
Abstract
Background
Bicuspid aortic valve (BAV) disease is a leading cause of aortic stenosis (AS). Surgical aortic valve replacement (SAVR) has traditionally been regarded as the best therapeutic option for bicuspid AS. However, the distinctive anatomical characteristics of BAV make the treatment with transcatheter aortic valve replacement (TAVR) challenging, so this population was often excluded from the trials. We aimed to compare TAVR and SAVR in terms of safety and efficacy in the population with bicuspid AS.
Methods
We conducted a systematic review and meta-analysis of randomized controlled trials (RCTs) and observational studies, searched from PubMed, Cochrane, Scopus, and Web of Science (from inception until September 2025). Dichotomous outcomes were pooled as risk ratios (RRs), and continuous outcomes as mean differences (MDs), each with 95% confidence intervals (CIs).
Results
A total of 78,677 patients were included in one RCT, 12 retrospective cohort studies, and one prospective cohort study. TAVR, compared to SAVR, was associated with significantly higher rates of permanent pacemaker implantation (PPI) (O.R. = 2.29, 95% C.I. [1.51, 3.47], P < 0.01) and shorter length of hospital stay (M.D. = −2.24, 95% C.I. [-3.96, −0.52], P = 0.01) and lower bleeding rates (O.R. = 0.31, 95% C.I. [0.14, 0.69], P < 0.01). However, there were no significant differences in all-cause mortality (ACM) (P = 0.948), acute kidney injury (AKI) (P = 0.28), stroke incidence (P = 0.475), and vascular complications (P = 0.31). The PPI and stroke rate results were consistent during in-hospital and short-term follow-ups. However, subgroup analysis by follow-up duration revealed that long-term stroke incidence was significantly higher in the TAVI group.
Conclusion
TAVR offers benefit by minimizing significant bleeding and hospital length of stay. However, the benefits should be balanced against the considerably increased risk of PPI and PVL. Further RCTs are needed to confirm these findings.
Introduction
Bicuspid aortic valve (BAV) disease is the most prevalent congenital heart disease and leading cause of aortic stenosis (AS) in young people. Up to 50% of people with BAV require aortic valve replacement during their lifespan. 1 The number of older patients with bicuspid AS is also rising. A BAV accelerates disease progression, raises the risk of AS, and also poses hurdles to treatments due to its distinctive anatomical characteristics, including aortopathy cusp fusion with a calcified raphe, and asymmetric leaflet calcification.2,3
The flow hemodynamics of the aortic valve in bicuspid cases leads to premature leaflet degradation. Compared to tricuspid aortic valves, stenotic BAVs contain more calcified leaflets and raphes, as well as dilatation of the aortic annulus and root. 3 The British Society of Echocardiography advocates routine echocardiograms for patients with BAV to assess valve hemodynamics, severity of stenosis, and left ventricular function. 4
Surgical aortic valve replacement (SAVR) has traditionally been regarded as the best therapeutic option for bicuspid AS because of its younger age of presentation compared to tricuspid AS and concomitant aortopathies, which generally require aortic root repair. 1 Concomitant aortopathy necessitates aortic root repair, posing a risk of aortic dissection and presenting technical obstacles due to bicuspid anatomy.5,6 However, the advent of transcatheter devices during the last two decades has led to debate regarding the best management strategy for patients with AS.
Early randomized controlled trials (RCTs) suggested that transcatheter aortic valve replacement (TAVR) was initially reserved for patients with significant surgical risk and contraindications to SAVR.5,7 Subsequent trials found that TAVR was not inferior to SAVR in intermediate-risk individuals.8,9 Recent RCTs found that tricuspid AS results were equivalent following TAVR and SAVR, especially in low-risk patients.10,11 The PARTNER III trial found that TAVR in low-risk patients reduced the risk of death, stroke, or rehospitalization after 1 year. 10 Patients with BAV were excluded from clinical studies due to technical concerns regarding their characteristics and potential for aortopathy.
With more experience with TAVR and a lower threshold for younger and lower-risk patients, there is potential in expanding the procedure to individuals with bicuspid AS. Although TAVR is commonly used in high- and extreme-risk AS patients, BAV patients with AS were omitted from pivotal trials that led to its approval in the US.5,7,8 We aimed to compare the safety and efficacy outcomes after SAVR and TAVR in stenosis of BAV.
Methods
Protocol registration
This systematic review and meta-analysis were conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 12 (Table S1) and adhere to the Cochrane Handbook for intervention. 13 The review protocol was registered in PROSPERO with ID: CRD420251155812 .
Data sources and search strategy
PubMed, SCOPUS, Web of Science, and Cochrane Library databases were searched from inception up to September 2025 using the search terms related to “Bicuspid Aortic Valve Disease,”, “SAVR,” and “TAVR”. The detailed search terms used for each database are written in (Table S2). Manual backward and forward citation analyses were done for all the references of the included studies.
Eligibility criteria
Eligible studies were RCTs and observational studies that had the following PICO criteria • • • •
There were no restrictions based on sex, ethnicity, setting, or publication date. We excluded the previous reviews, cross-sectional studies, single-arm studies, case reports, case series, conference abstracts, preclinical studies, animal studies, editorial studies, non-English studies, pharmacokinetics, and pharmacodynamics studies, which had no clear clinical outcomes.
Study selection
The retrieved references were screened in two steps by four reviewers working in two independent pairs (O.H.A., A.A.A., F.A.A., F.S.A.). At both the title/abstract and full-text levels, each record was screened independently by two reviewers; disagreements were resolved by discussion within the pair or, if needed, by another reviewer (A.M.). The Rayyan website was used for the selection process. 14
Data extraction
Using a standard Google spreadsheet, four authors independently (A.F.A., T.N.A., R.M.A., A.G.A.) extracted the data, and any conflicts were resolved by discussion within the pair or, if needed, by another reviewer (A.M). Extracted data were divided into three domains: (1) (2) (3)
Quality assessment
Two reviewers independently (O.H.A., A.A.A.) assessed the risk of bias in included RCTs using the Cochrane Risk of Bias (ROB-2) assessment tool. 15 This evaluation encompassed an assessment of the randomization process, concealment of the allocation sequence, deviations from the intended interventions, utilization of appropriate analysis to estimate the effect of assignment to intervention, measurement of the outcome, selection of the reported results, and overall risk of bias. Observational studies were appraised using the Newcastle–Ottawa Scale (NOS), which evaluates study quality across three categories: adequacy of the sample, comparability between intervention and control groups, and outcome assessment. 16 Any discrepancies were resolved through consultation with a third investigator.
Statistical analysis
We used R version 4.3 and the meta packages for statistical analysis. 17 We pooled results from the studies included in our analysis using mean differences (MDs) with 95% confidence intervals (CIs) for continuous data, and odds ratios (ORs) for dichotomous data. When the reported data were not normally distributed, we converted data presented with median and interquartile range (IQR) to mean and standard deviation (SD). 18 A random-effects model using the restricted maximum likelihood (REML) estimator was applied to account for potential between-study heterogeneity. We used the chi-square test and quantified heterogeneity using the I-squared (I2) test, which quantifies the percentage of heterogeneity not attributed to chance. Heterogeneity was considered statistically significant if the chi-square test p-value was less than 0.1. Heterogeneity was interpreted according to the Cochrane Handbook, with an I2 value of 0–40% indicating low heterogeneity, 30–60% indicating moderate heterogeneity, 50–90% representing substantial heterogeneity, and 75–100% signifying considerable heterogeneity. Additionally, we conducted a subgroup analysis based on the follow-up duration as follow: in-hospital follow-up, short term follow-up (post-discharge to less than 1 year), and long-term follow-up (1 year or longer). Finally, we conducted a sensitivity analysis using the leave-one-out method to test the stability of the effect size and its direction by removing one study at a time whenever possible, and utilized L’Abbé plots to show the effect of each study on the heterogeneity and the overall effect sizes. 19 Publication bias couldn’t be assessed because of the limited number of included trials. 20
Results
Our initial search yielded 6923 potentially relevant articles, as shown in the PRISMA diagram (Figure 1). A total of 1912 duplicate studies were deleted, and 35 studies were retained for full-text evaluation. After exclusion of irrelevant studies based on our pre-determined eligibility criteria, 14 eligible articles3–16 met all inclusion criteria. PRISMA flow chart for the systematic search and selection process.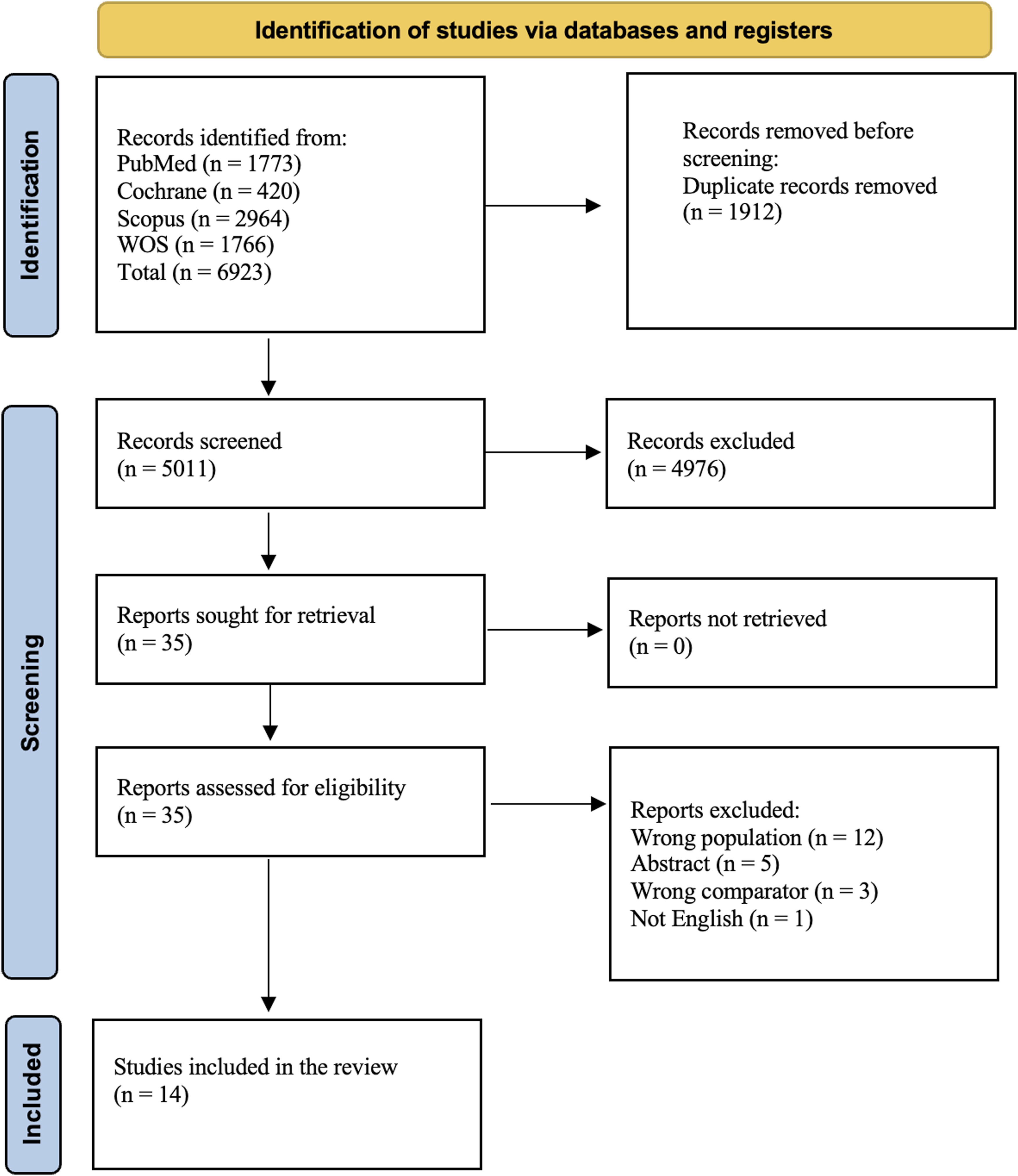
Study characteristics
Summary characteristics of the included trials.
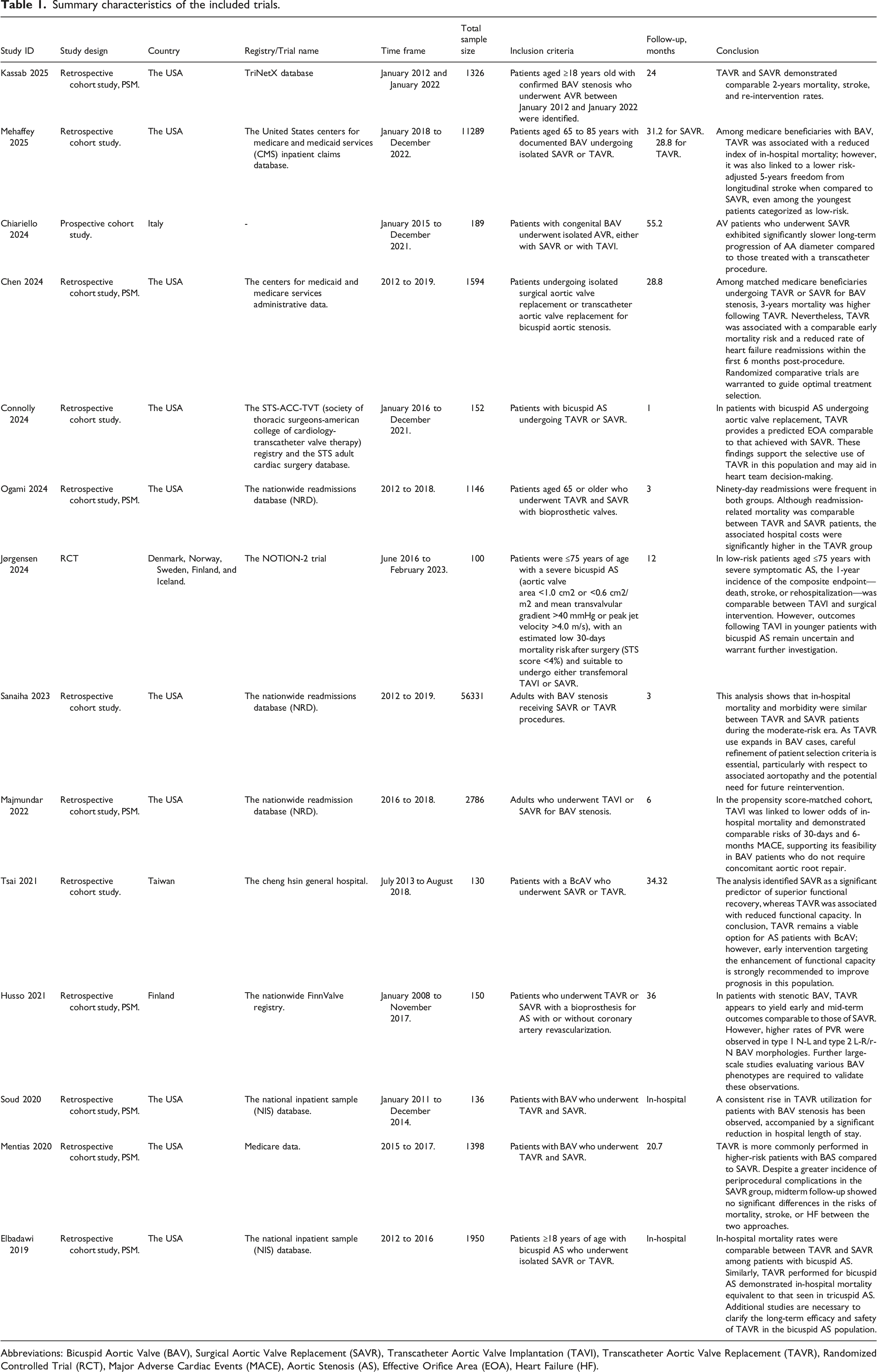
Abbreviations: Bicuspid Aortic Valve (BAV), Surgical Aortic Valve Replacement (SAVR), Transcatheter Aortic Valve Implantation (TAVI), Transcatheter Aortic Valve Replacement (TAVR), Randomized Controlled Trial (RCT), Major Adverse Cardiac Events (MACE), Aortic Stenosis (AS), Effective Orifice Area (EOA), Heart Failure (HF).
Baseline characteristics of the included patients.
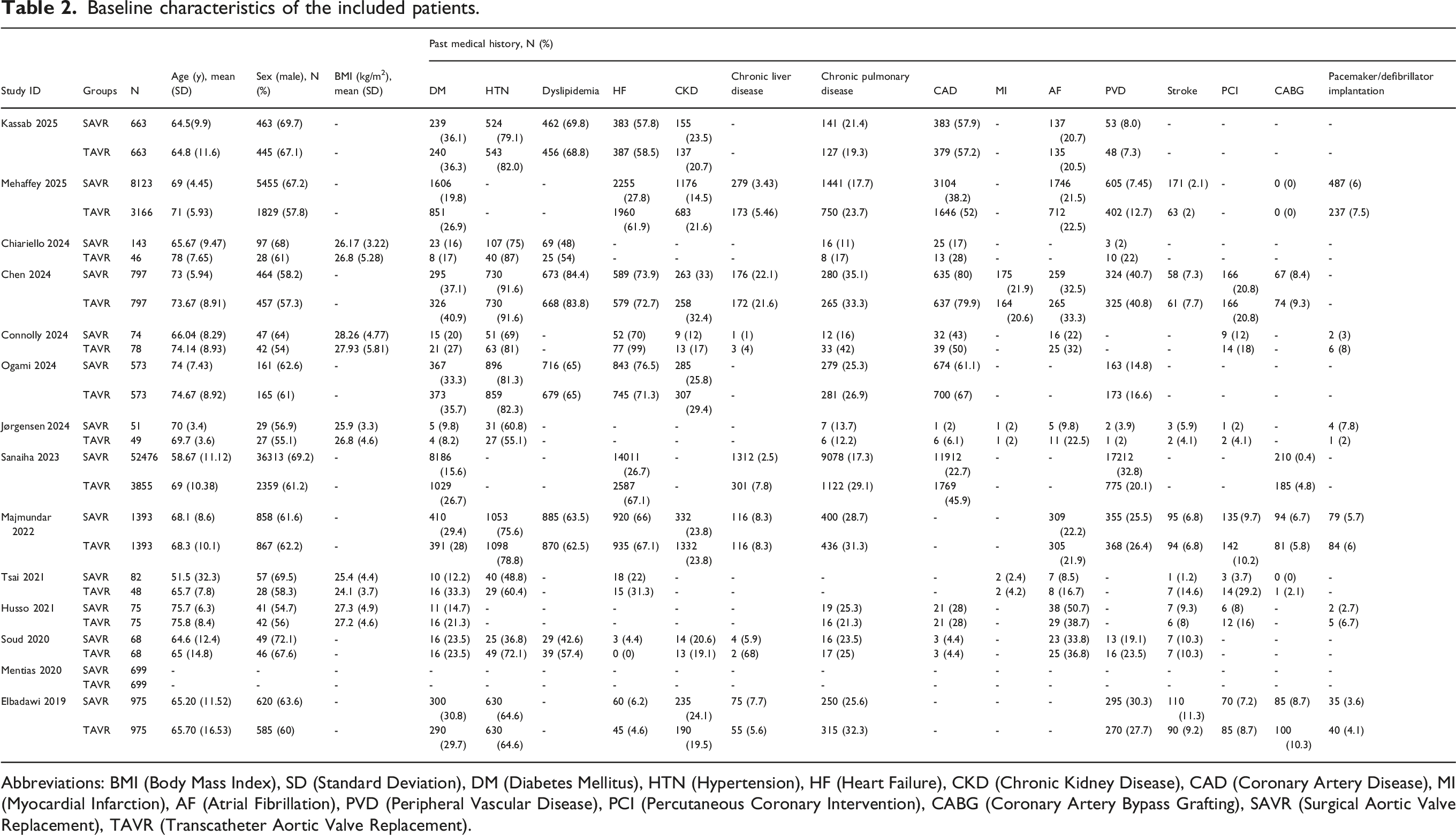
Abbreviations: BMI (Body Mass Index), SD (Standard Deviation), DM (Diabetes Mellitus), HTN (Hypertension), HF (Heart Failure), CKD (Chronic Kidney Disease), CAD (Coronary Artery Disease), MI (Myocardial Infarction), AF (Atrial Fibrillation), PVD (Peripheral Vascular Disease), PCI (Percutaneous Coronary Intervention), CABG (Coronary Artery Bypass Grafting), SAVR (Surgical Aortic Valve Replacement), TAVR (Transcatheter Aortic Valve Replacement).
Risk of bias assessment
According to the NOS tool, 12 included studies were considered to have good quality,3,4,6–8,10–16 while one study (Sanaiha 2023) was rated as fair quality due to limited comparability between groups, as potential confounders were not adequately controlled 9 (Table S3). Additionally, when the Rob2 tool was used to assess the risk of bias, Jørgensen et al. showed that it has a low risk of bias 5 (Figure S1).
Primary outcomes
PPI
The pooled analysis of 8,247 patients demonstrated a significantly higher rate of PPI in the TAVR group compared to the SAVR group (O.R. = 2.29, 95% C.I. [1.51, 3.47], P < 0.01), with the pooled studies showing substantial heterogeneity (I2 = 68.6%) (Figure 2). Nevertheless, the results remained consistent across sensitivity analyses using the leave-one-out method, as the exclusion of individual studies did not alter the direction, significance, magnitude of effect, or width of the CIs (Figure S2). Forest Plot of the PPI rates. O.R. Odds ratio, CI Confidence Interval, TAVR Transcatheter Aortic Valve Replacement, SAVR Surgical Aortic Valve Replacement, PPI permeant pacemaker implantation.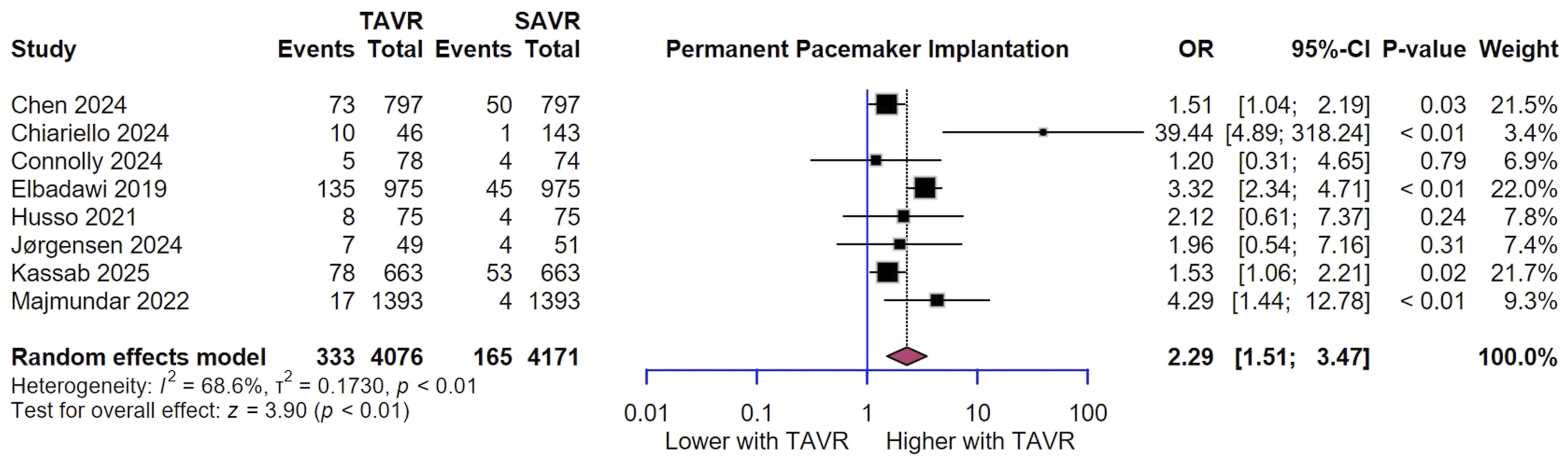
In the L'Abbé plot, the studies displayed consistent positioning above the line of no effect, with all studies contained within the 95% prediction interval (PI) and 95% CI, suggesting acceptable concordance among studies despite the heterogeneity except for Majmundar et al. 10 (Figure S3).
Upon stratification by follow-up timeframe, PPI was significantly higher with TAVR in hospital (OR 2.91, 95% CI [1.72, 4.92], p < 0.001) and at short term (OR 1.76, 95% CI [1.20, 2.58], p = 0.004). However, long-term follow-up showed similar PPI rate between the two groups (O.R. = 6.75, 95% C.I. [0.28, 155.47], P < 0.24) (Figure 3). Forest Plot of PPI rates subgroup analysis based on follow up duration. O.R. Odds ratio, CI Confidence Interval, TAVR Transcatheter Aortic Valve Replacement, SAVR Surgical Aortic Valve Replacement, PPI permeant pacemaker implantation.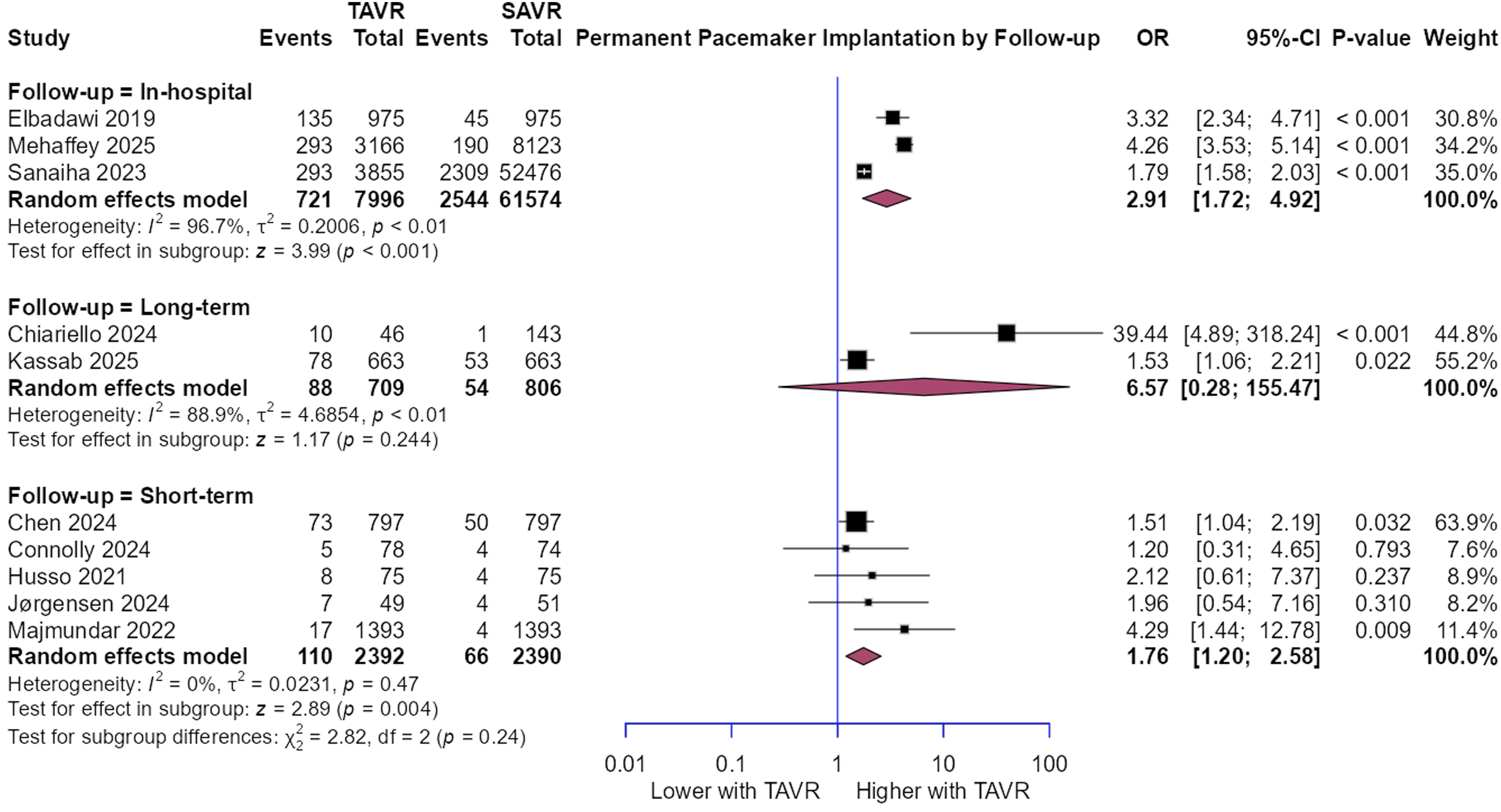
ACM
The pooled analysis of 17,920 patients showed no significant difference in ACM rates between the TAVR and SAVR groups (O.R. = 1.23, 95% C.I. [0.84, 1.80], P = 0.29). The pooled studies demonstrated substantial heterogeneity (I2 = 58.4%) (Figure 4). However, the results remained consistent across sensitivity analyses using the leave-one-out method (Figure S4). Moreover, in the L'Abbé plot, the studies showed variable distribution around the line of no effect, with most studies falling within the 95% PI and 95% CI, except for four studies7,10–12 (Figure S5). Forest Plot of the ACM. O.R. Odds ratio, CI Confidence Interval, TAVR Transcatheter Aortic Valve Replacement, SAVR Surgical Aortic Valve Replacement, ACM All Cause-Mortality.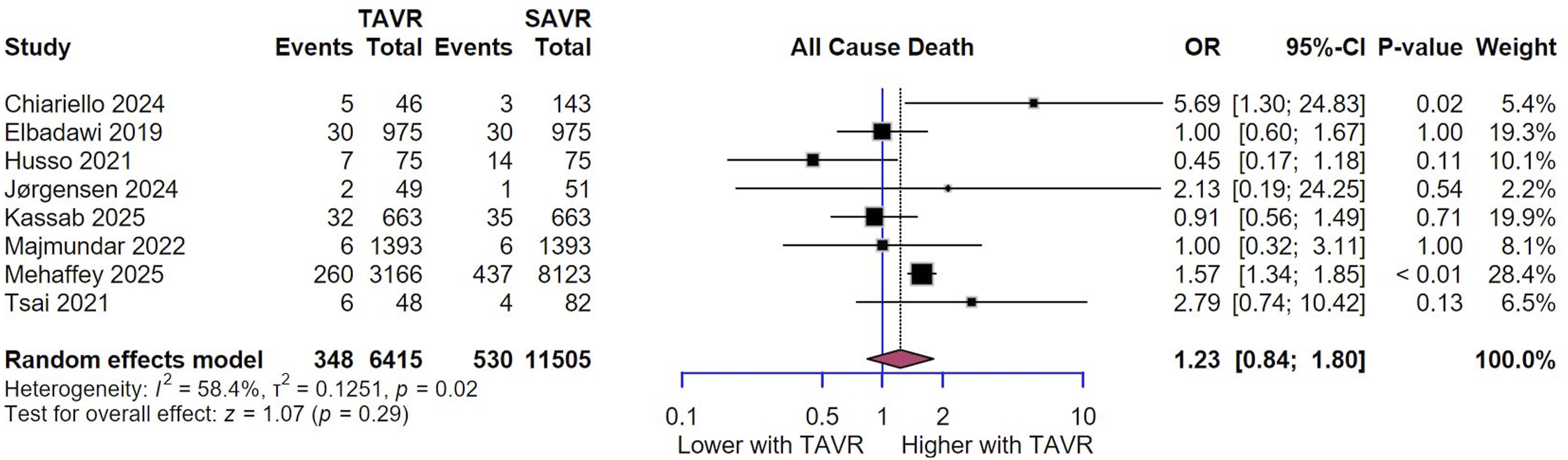
When stratifying studies by follow-up duration, there was no significant difference in all-cause death across all subgroups, in-hospital (O.R. = 0.97, 95% C.I. [0.42, 2.23], P = 0.948), long-term (O.R. = 1.38, 95% C.I. [0.69, 2.79], P = 0.364), and short-term follow-up (O.R. = 1.35, 95% C.I. [0.95, 1.93], P = 0.097) (Figure 5). Forest Plot of ACM subgroup analysis based on follow up duration. O.R. Odds ratio, CI Confidence Interval, TAVR Transcatheter Aortic Valve Replacement, SAVR Surgical Aortic Valve Replacement, ACM All-Cause Mortality.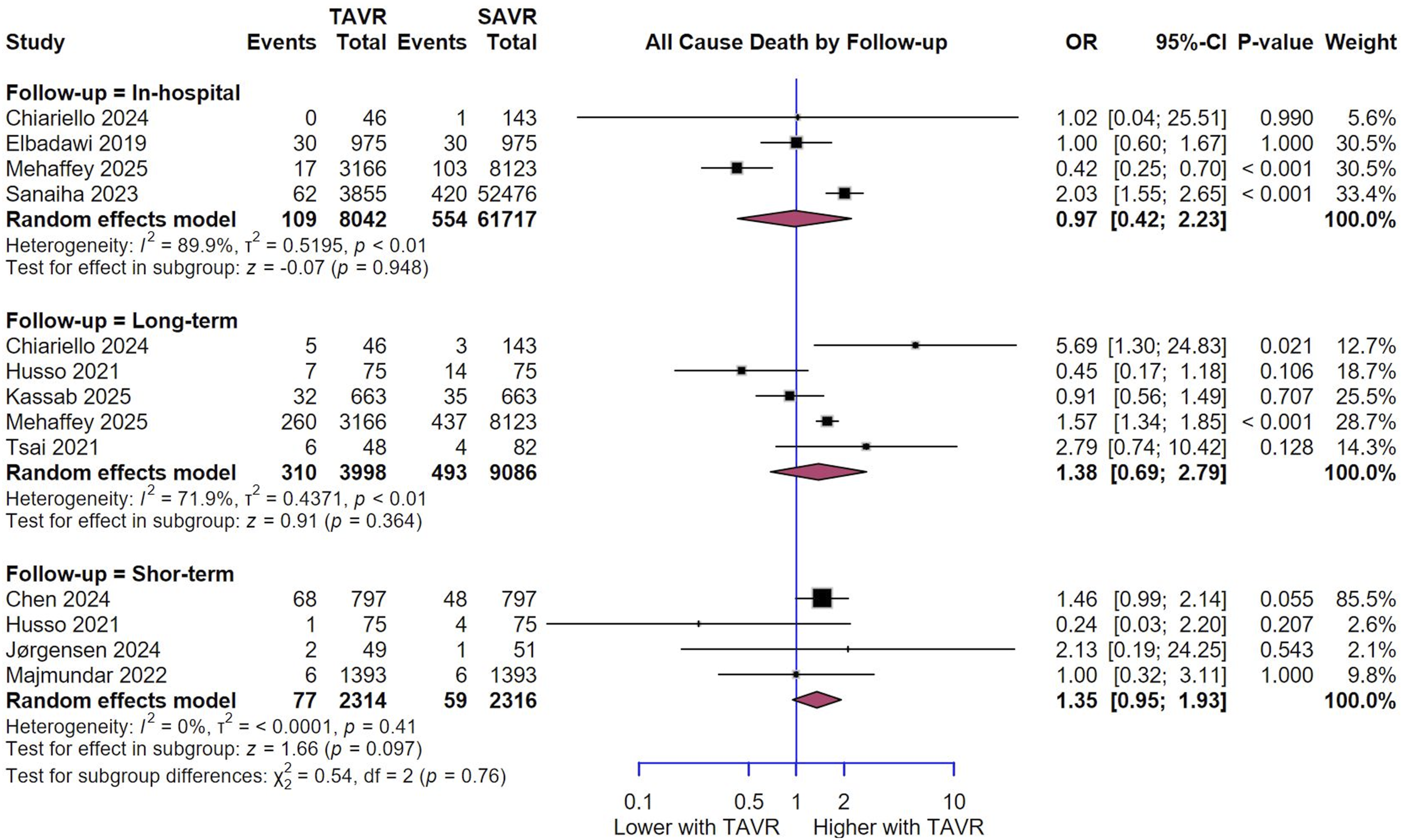
Stroke
The pooled analysis of 8,036 patients revealed no statistically significant difference in stroke rates between the TAVR group versus the SAVR group (O.R. = 1.32, 95% C.I. [0.81, 2.13], P = 0.475), with moderate heterogeneity (I2 = 47.9%) (Figure 6). Nevertheless, the findings demonstrated robustness when subjected to sensitivity analyses employing the leave-one-out approach (Figure S6). In the L'Abbé plot, the studies displayed heterogeneous positioning relative to the line of no effect, with most studies contained within the 95% PI and 95% CI, except for four studies5,10–12 (Figure S7). Forest Plot of Stroke. O.R. Odds ratio, CI Confidence Interval, TAVR Transcatheter Aortic Valve Replacement, SAVR Surgical Aortic Valve Replacement.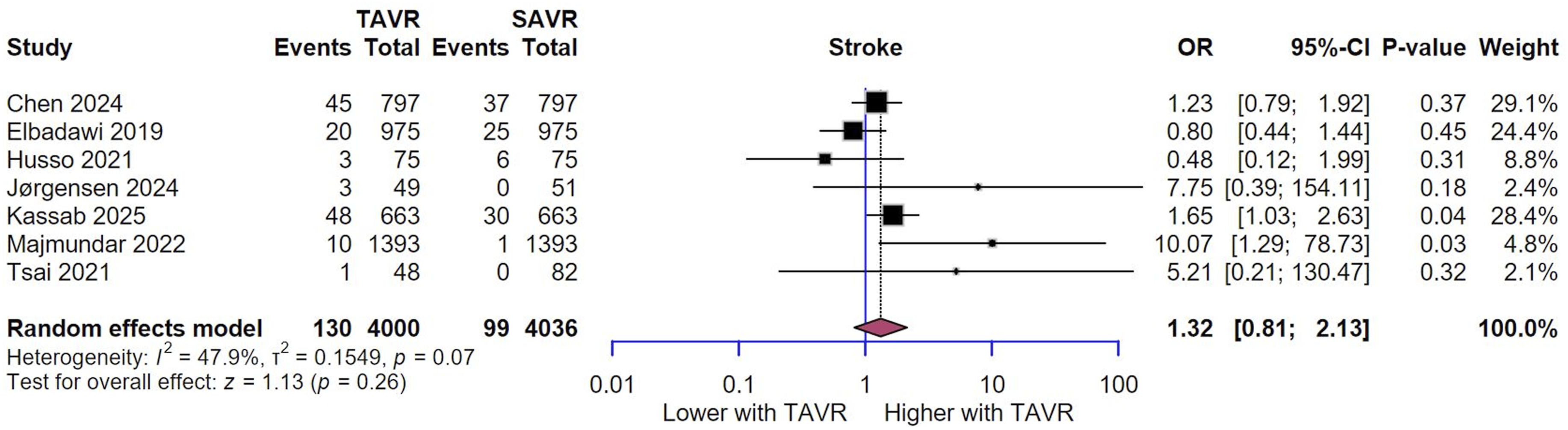
Upon stratification of studies by follow-up timeframe, no significant differences in stroke occurrence were observed across in-hospital (O.R. = 0.99, 95% C.I. [0.79, 1.24], P = 0.931), and short-term follow-up (O.R. = 1.79, 95% C.I. [0.46, 6.99], P = 0.403). However, subgroup analysis by follow-up duration revealed that long-term stroke incidence was significantly higher in the TAVI group (O.R. = 1.43, 95% C.I. [1.04, 1.97], P = 0.029) (Figure 7). Forest Plot of Stroke rates subgroup analysis based on follow up duration. O.R. Odds ratio, CI Confidence Interval, TAVR Transcatheter Aortic Valve Replacement, SAVR Surgical Aortic Valve Replacement.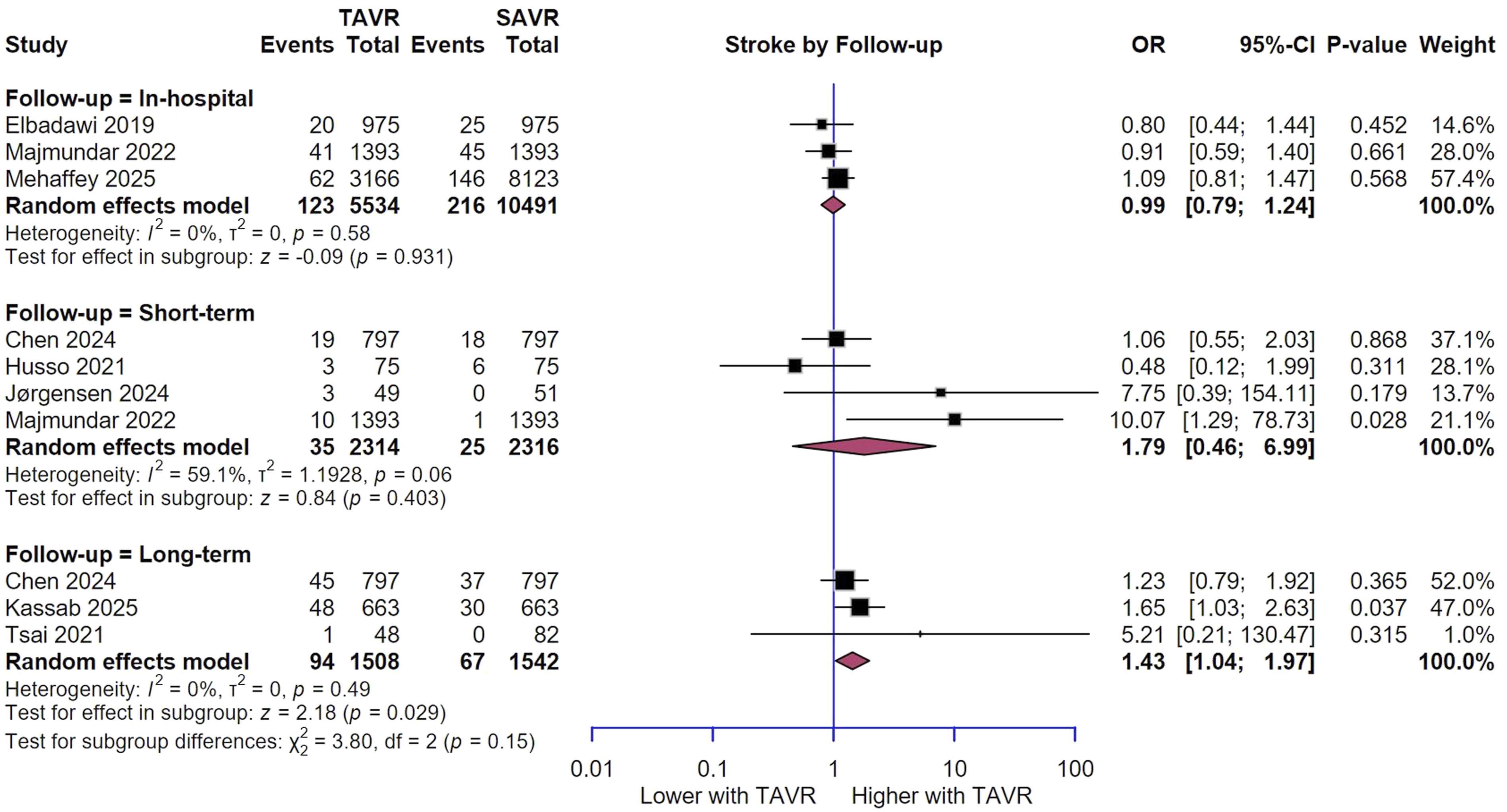
Secondary outcomes
PVL were significantly higher in the TAVR group compared to the SAVR group (O.R. = 4.60, 95% C.I. [1.43, 14.78], P = 0.01) (Figure 8). Hospital length of stay was significantly shorter in the TAVR group compared to the SAVR group (M.D. = −2.24, 95% C.I. [-3.96, −0.52], P = 0.01) (Figure S8). MI rates were comparable between the TAVR and SAVR groups (O.R. = 0.85, 95% C.I. [0.45, 1.60], P = 0.62) (Figure S9). Similarly, AKI rates showed no significant difference between the two groups (O.R. = 0.66, 95% C.I. [0.31, 1.39], P = 0.28) (Figure S10). However, bleeding rates were significantly lower in the TAVR group compared to the SAVR group (O.R. = 0.31, 95% C.I. [0.14, 0.69], P < 0.01) (Figure S11). Conversely, the two groups had similar vascular complications (O.R. = 1.77, 95% C.I. [0.59, 5.30], P = 0.31) (Figures S12). Nevertheless, valve reintervention rates showed no significant difference between the two groups (O.R. = 2.59, 95% C.I. [0.63, 10.65], P = 0.19) (Figure S13). Forest Plot of PVL. O.R. Odds ratio, CI Confidence Interval, TAVR Transcatheter Aortic Valve Replacement, SAVR Surgical Aortic Valve Replacement.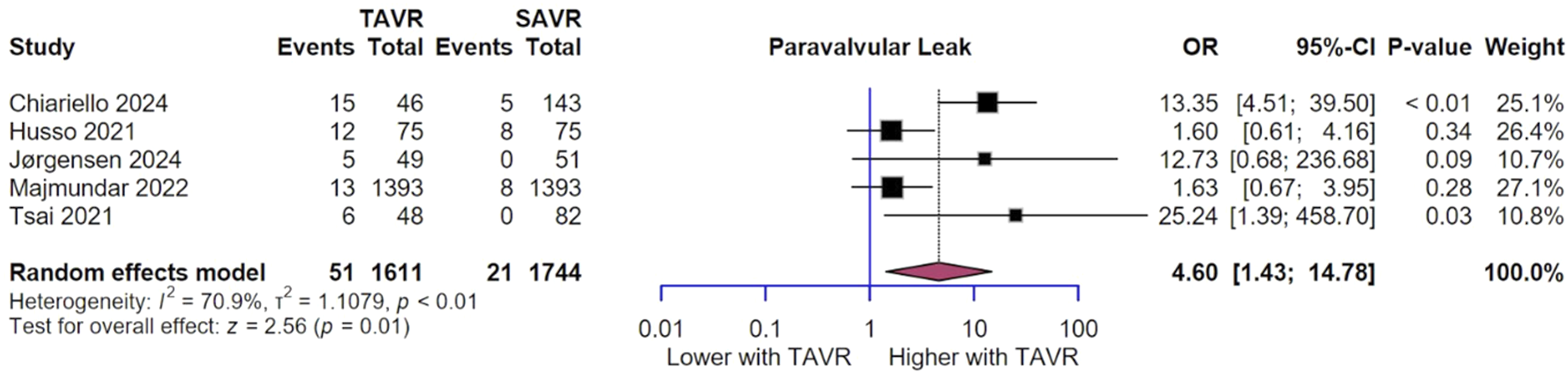
Discussion
Summary of findings
In this meta-analysis, we included 14 studies with 78,677 patients having bicuspid aortic valves and aimed to compare the safety and efficacy outcomes of TAVR and SAVR in this group. We found that TAVR was associated with a significantly higher risk of PPI compared to SAVR and this result was consistent during in-hospital and short-term follow-ups. However, there were no significant differences in all-cause mortality and stroke at follow-up. However, on subgrouping stroke outcome by follow-up duration, long-term stroke incidence was higher in the TAVR group. TAVR was superior to SAVR in reducing the risk of major bleeding and the length of hospital stay, however, it was associated with a significantly higher risk of PVL. We found no significant differences in the rates of MI, AKI, vascular complications, and the need for valve reintervention.
Interpretation of findings
There are still concerns regarding the use of TAVR in BAV patients for some technical and anatomical issues. The lifelong care of patients with AS is affected by the fact that BAV patients usually develop AS at a younger age, and are at reduced surgical risk than those with senile calcific tricuspid AS. 21 Also, it should be taken into account that there is still a lack of long-term data on TAVR. Further, the entire valve expansion in TAVR that could be potentially prevented by the non-circular orifice of BAV combined with more calcified and asymmetrical leaflets, may limit appropriate and circular expansion. 21 For younger, operable patients with severe BAV stenosis, SAVR is currently the gold standard. TAVR has, however, lately been suggested for BAV patients, and encouraging outcomes have been documented.22–24 The use of TAVR in BAV patients is not explicitly recommended by current guidelines, which typically advise surgery for younger patients with severe and symptomatic AS. 25
The NOTION-2 trial was the first to compare TAVR and SAVR in patients ≤75 years of age without excluding BAV. 26 BAV stenosis is more typically found in young individuals, hence, it is critical to include it in a trial comparing both treatment modalities in a young population. 27 In the surgical group, individuals with BAV had a lower primary event rate (3.9%) compared to those with tricuspid valves (8.3%). 26 BAV stenosis patients may have a lower cardiovascular risk because of their younger age. 27 However, given the small size of the bicuspid AS cohort in the NOTION-2 trial, 26 it may be possible that the observed results are affected to some degree by coincidence. TAVR was associated with lower rates of new-onset atrial fibrillation and significant bleeding compared to SAVR, as observed in earlier trials. Other reported unfavorable outcomes by previously published studies such as PPI and PVL supported surgery.9,28–30
Recent data from the Society of Thoracic Surgeons/American College of Cardiology Transcatheter Valve Therapies (STS/ACC TVT) registry compared 2,691 matched BAV patients with an equal number of patients who had a tricuspid valve and were deemed intermediate or high risk for open-heart surgery and underwent TAVR. 31 All-cause death rates were comparable after 30 days (2.6% vs 2.4%) and 1 year (10.8% vs 12.1%) after the intervention. 31 Individuals with a BAV had a 50% increased incidence of stroke after 30 days as of 2.4% compared to 1.6% for tricuspid cases. 31
Kaang et al. reported similar rates of in-hospital mortality and stroke. Similar to our findings, they reported that patients who underwent TAVR had higher rates of PPI and PVL. 32 On the other hand, patients who underwent TAVR displayed lower rates of AKI, major bleeding, and pulmonary complications. 32 A more recent meta-analysis found that TAVR was associated with a much lower risk of major bleeding but a higher risk of PPI, which supports our findings. The authors found no significant differences in 30-days or mid-term mortality, stroke, major vascular complications, AKI, PVL, or conduction abnormalities.
In line with our results, other research has shown a comparable 30-days mortality and stroke rate following risk adjustment, indicating that TAVR is safe for certain bicuspid AS in current practice.33–36 But compared to SAVR, TAVR was consistently linked to a noticeably greater rate of new PPI. According to Chen et al., the incidence of PPI was 9.2% in TAVR and 6.3% in SAVR. 35 This risk should be taken into account when comparing young patients with bicuspid anatomy, who have a low surgical risk for TAVR against SAVR.
Similar to other authors, Chiariello et al. 37 discovered that the TAVR group had a greater incidence of PPI and PVL as presented in our study.38,39 However, the selection criteria, which included older age and worse baseline clinical conditions of patients in the TAVR group, should be regarded as a limitation in the comparison of the two groups. Chiariello et al. also reported that SAVR had greater long-term survival and improvement of clinical status. 37 Higher PVL in TAVR may explain our observation of an increased stroke rate at long-term follow-up. A prior study demonstrated that platelets had the ability to enter PVL channels several times across subsequent cardiac cycles, increasing the thrombogenic risk of modest PVL flows. 40 The authors found that this thrombogenic potential is determined by patient-specific PVL channel characteristics and morphologies, rather than the clinical classification of PVL. 40 According to a previous study, 36 PPI was more common in TAVR patients than in SAVR patients, but lower than in a major systematic study of non-BAV TAVR patients, which found a prevalence of 17%.41,42 Preprocedural atrioventricular conduction block and intraprocedural block are known indicators of a higher chance of PPI. Along with a higher risk of annular disruption, TAVR can adversely cause higher rates of post-procedural PVL and PPI.23,33,34 These structural issues led to the original exclusion of BAV patients from TAVR trials.23,36,43,44 However, recent prospective and retrospective investigations have shown that TAVR has the potential to help certain BAV patients, and medium-term studies have shown comparable or superior durability. 45
Sanaiha et al. reported that although BAV patients were admitted for shorter periods of time, TAVR led to a substantial increase in expenses. 36 The intrinsic cost discrepancies between prosthesis utilized in open and transcatheter cases, as well as variations in preprocedural diagnostic and catheterization laboratory fees, are probably the cause of this cost disparity. 46 Other studies comparing the costs of SAVR and TAVR that have indicated a persistent discrepancy in hospitalization expenses because of TAVR device-related expenditures are considered a limitation that can present in our findings supporting TAVR. 47
Strengths, limitations, and recommendations
To our knowledge, this is the most comprehensive and updated meta-analysis comparing SAVR and TAVR in patients with BAV stenosis with the largest sample size. The majority of included studies had an observational study design, which might be a limitation of our study. Also, the lack of long-term follow-up limits the conclusion of our study. Future large-scale RCTs are needed to support these findings with long-term follow-up.
Clinical implications and future directions
While SAVR remains the recommended treatment for lower-risk individuals with BAV stenosis, our findings suggest that TAVR is a feasible and safe option for certain patients, particularly those who are older or have a higher surgical risk, with advantages like less bleeding and shorter hospital stays. The 2025 ESC/EACTS guideline recommends TAVR for older patients (≥75), those at high risk (STS-PROM/EuroScore II >8%), and those unsuitable for surgery. 48 For BAV, SAVR is recommended for patients with AS affecting the BAV and associated disease. 48
Regarding the increased risks of PPI and PVL with TAVR, heart teams must carefully weigh these issues, particularly for younger patients who bear a lifetime of life-long risk from these complications.
Conclusion
Our data indicate that in patients with BAV stenosis, TAVR is a less invasive option than SAVR, with comparable short-term mortality and stroke rates. TAVR also offers benefit by minimizing significant bleeding and hospital length of stay. However, the benefits should be balanced against the considerably increased risk of PPI and PVL. However, these findings are limited by the observational nature of the available data and the absence of long-term findings. A multidisciplinary heart team must decide between TAVR and SAVR based on particular patient factors.
Supplemental material
Supplemental material - Safety and efficacy of transcatheter aortic valve replacement (TAVR) vs. surgical aortic valve replacement (SAVR) in patients with bicuspid aortic stenosis: A Systematic review and meta-analysis
Supplemental material for Safety and efficacy of transcatheter aortic valve replacement (TAVR) vs. surgical aortic valve replacement (SAVR) in patients with bicuspid aortic stenosis: A Systematic review and meta-analysis by Ahmed Farid Gadelmawla, Ahmed Mansour, Ahmed Elbataa, Osama Hamdi Asiri, Amnah Ali Alharbi, Fatimah Ashraf Alqurais5, Fatem Saleh Al-Ibrahim, Abdulaziz Fahad AlHasani, Turki Nashi Alharbi, Ruba Mohammed AL Murayyi, Abdulelah Ghazi Alotaibi, Hamza A. Abdul-Hafez and Ihab Suliman in Perfusion
Footnotes
Author contributions
A.F.G.: Conceptualization, data curation, writing review/editing; A.M.: methodology, validation; A.E.: formal analysis, software; O.H.A.: methodology, writing original draft; A.A.A.: methodology, writing original draft; F.A.A.: methodology; F.S.A.: methodology; A.F.A.: methodology; T.N.A.: methodology; R.M.A.: methodology; A.G.A.: methodology; H.A.H.: writing original draft; I.S.: project administration, supervision.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All required data are included in the manuscript or the supplementary material. Any additional data can be obtained from the corresponding author upon a reasonable request.
Supplemental material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.