
Abstract
Introduction
Standard anticoagulation protocols for patients with trauma-related acute respiratory distress syndrome (TR-ARDS) undergoing venovenous extracorporeal membrane oxygenation (VV-ECMO) are often inapplicable due to high bleeding risks. This study evaluated the safety and feasibility of a prolonged anticoagulation-free strategy (≥72 h) in patients with severe trauma.
Methods
We retrospectively reviewed 37 patients with blunt TR-ARDS at a Level 1 Trauma Center (2016–2024). Patients were categorized into an anticoagulation-free group (withheld ≥72 h; n = 18) and an anticoagulation group (n = 19).
Results
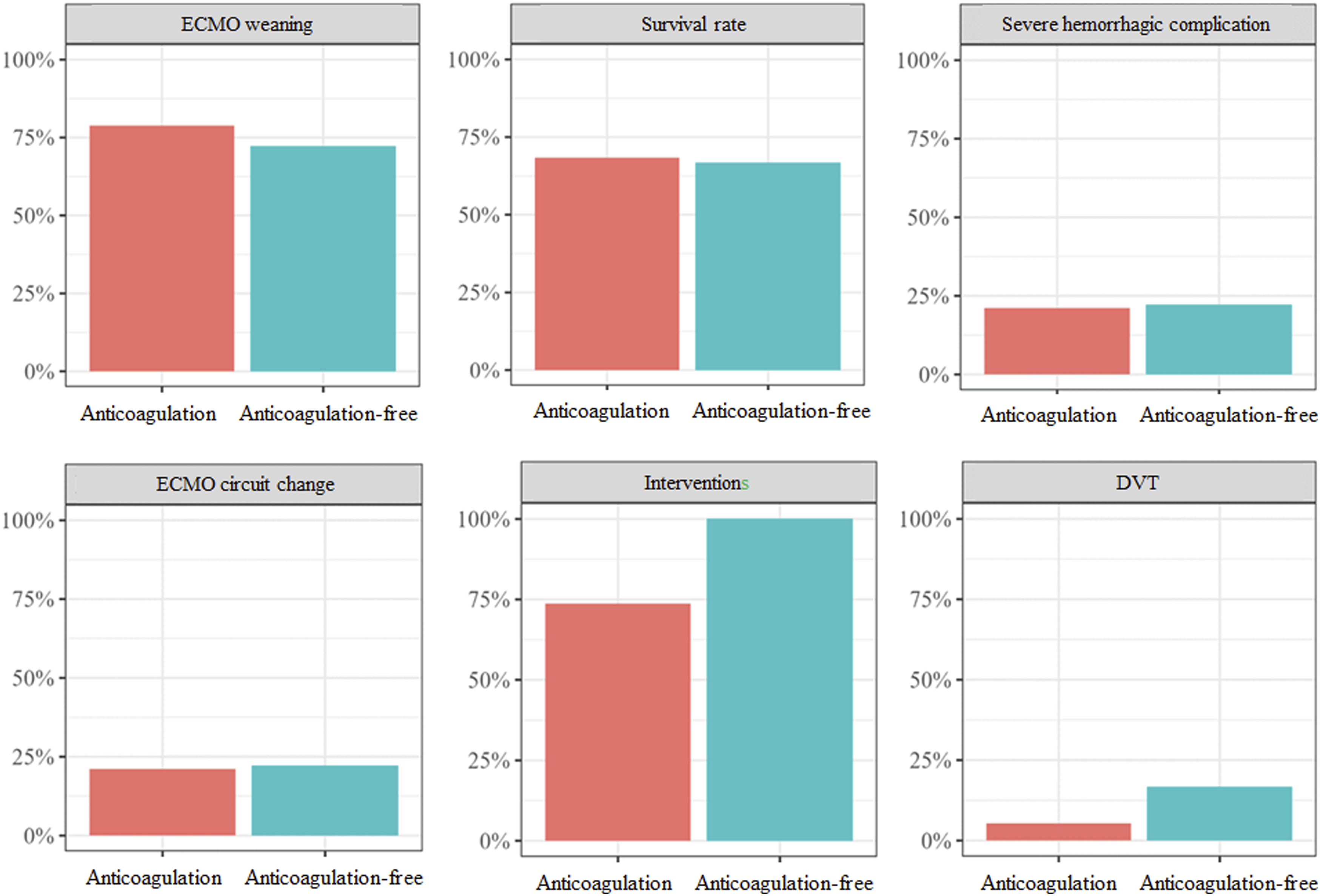
Clinical outcomes, including survival (66.7% vs 68.4%, p = 1.000), VV-ECMO weaning, and hemorrhagic/thrombotic complications, were comparable between groups. Notably, the anticoagulation-free group exhibited significantly higher baseline severity, with lower Glasgow Coma Scale and Trauma and Injury Severity Score scores and more pronounced initial coagulopathy (prolonged PT, lower fibrinogen levels). Despite this, 12 of 18 patients (66.7%) in the anticoagulation-free group successfully completed their entire VV-ECMO course without any systemic anticoagulation, with no increase in circuit-related complications.
Conclusions
Our findings suggest that withholding systemic anticoagulation for ≥72 h is a safe and feasible strategy for high-bleeding-risk trauma patients. This risk-adapted approach, prioritizing hemorrhage control, does not compromise patient safety or device integrity in selected patients with severe trauma and TR-ARDS. Larger multicenter prospective studies should validate this risk-stratified management framework.
Keywords
Introduction
Acute respiratory distress syndrome (ARDS) develops in approximately 4.6% of trauma patients, carrying a high mortality rate ranging from 30% to 80%.1–3 Venovenous extracorporeal membrane oxygenation (VV-ECMO) has increasingly been used as a life-saving salvage therapy when optimal mechanical ventilation fails to achieve adequate oxygenation.1–4
Although systemic anticoagulation is generally required to prevent circuit and patient thromboembolism, it significantly increases hemorrhagic complications, which account for up to 23% of deaths.2,5 Maintaining an appropriate balance between thrombosis and bleeding is particularly challenging in trauma patients due to acute hemorrhage and trauma-induced coagulopathy (TIC).2,5 Consequently, evidence-based anticoagulation management models remain limited for this population.
According to the Extracorporeal Life Support Organization (ELSO) guidelines, anticoagulation may be delayed for 24–48 h in patients with high bleeding risks, as achieving definitive hemostasis is critical during the initial early stabilization period.6–8 Furthermore, modern biocompatible, heparin-coated circuits may maintain patency without exogenous heparin during this window. However, the safety and feasibility of a prolonged anticoagulation-free strategy beyond this immediate phase remain uncertain.7–10
Therefore, this study evaluated the safety and clinical feasibility of a prolonged anticoagulation-free strategy (≥72 h) in severely injured patients. We hypothesized that higher trauma severity and initial coagulopathy would drive the clinical decision to withhold anticoagulation, and that this prolonged withholding strategy would achieve clinical outcomes comparable to standard therapy without increasing thrombotic complications.
Methods
Study design
This study’s primary aim was to compare clinical outcomes between two groups of patients with TR-ARDS who underwent VV-ECMO, categorized by whether systemic anticoagulation was initiated within the first 72 h of support. Specifically, patients were divided into an anticoagulation-free group (withheld for ≥72 h) and an anticoagulation group (initiated within <72 h). The secondary aim was to explore trends in patient characteristics and clinical indicators associated with the decision to withhold anticoagulation. We retrospectively reviewed patients with TR-ARDS who underwent VV-ECMO at a regional trauma center in South Korea between January 2016 and December 2024.
Inclusion criteria were age ≥18 years and VV-ECMO support for ≥24 h. Of the patients who received ECMO during the study period, those who received VV-ECMO specifically for TR-ARDS were eligible for inclusion. Exclusion criteria included venoarterial (VA) ECMO performed for extracorporeal cardiopulmonary resuscitation (E-CPR) or heart failure, and VV-ECMO applied as a rescue strategy for conditions such as tracheal stenosis-related respiratory failure. Exclusion criteria included non-survivable traumatic injuries (such as irreversible brain herniation) and irreversible underlying medical conditions (e.g., terminal-stage malignancies or end-stage organ failure) where ECMO support was deemed futile. Notably, patients with intracranial hemorrhage (ICH) were not automatically excluded if the bleed was considered controllable or stable; in these instances, VV-ECMO was initiated using an anticoagulation-free protocol to balance the need for respiratory support with the risk of hemorrhagic progression. Additional exclusion criteria are shown in Figure 1. Therefore, we established a 72-h threshold from the initiation of ECMO to categorize the study groups. Specifically, patients in whom anticoagulation could not be initiated within the first 72 h because of active bleeding or a severe bleeding tendency were classified as the anticoagulation-free group, while those in whom anticoagulation could be initiated and maintained within this 72-h window were classified as the anticoagulation group. Flowchart of patient selection.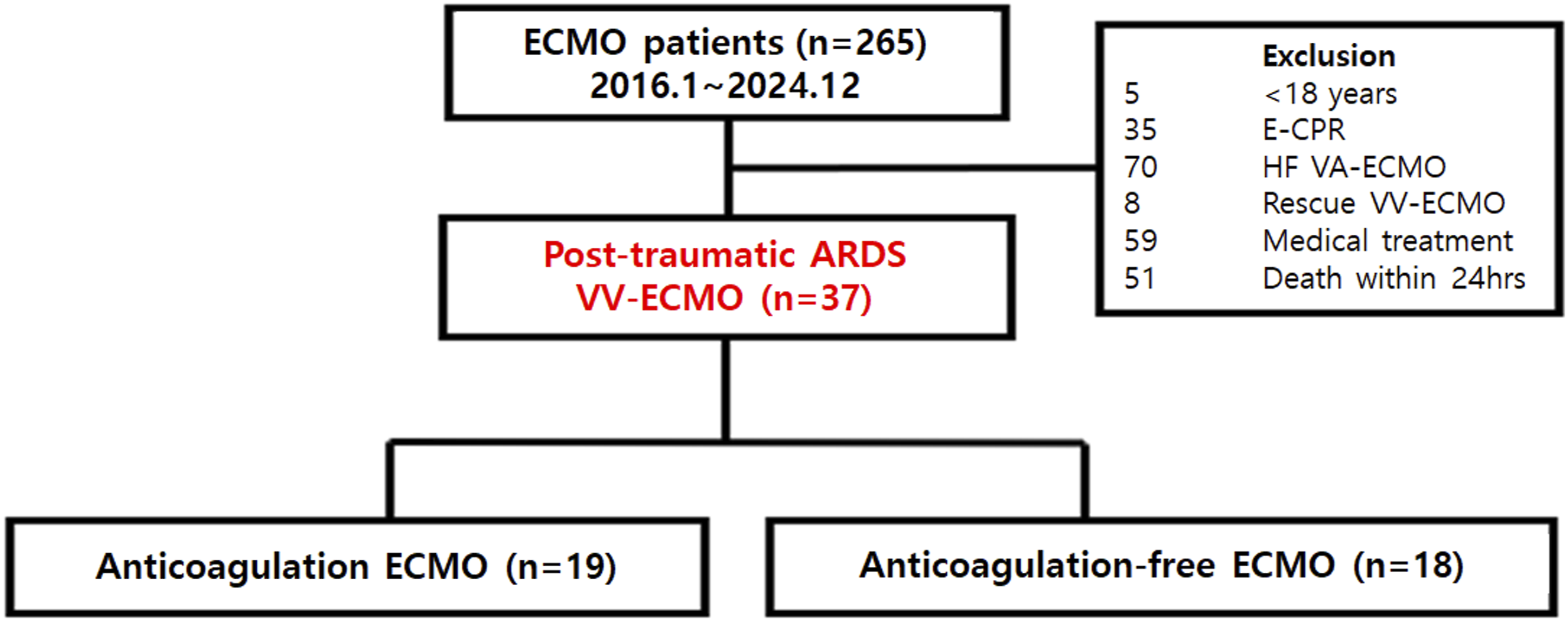
At our institution, a low-dose anticoagulation protocol is routinely applied for trauma patients. Patients in whom anticoagulation was withheld for ≥72 h were compared with those in whom anticoagulation could be maintained. Clinical characteristics, laboratory findings, trauma severity scores, survival rates, length of hospital stay, ECMO weaning, and complications were compared between the two groups. Pre-ECMO and peri-ECMO variables demonstrating statistically significant trends were evaluated to explore their relevance to the application of an anticoagulation-withholding strategy.
Indications for VV-ECMO
VV-ECMO was applied according to the ELSO guidelines. ECMO was initiated in patients with persistent hypoxemia, hypercapnia, or respiratory acidosis despite appropriate mechanical ventilation. ECMO cannulation was considered when the PaO2/FiO2 ratio remained ≤80 for >6 h with an FiO2 of ≥0.9, accompanied by radiologic findings consistent with ARDS, including bilateral opacities on chest radiography or computed tomography (CT) according to the Berlin criteria. In our study population, all subjects met these stringent physiological and radiological criteria. Specifically, the mean pre-ECMO PaO2/FiO2 ratio was 53.61 ± 14.50 mmHg. Although the mean arterial pH was maintained at 7.31 ± 0.08 through aggressive pre-ECMO stabilization and physiological compensation, the profound hypoxemia remained refractory, strictly necessitating VV-ECMO support. Furthermore, all included patients demonstrated significant radiological opacification (white-out) involving at least two out of four quadrants on chest radiography prior to cannulation.
Contraindication for ECMO
At our trauma center, contrast-enhanced CT is routinely performed as an initial evaluation in trauma patients. ECMO was not initiated in cases where CT demonstrated intracranial hemorrhage or other non-recoverable comorbid conditions. However, if the hemorrhage was deemed controllable, ECMO could still be considered.
ECMO management
ECMO cannulation was typically performed bedside in the intensive care unit using ultrasound-guided Seldinger techniques via the internal jugular vein and femoral vein or via bilateral femoral venous access. Transfusion thresholds varied slightly among clinicians but were generally maintained at hemoglobin levels >10 g/dL and platelet counts >80,000/mm3. Mechanical ventilation followed a lung-protective strategy using low tidal volumes with a respiratory rate of 6–8 breaths/min. Tracheostomies were performed when mechanical ventilation was expected to exceed 2 weeks. To optimize oxygenation and circuit patency, ECMO blood flow was titrated to maintain a SpO2 of 88–92% and a PaO2 of at least 70 mmHg. Sweep gas flow was initially set at a 1:1 ratio with the blood flow rate and subsequently adjusted based on serial arterial blood gas analysis (ABGA) to maintain PaCO2 within the normal physiological range. While a formal routine screening protocol for deep vein thrombosis (DVT) was not implemented at our institution, targeted venous ultrasonography was practically performed for all patients following decannulation to assess the cannulation sites. Additionally, in cases of clinical suspicion or for multiple trauma patients requiring periodic follow-up CT scans (chest or abdomen) for injury monitoring, the presence of DVT or pulmonary thromboembolism (PTE) was actively evaluated through these imaging studies. This approach allowed for the identification of both clinically apparent cases and silent thrombotic events detected during routine trauma surveillance.
Center’s anticoagulation guidelines
Our trauma center generally applies a low-dose unfractionated heparin protocol during VV-ECMO. Anticoagulation protocols were adjusted according to individual patient conditions, targeting an activated partial thromboplastin time (aPTT) of 50–70 s and an activated clotting time (ACT) of 130–150 s. In patients with active bleeding or severe bleeding tendencies, anticoagulation was either not initiated or discontinued. The same anticoagulation principles were applied to both groups in this study. In patients with a high risk of bleeding or active hemorrhage, the systemic heparin bolus typically administered during cannulation was selectively withheld to ensure definitive hemostasis and prevent hemorrhagic progression.
Initial heparin bolus administration was not considered as a study variable, as the commonly used bolus dose (50–100 U/kg) is generally expected to be cleared from circulation within several hours and may not influence subsequent anticoagulation status. Anticoagulation was resumed when hemorrhage was shown to be controlled on follow-up CT imaging, surgical drain output had decreased, or the coagulopathies had stabilized.
Data collection
Clinical data were obtained from the institution’s electronic medical records. This study was approved by the Institutional Review Board of Pusan National University Hospital (IRB No. 2310-037-132), and the need for informed consent was waived owing to the study’s retrospective design.
Collected variables included age, sex, ECMO type, ECMO indication, ECMO support duration, trauma severity scores, and coagulation laboratory values. Outcomes compared between the two groups included hemorrhagic events, thromboembolic events, transfusion volume, ECMO weaning, hospital length of stay, and survival. In this study, survival was defined as survival to hospital discharge. This required that the patient not only be successfully weaned from VV-ECMO support but also complete all required surgical and medical interventions for their traumatic injuries, leading to a stable discharge from the hospital.
Coagulation parameters—such as PT, aPTT, ACT, D-dimer, hemoglobin, platelet count, and fibrinogen levels—were routinely measured every 4–6 h before and after ECMO initiation, and more frequently when clinically indicated (e.g., active bleeding). Pre-ECMO laboratory values were defined as values obtained within 6 h before cannulation.
Trauma severity assessment included Glasgow Coma Scale (GCS) scores, Revised Trauma Scores (RTSs), Injury Severity Scores (ISSs), Trauma and Injury Severity Scores (TRISSs), Respiratory ECMO Survival Prediction (RESP) scores, and Acute Physiology and Chronic Health Evaluation (APACHE) scores.
Statistical analyses
All p-values <0.05 were considered statistically significant. Continuous variables were analyzed using the independent t-test or Wilcoxon rank-sum test, and categorical variables were analyzed using the chi-squared or Fisher’s exact tests, as appropriate. All statistical analyses were performed using R statistical software (version 4.3.1; R Core Team, 2024).
Results
Among the 265 patients who received ECMO support during the study period, 37 met the inclusion criteria and none of the exclusion criteria outlined in Figure 1, and were included in the final analysis (19 in the anticoagulation group and 18 in the anticoagulation‐free group).
Patient demographics and traumatic severity score data.
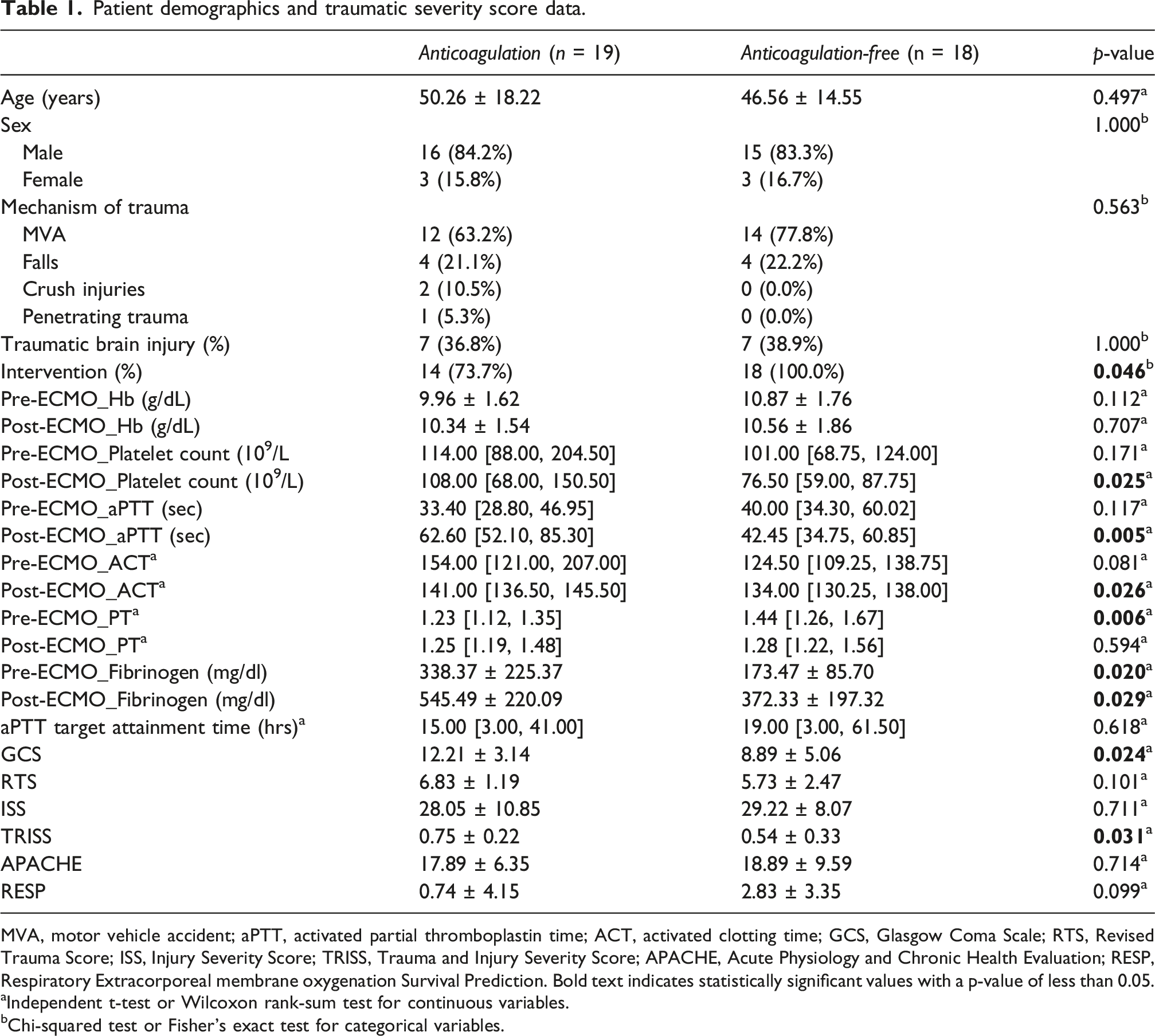
MVA, motor vehicle accident; aPTT, activated partial thromboplastin time; ACT, activated clotting time; GCS, Glasgow Coma Scale; RTS, Revised Trauma Score; ISS, Injury Severity Score; TRISS, Trauma and Injury Severity Score; APACHE, Acute Physiology and Chronic Health Evaluation; RESP, Respiratory Extracorporeal membrane oxygenation Survival Prediction. Bold text indicates statistically significant values with a p-value of less than 0.05.
aIndependent t-test or Wilcoxon rank-sum test for continuous variables.
bChi-squared test or Fisher’s exact test for categorical variables.
Table 1 also presents the trauma severity scores comparison. The anticoagulation-free group showed significantly lower GCS and TRISS scores. Although the proportion of patients with GCS scores ≤8 was similar between the two groups, the proportion with a TRISS <0.5, indicating lower predicted survival, was higher in the anticoagulation-free group. No significant differences were observed in RESP scores.
Patient outcomes.
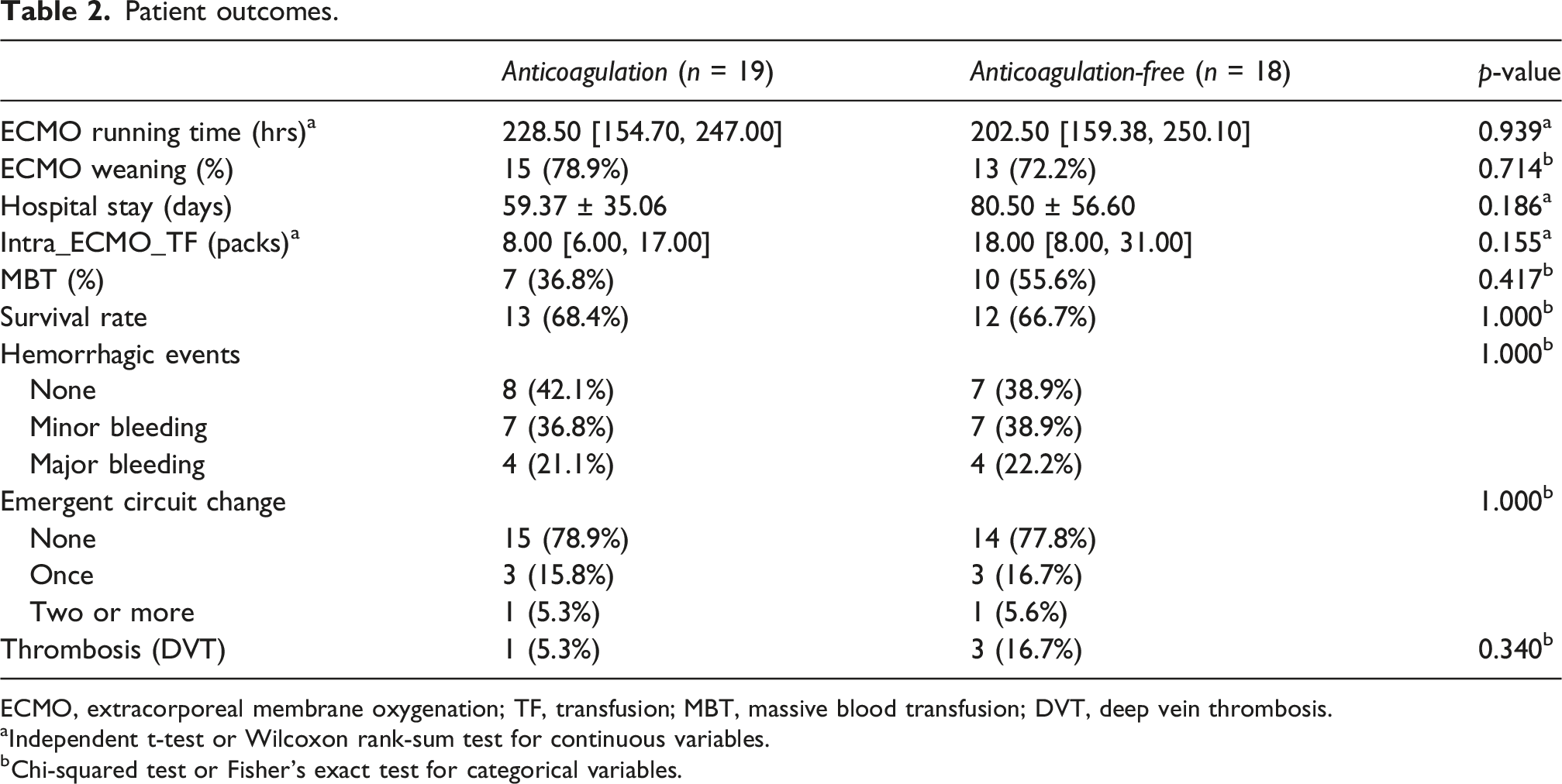
ECMO, extracorporeal membrane oxygenation; TF, transfusion; MBT, massive blood transfusion; DVT, deep vein thrombosis.
aIndependent t-test or Wilcoxon rank-sum test for continuous variables.
bChi-squared test or Fisher’s exact test for categorical variables.
The demographic and clinical characteristics of the two groups are shown in Figure 2, and primary treatment outcomes are shown in Figure 3. Significant differences in baseline coagulopathy and severity between groups. Comparison of clinical outcomes between the anticoagulation and anticoagulation-free groups. Survival rate represents survival to hospital discharge.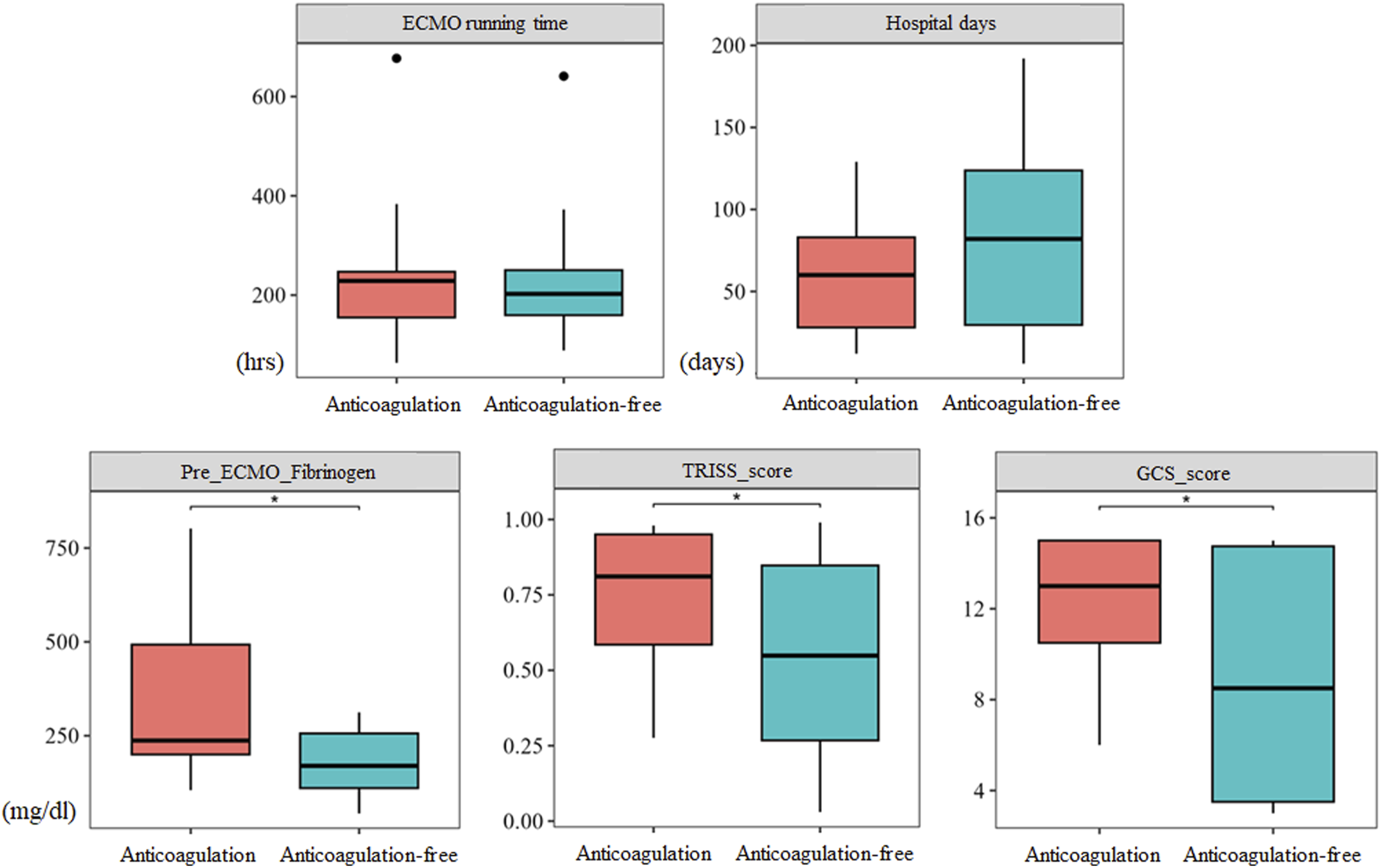
Anticoagulation-free ECMO group information.
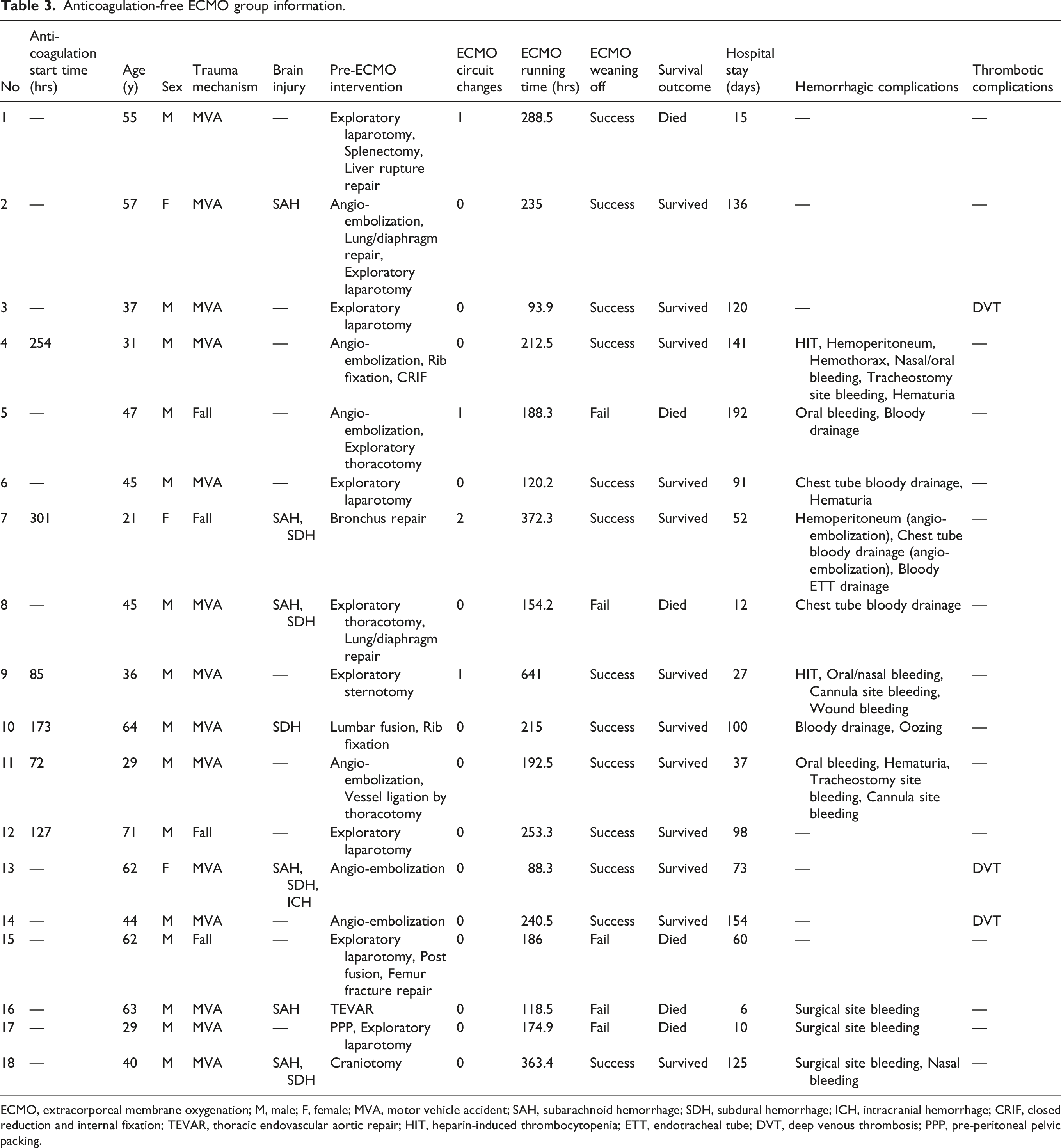
ECMO, extracorporeal membrane oxygenation; M, male; F, female; MVA, motor vehicle accident; SAH, subarachnoid hemorrhage; SDH, subdural hemorrhage; ICH, intracranial hemorrhage; CRIF, closed reduction and internal fixation; TEVAR, thoracic endovascular aortic repair; HIT, heparin-induced thrombocytopenia; ETT, endotracheal tube; DVT, deep venous thrombosis; PPP, pre-peritoneal pelvic packing.
Subgroup analysis of completely anticoagulation-free patients
A secondary subgroup analysis was performed on patients who remained anticoagulation-free throughout the entire ECMO duration (n = 12, 32.4%). The mean duration of ECMO support in this subgroup was 187.6 ± 82.8 h. When comparing this group to the anticoagulated group (n = 25), the circuit exchange rate did not show a significant increase (16.7% vs 24.0%, p = 1.000). Survival to discharge (50.0% vs 76.0%, p = 0.146) and successful weaning rates (58.3% vs 84.0%, p = 0.116) showed no statistically significant differences between the completely anticoagulation-free group and the anticoagulated group.
Discussion
This study demonstrates that a prolonged anticoagulation-free strategy (beyond 72 h) is safe and feasible for severe trauma patients with TR-ARDS requiring VV-ECMO. While anticoagulation is traditionally considered essential for ECMO management, evidence-based guidelines for the trauma population remain undefined. Applying medical ARDS protocols to trauma patients often overlooks the critical risks of hemorrhagic shock and uncontrolled injuries. 7 Given that mortality among patients with TR-ARDS remains extremely high, ranging from 30% to 80%,3,10,11 there is a critical need for viable salvage strategies. Consequently, we hypothesized that an anticoagulation-withholding strategy could maintain clinical efficacy while minimizing hemorrhagic complications, and our comparative analysis supports the safety and viability of this approach.
Our findings regarding complication rates are consistent with global registry data and existing literature. The ELSO registry (2010–2017, n = 7,579) reported that 40.2% of VV-ECMO patients experience at least one complication, with thrombotic events accounting for 54.9%. Furthermore, a 2022 ELSO analysis noted a complication rate of approximately 40% in adults, with thrombosis occurring in 22%. 12 Olson et al. reported a total thrombosis incidence of 22.9% (13.4% circuit-related and 9.5% patient-related) and a major bleeding rate of 27.9% in anticoagulation-free ECMO. 13 Furthermore, in a meta-analysis comparing low-dose versus standard-dose regimens, Lv et al. found no significant difference in thrombotic complications between the two strategies, while noting that gastrointestinal and surgical-site bleeding were significantly less frequent in the low-anticoagulation group. 14 These developments align with the increasing clinical utilization of low-dose anticoagulation or withholding strategies as clinical experience accumulates.5,6,10 In this context, our observed total thrombosis rate of 27% and major bleeding rate of 21.8% fall within expected international ranges, especially considering the higher baseline trauma severity of our cohort. 12
A particularly noteworthy finding from our secondary subgroup analysis is that two-thirds of the patients in the anticoagulation-free group (66.7%, 12/18) successfully completed their entire ECMO course (mean duration: 187.6 ± 82.8 h) without a single dose of systemic anticoagulation. Importantly, the rate of circuit exchange—a direct indicator of significant circuit thrombosis—was not higher in these patients (16.7%, 2/12) compared to those who received standard anticoagulation (24.0%, 6/25; p = 1.000). No statistically significant differences were observed between this subgroup and the anticoagulated group regarding survival to discharge (50.0% vs 76.0%, p = 0.146) and weaning success (58.3% vs 84.0%, p = 0.116). These results provide significant evidence that, with meticulous technical management and close monitoring, the traditional 48-h withholding window can be extended to the entire duration of ECMO support in selected high-risk trauma patients. This highlights that a completely anticoagulation-free strategy is not merely a temporary stabilizing measure but a sustainable management option, especially when the physiological state of trauma-induced coagulopathy may naturally mitigate the risk of circuit-related thrombosis.
Following the validation of our hypothesis, we explored specific clinical indicators that characterized patients managed without anticoagulation. These patients frequently presented with prolonged PTs, reduced fibrinogen levels, and higher trauma severity (lower GCS and TRISS scores) prior to ECMO initiation. They were also more likely to have undergone pre-ECMO interventional procedures for bleeding control. Notably, while trauma-specific indicators like GCS (p = 0.024) and TRISS (p = 0.031) showed significant differences between groups, the RESP score—a widely used survival prediction model for medical ARDS—did not (p = 0.099). This discrepancy reinforces the premise that TR-ARDS is pathophysiologically distinct from medical ARDS. Unlike medical cases driven by systemic inflammation, TR-ARDS is characterized by direct mechanical insults and trauma-induced coagulopathy (TIC). Therefore, traditional models like the RESP score are inadequate for this population as they fail to account for acute hemorrhage risk or anatomical injury severity, suggesting that trauma-specific coagulation status and injury mechanisms should take precedence in clinical decision-making.
While this study is limited by its retrospective design and small sample size, it underscores the necessity of a flexible, individualized approach to anticoagulation in severely injured patients. The clinical cues identified here offer a preliminary framework for future prospective trials. Ultimately, these findings contribute to the development of much-needed, evidence-based anticoagulation protocols for the complex TR-ARDS population, where standardized medical approaches often prove inadequate.
In this study, we demonstrated that withholding anticoagulation for at least the initial 72 h in TR-ARDS patients with active bleeding is a feasible and safe strategy, showing no significant deterioration in clinical outcomes such as survival or complications. Notably, factors such as prolonged PT, low fibrinogen, and higher trauma severity (low GCS/TRISS) emerged as key clinical features in patients managed without anticoagulation, providing potential decision-making cues for clinicians. Although limited by its retrospective nature, these findings highlight the need for flexibility in anticoagulation management for high-risk trauma patients, warranting further validation through larger prospective trials.
Footnotes
Acknowledgements
This work was supported by a clinical research grant from Pusan National University Hospital.
Ethical considerations
This study was approved by the Institutional Review Board of Pusan National University Hospital (IRB No. 2310-037-132), and the need for informed consent was waived owing to the study’s retrospective design.
Author contributions
Conceptualization: SHK, SS; Data curation: SHK, HCS, NHL, SL; Formal analysis: HCS; Methodology: HCS; Writing-original draft: HCS, Writing-review: SHK, HCS; feedback & editing: all authors. All authors have read and agreed to the published version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.