
Abstract
Wiskott-Aldrich syndrome (WAS) is an X-linked genetic disorder characterised by eczema, immunodeficiency, and thrombocytopenia. Cardiopulmonary bypass causes a reduction in platelet numbers and function leading to an increased risk of bleeding. We report a case of a 33 year old male with WAS who underwent a redo ascending aorta and total aortic arch replacement as part of a two stage surgery for a Type B aortic dissection. The report discusses the considerations given to cardiopulmonary bypass in order to mitigate platelet number reduction and the degree of systemic inflammatory response. Post operative viscoelastometry indicated a minor hypocoagulopathy with minimal post-operative bleeding.
Keywords
Introduction
Wiskott-Aldrich syndrome (WAS) is a rare X-linked genetic disorder which is characterised by immune deficiency, impaired platelet numbers and function, and eczema. 1 Primarily affecting males, the incidence of this disease is between 1 and 10 cases per million males worldwide. 2 There is also growing evidence of a relationship between immune dysregulation observed in some WAS patients and vasculitis, which includes development of aneurysms in the abdominal and thoracic aorta. 3 Cardiopulmonary bypass has a deleterious effect on coagulation primarily affecting platelet numbers and function which can increase the risk of bleeding post-operatively.
Case report
A 33 years male with Wiskott-Aldrich Syndrome (WAS) presented with a chronic Type B aortic dissection which had migrated into the distal arch causing progressive dilatation of a residual aneurismal aorta. The patient had undergone repair of a Type A dissection 4 years previously with a mechanical aortic valve and root replacement. The plan was to repair the dissection in two stages. The first stage, and the subject of this case report, was to perform a redo ascending aorta and total arch replacement using frozen elephant trunk procedure.
The patient’s previous medical history included: pneumococcal septicaemia with multiorgan failure leading to bilateral below-the-knee amputations and fingertip amputations; stage 5 chronic kidney disease; and a splenectomy at the age of five. The patient was also undergoing immunoglobulin therapy to address his immunodeficiency.
A Medtronic cardiopulmonary bypass circuit was used which included a Cortiva®-coated Fusion® oxygenator (Medtronic Inc., Minneapolis, MN). The prime consisted of 800 ml Plasma-Lyte 148, 500 ml Albumin, 150 ml Mannitol, and 10,000IU unfractioned heparin. Antegrade and retrograde autologous priming was utilised to mitigate blood dilution and preserve platelet numbers. A pre-operative haemoglobin of 122 g/L dropping to 107 g/L on bypass indicated a estimated prime volume of 780 ml. Haemoglobin remained above 100 g/L throughout the case.
Cannulation was through the left femoral vein and the left subclavian artery via a 10 mm Vascutek Gelsoft™ graft (Inchinnan, Scotland UK). Full flow was targeted at 2.4 L/min/m2 with a mean arterial pressure of 60–70 mmHg. Total bypass time was 155 min which included a period of moderate hypothermic circulatory arrest lasting 35 min at a core body temperature of 25°C. Cross clamp time was 76 min with myocardial protection provided in the form of 4:1 high strength cardioplegia.
Selective antegrade cerebral perfusion (SACP) was instituted through the left carotid and brachiocephalic arteries with 13Fr and 15Fr Medtronic Gundry® (Minneapolis, MN) retrograde cardioplegia cannulae respectively. Flow was targeted at 10 ml/kg/min (pre-amputation weight) using bilateral near-infrared spectroscopy to monitor adequate cerebral protection. SACP lasted 51 min which spanned the circulatory arrest period and the resumption of flow to lower body once distal anastamosis of the new graft was complete. The rate of cooling and rewarming was limited to <0.3°C per minute with no more than a 10°C gradient between heater cooler unit and patient temperature to ensure homologous heat transfer.
Weaning from bypass was uneventful and without inotropic support. A total of 500 ml of Plasma-Lyte 148 was added throughout the case and 650 ml was filtered giving a total fluid balance on bypass of −150 ml. Urinary output was negligible due to renal failure.
Coagulation was assessed using the viscoelastometry analyser ClotPro® (Haemonetics®, Boston MA) pre- and post-operatively (Figure 1). Three units of fresh frozen plasma, two units of cryoprecipitate, and one pooled unit of platelets were transfused post-operatively according to local protocol for circulatory arrest cases. Post protamine ACT was within range of baseline value. Chest drain output at 8 h post-op was 200 ml. The patient was extubated 8 h post-operatively and received one unit of red blood cells the following day. He was discharged from ICU 8 days post-operatively. Pre-operative (a, b and c) and post-operative (d, e and f) ClotPro® (Haemonetics®, Boston Massachusetts) viscoelastometry testing using reagents to assess coagulation of extrinsic pathway (Channel 1), the functional qualitative fibrinogen level (Channel 2), and the coagulation of the intrinsic pathway (Channel 3).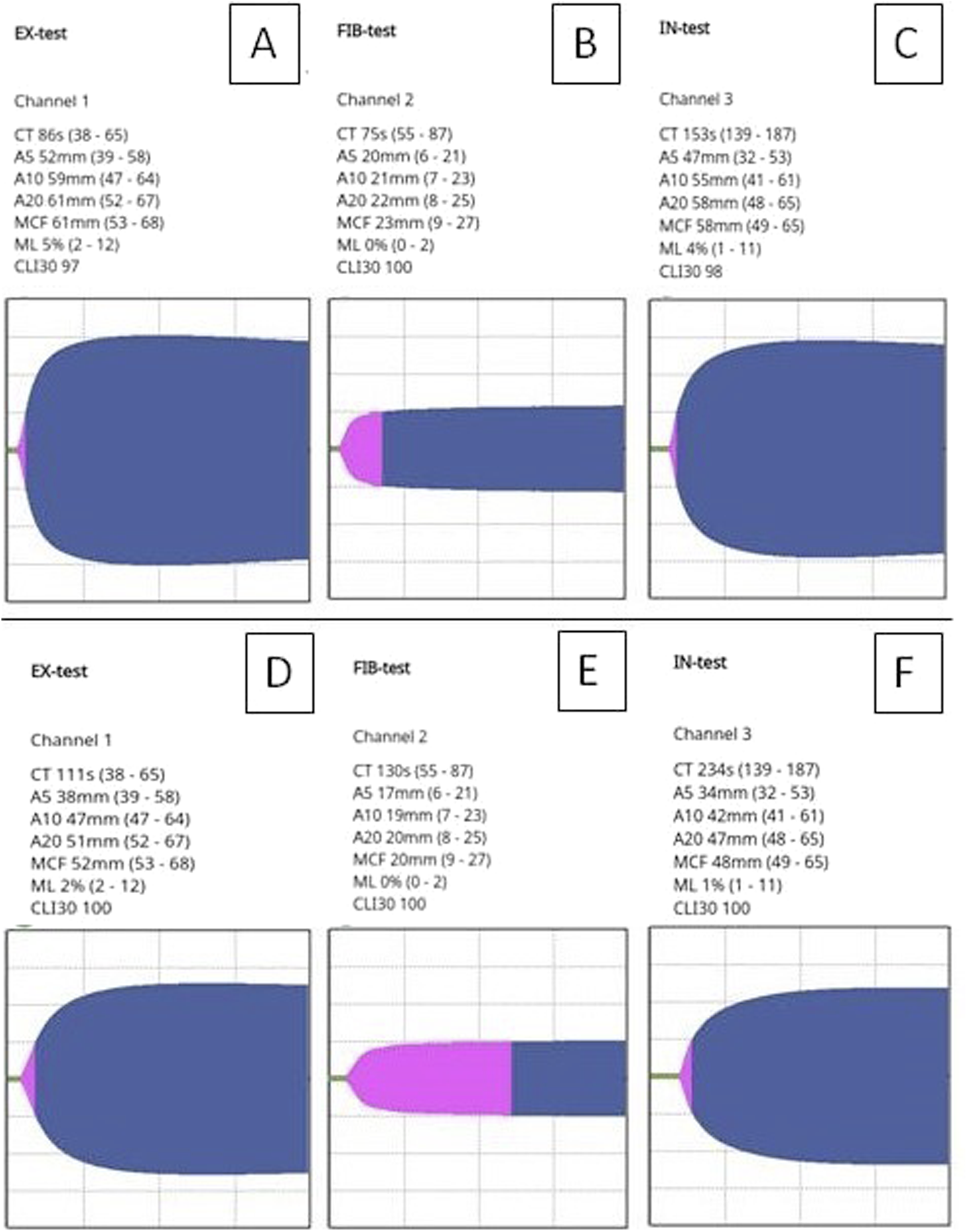
Discussion
Hypothermia is necessary when instituting circulatory arrest to provide adequate organ protection by reducing oxygen metabolism but this has deleterious effects on coagulation and increases the risk of haemorrhage.4,5 Bernabeu and colleagues 6 describe an aortic arch replacement performed on a patient with WAS at 32°C whilst maintaining lower body perfusion via the femoral artery and SACP in order to preserve clotting function. Continuous lower body perfusion was not possible for this case, however; moderate hypothermic circulatory arrest at 25°C with SACP does show favourable outcomes including coagulation and neurological effects compared with circulatory arrest at lower temperatures. 7
There is limited evidence to suggest that heparin-coated surfaces of extra-corporeal circuitry can lead to preserved platelet numbers and function, in addition to a reduction in blood product transfusion, compared with standard circuitry components.8–10 Only the oxygenator was Cortiva® coated due to logistical issues sourcing a fully coated circuit, however; it was anticipated that this would still be beneficial as the oxygenator is the source of the majority of platelet adsorption during cardiopulmonary bypass. 11
A splenectomy is a common form of treatment for patients with WAS in order to preserve platelet numbers, however; a significant portion of remaining platelets are classed as microplatelets which impair overall platelet function and this was evident to an extent in the ClotPro® results. Although the patient’s platelet numbers preoperatively were normal (159,000/µL), and the pre-operative viscoelastometry of the extrinsic and intrinsic pathway showed a maximal clot formation (MCF) within the normal range (Figure 1(a) and (c)), the influence of functional fibrinogen level is an important consideration. Figure 1(b) shows a fibrinogen MCF above 20 mm (23 mm) which is indicative of overcompensation of fibrinogen in clot formation and a reduced platelet function. The clot time within the extrinsic pathway (Figure 1(a)) was also extended most likely due to residual warfarin which was stopped 5 days prior to the operation according to protocol. 12
Viscoelastometry post-operatively (Figure 1(d)–(f)) confirmed a more pronounced general coagulopathy of an extended clotting time.
Conclusion
This case report describes a favourable outcome of major aortic surgery in a WAS patient by tailoring cardiopulmonary bypass strategy with respect to the coagulopathic concerns of the disease. This is illustrated by an uneventful weaning from cardiopulmonary bypass and an uncomplicated ICU stay post operatively. In contrast to the few other reported cases of major aortic surgery in patients with WAS,13,14 blood product transfusion and post-operative bleeding was minimal.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.