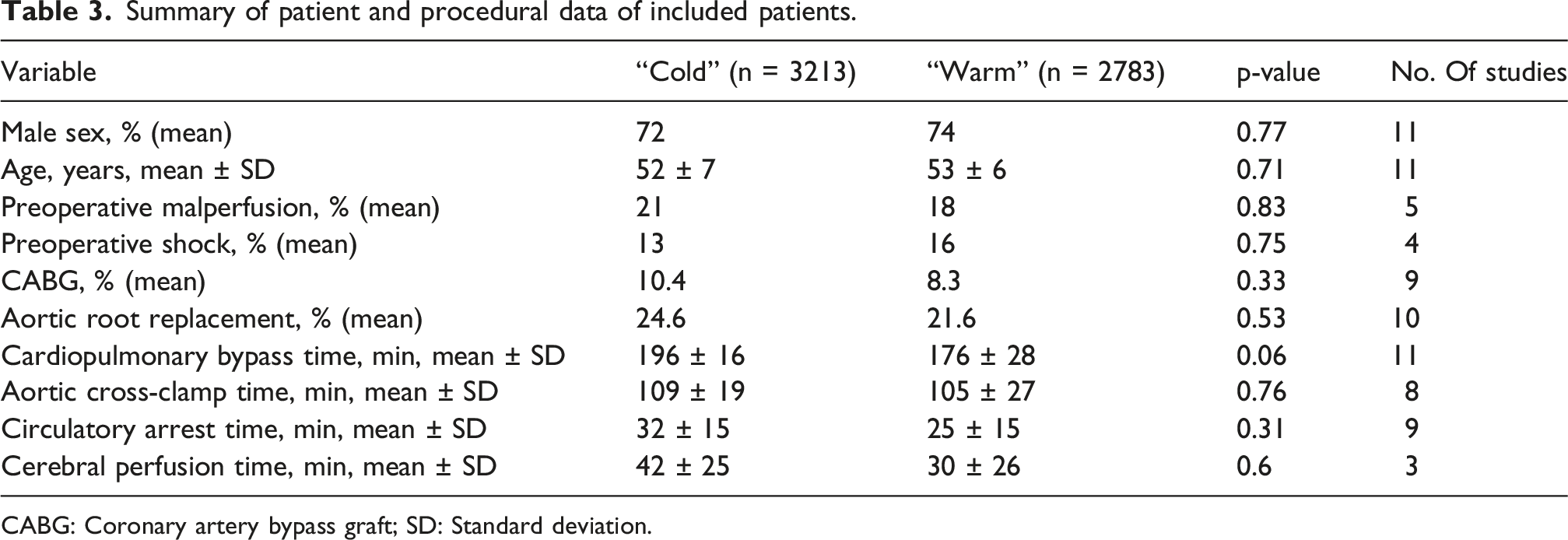
CABG: Coronary artery bypass graft; SD: Standard deviation.
Results of quality assessment/bias assessment
The mean NOS-score for the 10 observational cohort studies was 7.6, and the risk of bias for the one RCT-study 12 according to the RoB2 was judged low (Table 2).
Result of the meta-analysis
According to compared levels of hypothermia, forest plots were made comparing random effect models between low-moderate hypothermia versus high-moderate hypothermia and moderate hypothermia versus mild hypothermia, also including an overall effect comparing the lower grade of hypothermia with the higher one.
Figures 2–4 present the investigated outcomes across all included studies in forest plots. The random-effects meta-analysis yielded a pooled OR for in-hospital mortality of 0.72 (95% CI 0.59–0.88). Heterogeneity was minimal (K = 11; Q (10) = 7.4, p = 0.69; τ2 = 0; I2 = 0), as shown in Figure 2. Forest plot describing in-hospital mortality after ATAAD surgery. Forest plot describing postoperative stroke after ATAAD surgery. Forest plot describing postoperative dialysis after ATAAD surgery.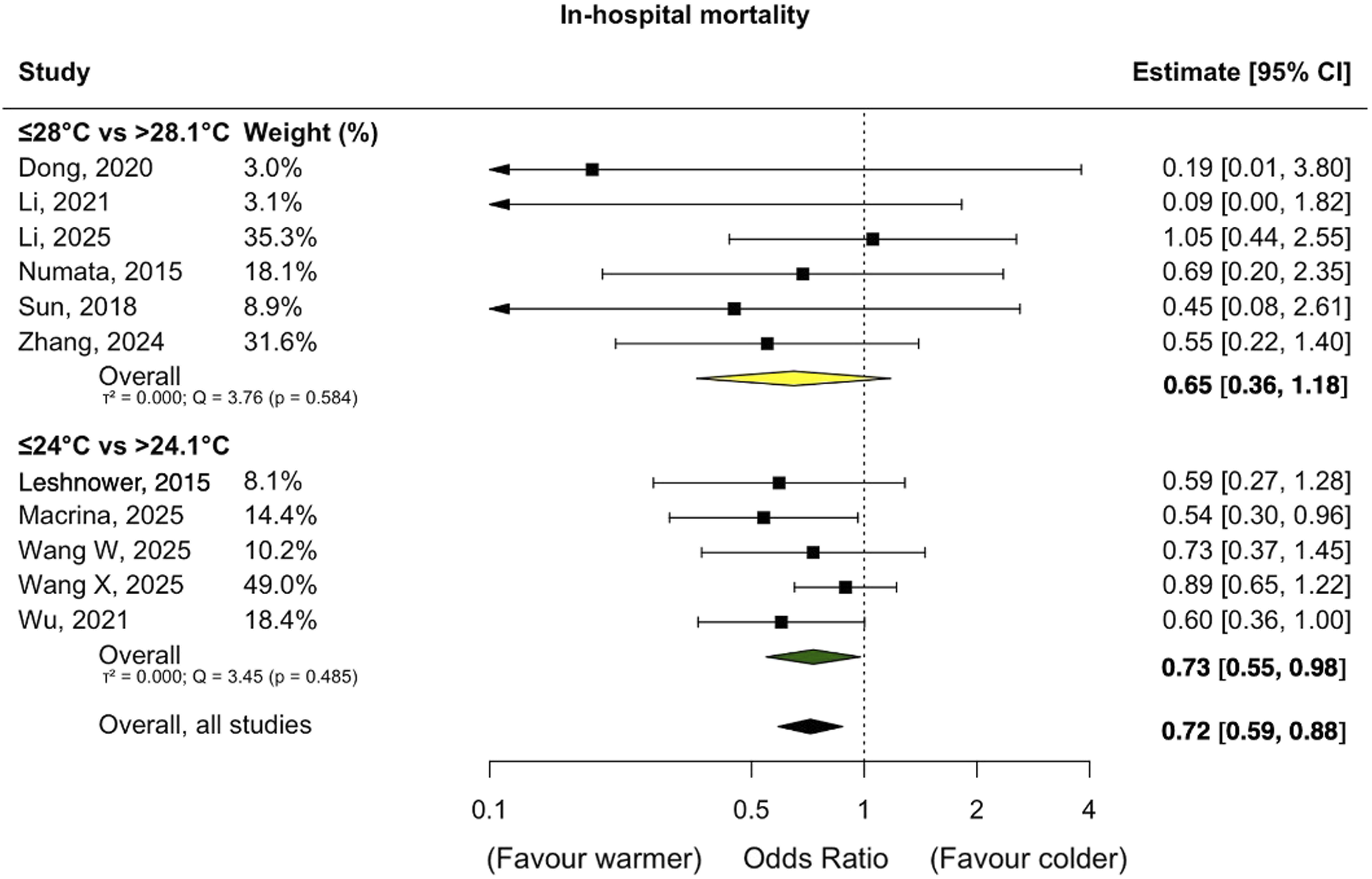
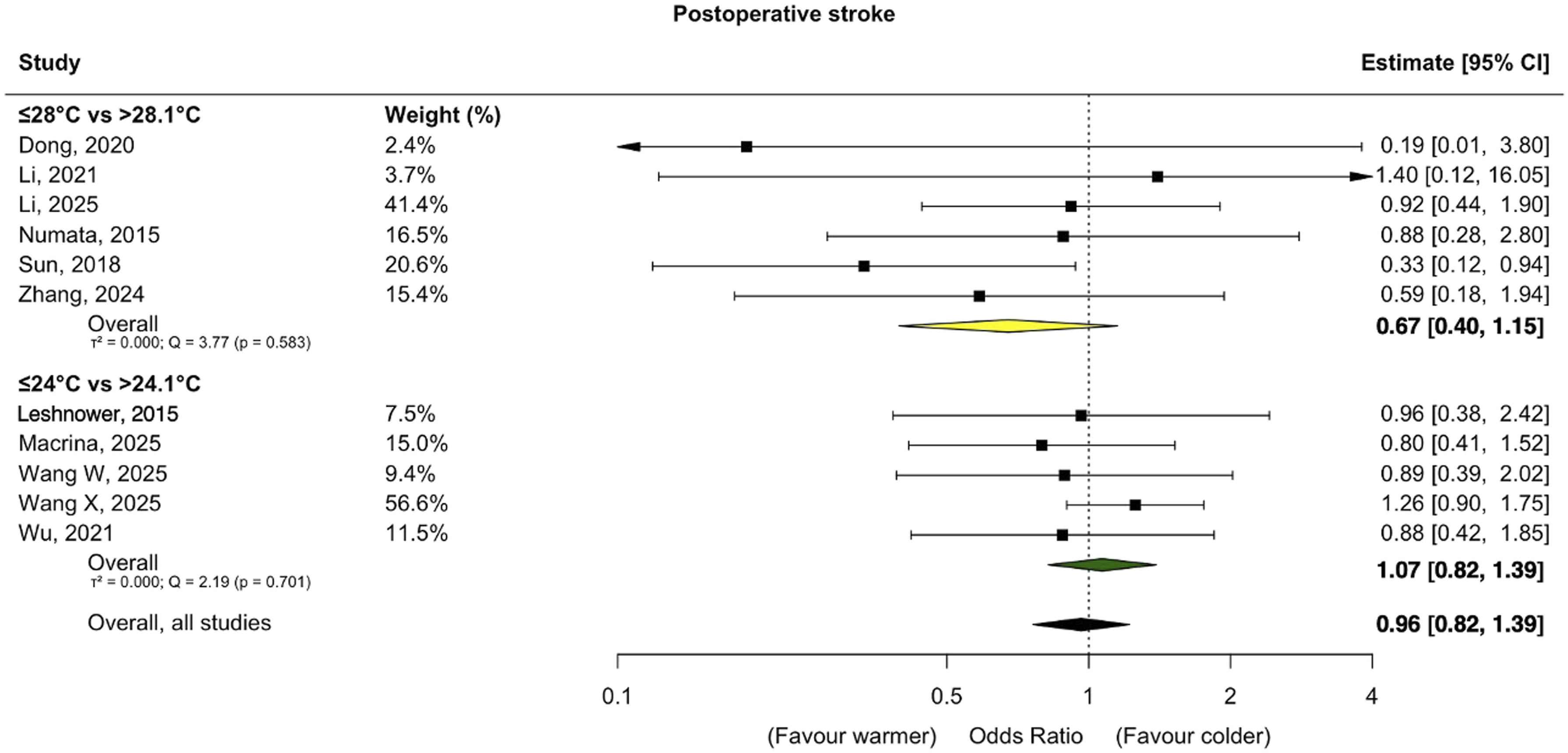
The pooled OR for postoperative stroke was 0.96 (95% CI 0.76-1.22), presented in Figure 3. Heterogeneity for postoperative stroke was also negligible (K = 11; Q (10) = 8.8, p = 0.55; τ2 = 0; I2 = 0).
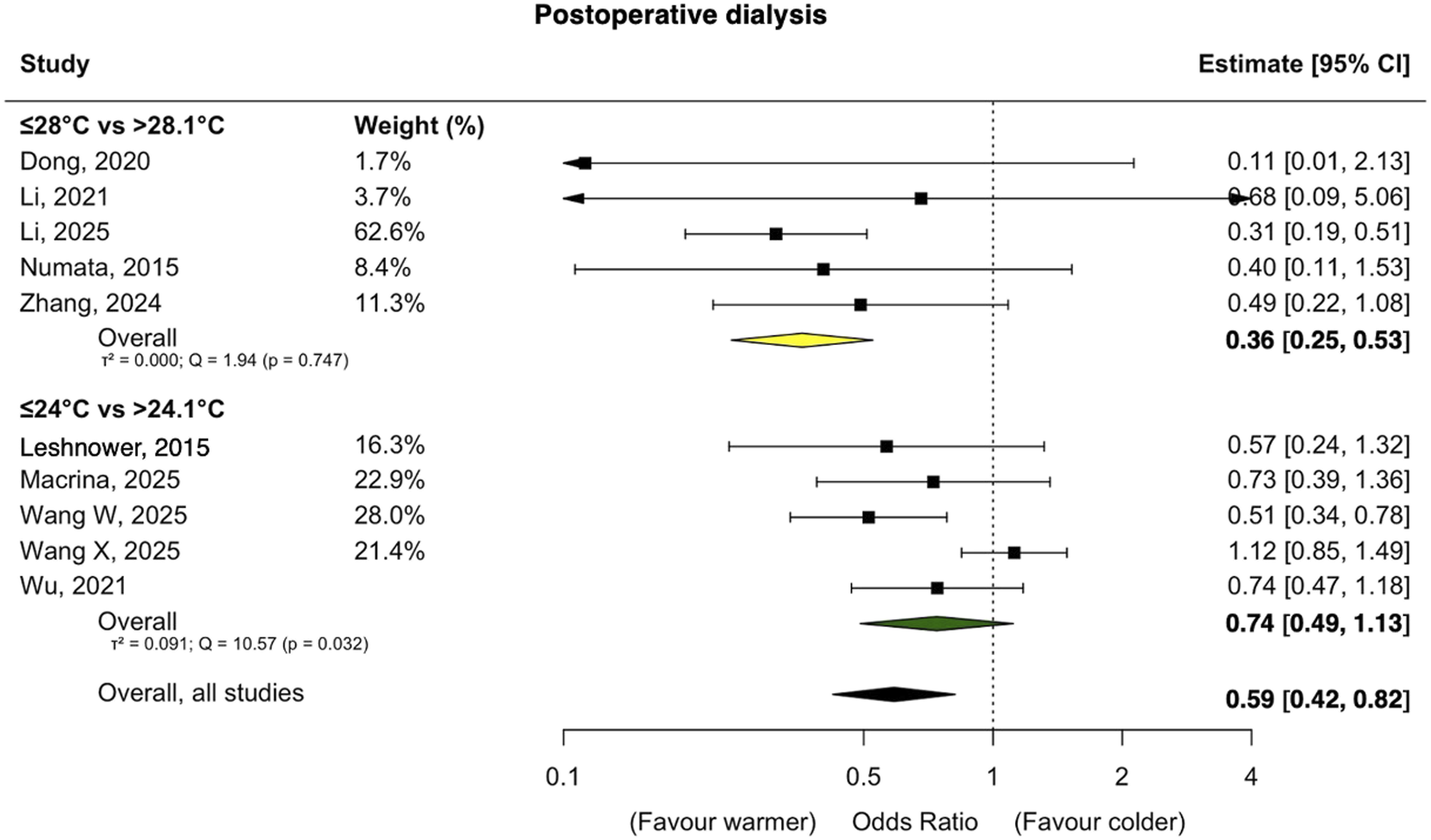
For postoperative dialysis, the OR was 0.59 (95% CI 0.42-0.82), as illustrated in Figure 4. The heterogeneity for this outcome was substantial (K = 10; Q (9) = 26.55, p = 0.0017; τ2 = 0.173; I2 = 66.1%).
Publication bias
Funnel plots for all studied outcomes are presented in Figure 5. Egger’s regression p-values for each studied outcome were 0.02 for in-hospital mortality, 0.02 for postoperative stroke and 0.13 for postoperative dialysis. Funnel plots for all studied outcomes.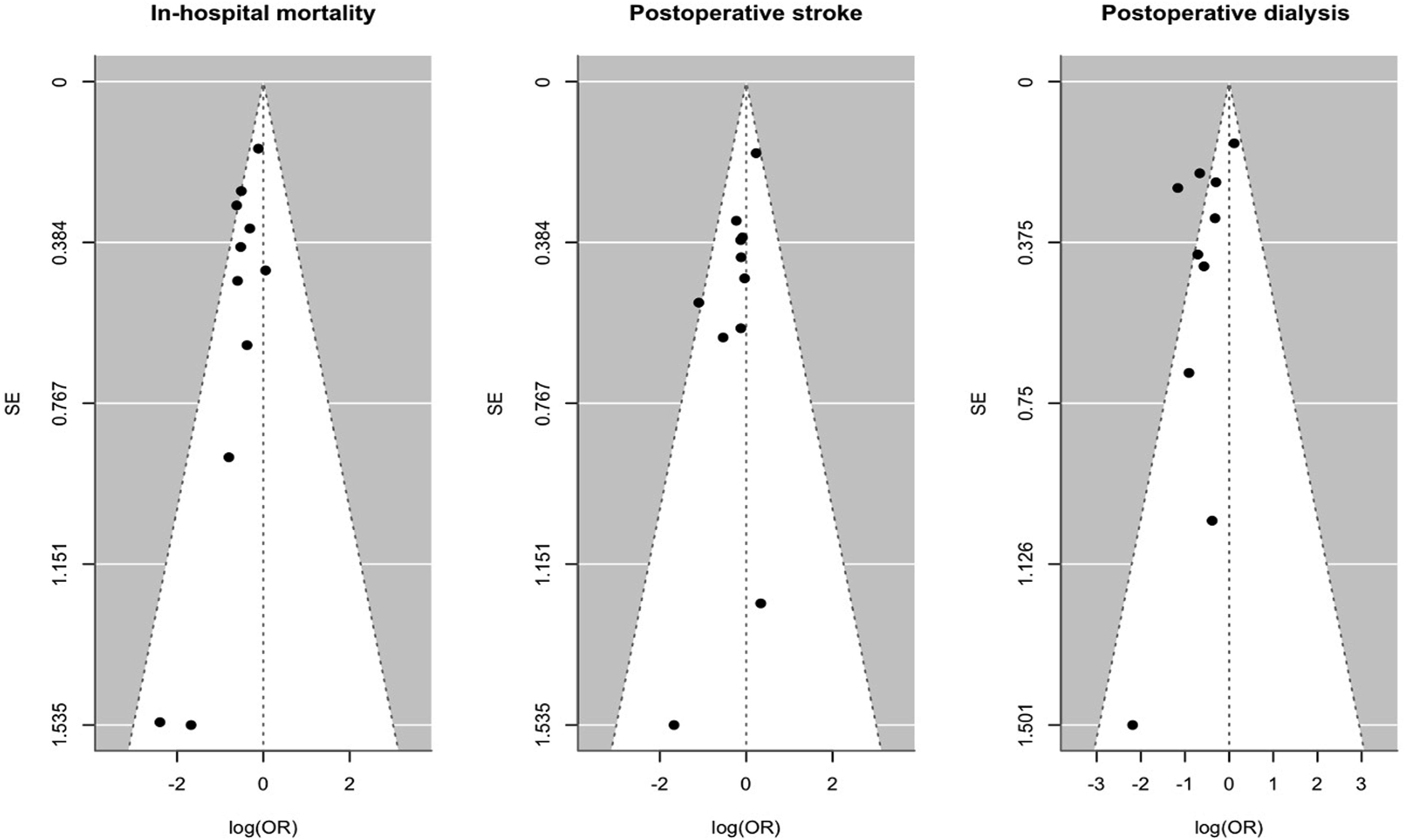
Discussion
In this meta-analysis, colder hypothermia was never superior to warmer hypothermia in ATAAD surgery, regarding the outcomes in-hospital mortality, postoperative stroke, and postoperative kidney failure requiring dialysis.
The use of hypothermia in cardiac surgery has evolved substantially during the last 25 years. It remains important to establish a safe upper threshold for hypothermia, to maintain the protective features of hypothermia and at the same time minimizing potential downsides of cooling patients. McCullough and colleagues 22 proposed in 1999 that a safe temperature to begin HCA was 20°C, to achieve the maximal metabolic suppression of the brain. In contrast, today, there are reports of cooling patients to a core temperature of 30°C, but now with the augmentation of ACP during the circulatory arrest period. 23 Although the optimal level of hypothermia has been investigated in several previous studies, this systematic review and meta-analysis aimed to further evaluate the use of warmer degrees of hypothermia in combination with ACP, as surgical techniques and approaches for the treatment of ATAAD continue to vary considerably between centres.
In addition, many studies in this field report only a single technique or a specific level of hypothermia without including a control group or comparative analysis, which makes the conduct of meta-analyses such as this more challenging.
Other things equal, the use of mild hypothermia would shorten cardiopulmonary bypass time, as rewarming time will be reduced, compared with strategies with deeper levels of hypothermia. A recent study by Uimonen et al. 24 demonstrated that increased cardiopulmonary bypass time in patients undergoing surgery for ATAAD worsened outcomes, which are in line with the findings of this meta-analysis. Increased cardiopulmonary bypass time in previous studies has also been associated with worsened rates of acute kidney injury, 25 postoperative neurocognitive dysfunction 26 and thrombocyte dysfunction. 27
Important perfusion-related parameters, including perfusate temperature as well as ACP flow and pressure targets, were not consistently reported across the included studies. These variables should be more clearly and systematically documented to enable future meta-analyses to better account for their potential impact, thereby contributing to the establishment of safe and standardized strategies for hypothermic circulatory arrest and cerebral perfusion in ATAAD surgery.
Assessment of potential publication bias
For in-hospital mortality and postoperative stroke, Egger’s regression test demonstrated a statistically significant asymmetry (p = 0.02), indicating a likely small-study effect or publication bias. This interpretation was also supported by the visual inspection of the funnel plot, which showed a marked asymmetry with an overrepresentation of smaller studies reporting relatively large protective effects of the exposure. Consequently, the pooled effects of these outcomes should be interpreted with caution, as the true underlying effect size may be overestimated.
For postoperative dialysis, neither the Egger’s regression test (p = 0.13) nor the funnel plot indicated asymmetry. This suggests that publication bias is unlikely to have influenced the evidence base for this outcome, and the pooled estimates here can be considered more reliable.
Taken together, these findings indicate that publication bias may have selectively affected the primary outcome, in-hospital mortality and postoperative stroke but not postoperative dialysis. In the context of the present meta-analysis, this means that while the protective association suggested for in-hospital mortality may reflect a genuine biological or clinical effect, the magnitude of this effect should be interpreted with caution.
Issues regarding heterogeneity among studies
Across the included studies, ”warmer” patients had a significant reduction in in-hospital mortality. The pooled random-effects estimate demonstrated a consistent benefit with minimal statistical heterogeneity (I2 = 0%). This suggests that the mortality effect was both directionally and quantitatively stable across studies, strengthening the robustness of this outcome. Nevertheless, even in the setting of negligible statistical heterogeneity, clinical variation between studies cannot be fully excluded. For postoperative stroke heterogeneity remained negligible (I2 ≈ 2%), and the pooled effect indicated no substantial inconsistency across the available studies. The low level of between-study variability supports the reliability of this estimate. In contrast, the analysis of postoperative dialysis demonstrated substantial heterogeneity (I2 = 66%), indicating that effect sizes varied meaningfully across studies. Although the pooled OR in this case also favoured the ”warmer” patients and reached statistical significance, the heterogeneity suggests that the magnitude of effect differs across populations and study settings. Consequently, while the direction of benefit appears consistent, the effect estimate for postoperative dialysis should be interpreted with caution.
Limitations
A limited number (n = 11) of published reports were included in this meta-analysis, and they were mostly observational studies (except one RCT). The heterogeneity of preoperative demographic characteristics, operative durations, definitions of hypothermia and postoperative outcomes might lead to inaccuracy of the results. The heterogeneous nature of variations in operative strategies made it difficult to compare clinical outcomes precisely at different HCA temperatures. There were also a broad variation and incompleteness in the reporting of detailed perfusion data. ORs from included studies were obtained from raw data, making them unadjusted, which could be a confounding factor. It should also be addressed that the different studies referred to neurological outcomes in different terms, such as temporary neurological dysfunction, permanent neurological dysfunction, stroke and cerebral accident. In this meta-analysis all these outcomes are labelled “postoperative stroke”, which is a broader, more inclusive term. The lack of descriptive preoperative status data such as specified malperfusion status, shock and cardiac tamponade, should also be addressed as a weakness when comparing the “cold” and “warm” group. Lastly, 8 out 11 studies were conducted in China with potential differences in genetic background, baseline risk profiles, and clinical management strategies that could have influenced the pooled estimates. Consequently, the applicability of these findings to other populations could require further validation in multicentre studies from diverse geographic regions.
Conclusions
Across all evaluated outcomes, deeper hypothermia did not demonstrate superiority over warmer strategies regarding in-hospital mortality, postoperative stroke or acute kidney failure requiring dialysis. A definitive optimal temperature threshold for ATAAD surgery requiring hypothermic circulatory arrest and ACP remains to be established.
Supplemental material
Supplemental material - Levels of hypothermia and clinical outcomes in acute type a aortic dissection surgery with circulatory arrest and antegrade cerebral perfusion: A systematic review and meta-analysis
Supplemental material for Levels of hypothermia and clinical outcomes in acute type a aortic dissection surgery with circulatory arrest and antegrade cerebral perfusion: A systematic review and meta-analysis by Erik Braatz, Magnus Dalén, Christian Olsson, Malin Stenman in Perfusion.
Footnotes
Acknowledgements
The authors would like to thank Lovisa Liljegren and Narcisa Hannerz, librarians at Karolinska Institutet, for developing the search strategy and performing the literature search.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Erik Braatz and Malin Stenman were financially supported by donations from the Swedish Heart Lung Foundation (Grant number 20251356). Magnus Dalén and Christian Olsson were financially supported by a donation from Mr Fredrik Lundberg, MD h.c.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.