
Abstract
Background
Postcardiotomy cardiogenic shock (PCS) is a life-threatening complication after adult cardiac surgery that frequently necessitates venoarterial extracorporeal membrane oxygenation (VA-ECMO). Central and peripheral VA-ECMO cannulation strategies generate distinct hemodynamic and perfusion profiles; however, whether these differences translate into varying risks of acute brain injury (ABI) remains uncertain. We therefore compared ABI risk according to cannulation strategy in adults with PCS requiring VA-ECMO, with secondary objectives to determine the overall prevalence of ABI and characterize its major subtypes.
Methods
We systematically searched PubMed, Embase, Cochrane Library, Web of Science, and Scopus through April 15, 2025, for studies reporting ABI in adult PCS patients receiving VA-ECMO. ABI outcome was defined as ischemic stroke, intracranial hemorrhage, hypoxic-ischemic brain injury, seizures, unspecified stroke, and brain death. Random-effects meta-analysis was performed, incorporating a contemporary single-center cohort from Johns Hopkins Hospital (2020–2025).
Results
The primary meta-analysis included seven cohorts (six published studies plus Johns Hopkins cohort; n = 2536), while secondary analyses included 17 cohorts (16 published studies plus Johns Hopkins cohort). Included patients (mean age = 65 years, BMI = 28 kg/m2, 61% male) underwent central VA-ECMO cannulation in 32% and peripheral cannulation in 68%. The pooled risk of ABI did not differ by cannulation strategy (risk ratio [RR], 1.01; 95% CI, 0.85–1.21; I2 = 0%), with similar ABI prevalence across groups (p = 0.99). Ischemic stroke and unspecified stroke were the most reported subtypes.
Conclusion
In adults with PCS supported by VA-ECMO, the risk of ABI was not significantly associated with cannulation strategy. These findings suggest that cannulation approach alone is unlikely to be the primary determinant of neurological risk in this population, underscoring the need for systematic neuroprotective strategies regardless of cannulation configuration.
Keywords
Introduction
Postcardiotomy cardiogenic shock (PCS) is a life-threatening complication after adult cardiac surgery, characterized by inadequate cardiac output despite maximal medical therapy following cardiac surgery.1,2 The incidence of refractory PCS requiring advanced mechanical circulatory support ranges from 0.5% to 1.5%. 3 For such patients, venoarterial extracorporeal membrane oxygenation (VA-ECMO) serves as a critical bridge to myocardial recovery, durable mechanical support, or transplantation. PCS has become one of the most common indications for VA-ECMO support. 4 Mortality among PCS patients receiving VA-ECMO remains high, with acute brain injury (ABI)—ischemic stroke, intracranial hemorrhage (ICH), and hypoxic-ischemic brain injury (HIBI)—representing a major contributor to poor outcomes and a leading cause of death in this population.2,5,6
In the PCS population, reported ABI incidence ranges from 10% to 30%, with variable definitions of ABI and diagnostic techniques between studies.7,8 Importantly, ABI is strongly associated with increased mortality—89% in patients with ABI compared with 57% without (p < 0.001). 9 Despite the clinical significance of ABI in this population, comparative data evaluating how different ECMO configurations affect ABI risk remain limited. VA-ECMO cannulation can be performed centrally or peripherally, each with distinct hemodynamic implications for cerebral perfusion. 10 Central cannulation, performed through sternotomy with right atrial inflow and ascending aortic outflow, provides antegrade aortic flow and potentially superior upper body perfusion. 11 Peripheral cannulation involves femoral venous inflow and femoral or axillary arterial outflow. 11 While less invasive, femoral arterial cannulation produces retrograde aortic flow and risks differential hypoxia (Harlequin syndrome), whereas axillary or subclavian arterial cannulation generates antegrade flow similar to central cannulation. These physiological differences suggest that cannulation strategy could influence the risk of ABI10,11; however, this relationship has not been systematically examined in PCS patients.
Some studies suggest that central cannulation may be associated with higher mortality, greater bleeding requiring reoperation, and increased transfusion requirements, whereas peripheral cannulation carries a higher risk of limb ischemia7,8,12; however, whether these procedural differences translate into differential risk of ABI remains unclear. Notably, our prior single-center analysis (2017–2020) suggested numerically higher ischemic stroke rates with central cannulation, though overall ABI did not differ significantly. 13 Whether such patterns persist across larger populations remains unclear. Prior meta-analyses have examined overall complications between cannulation strategies but have either pooled PCS with non-postcardiotomy indications or focused on composite endpoints rather than ABI specifically.8,12
Therefore, we sought to systematically evaluate the association between cannulation strategy (central vs peripheral) and the risk of ABI in adults with PCS supported with VA-ECMO. Secondary objectives were to determine the overall prevalence of ABI and to characterize the distribution of ABI subtypes in this population.
Methods
This systematic review adheres to the 2020 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines in Supplemental Table 1. The protocol was prospectively registered with the International Prospective Register of Systematic Reviews (PROSPERO; CRD420251007318). The single-center cohort dataset was reviewed and approved by Johns Hopkins Medicine Institutional Review Board (IRB00216321), with a waiver of consent.
Search strategy
A comprehensive literature search was conducted across five electronic databases (PubMed, Embase, Cochrane Library, Web of Science, and Scopus) from inception through April 15, 2025. The search strategy combined controlled vocabulary, such as Medical Subject Headings (MeSH) and Emtree terms when appropriate, with free-text keywords relevant to VA-ECMO, PCS, and humans. The full search strategies for each database are available in Supplemental Table 2. References to the included articles were also manually screened to identify additional eligible studies. All records retrieved were independently reviewed by our team for eligibility using Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia). Any conflicts were resolved by consensus or by consultation with a third reviewer. Articles that met the inclusion criteria were obtained and reviewed.
Inclusion and exclusion criteria
We included studies that reported the prevalence of ABI outcomes in adult patients (≥18 years) undergoing VA-ECMO for PCS, stratified by cannulation type as central versus peripheral. Eligible studies were required to provide the number of ABI patients and baseline characteristics stratified by both cannulation types. Exclusion criteria included pediatric or adolescent patients younger than 18 years and studies restricted to venovenous ECMO (VV-ECMO). Abstracts without corresponding full texts such as conference proceedings, animal studies, case reports, case series with fewer than 20 patients, commentaries, editorials, systematic reviews and meta-analyses, narrative reviews, and articles published in languages other than English were also excluded.
In addition to the published literature, we incorporated a single-center retrospective observational cohort from The Johns Hopkins Hospital (April 1, 2020, and August 31, 2025), which did not overlap with previously published Johns Hopkins cohorts. This cohort was included to provide contemporary patient-level data and to externally validate the comparative findings observed in the study-level meta-analysis. Adult patients (≥18 years) with PCS who required VA-ECMO were identified. Patients receiving non-VA ECMO configurations (e.g., venovenous or veno-veno-arterial ECMO), as well as those who underwent conversion between ECMO modalities, were excluded to ensure a homogeneous cohort managed exclusively with VA-ECMO.
A total of 115 patients met inclusion criteria. Cannulation strategy was classified as central or peripheral. Relevant baseline, procedural, and postoperative variables, along with ABI outcomes confirmed by neuroimaging (CT and/or MRI), were abstracted from the electronic medical record.
Study selection and data extraction
Titles and abstracts were screened in Covidence using a two-reviewer independent screening model. Seven investigators (J.R., A.H., H.Y.W., P.S., J.L., M.C., and A.M.) participated in the screening process, with each record assessed independently by two reviewers. Disagreements were resolved by a third reviewer (Y.L.). Full-text eligibility was independently evaluated by two reviewers (J.R. and Y.L.), and discrepancies were resolved by consensus. Data extraction was performed by seven investigators (J.R., Y.L., A.H., P.S., J.L., M.C., and A.M.), with each included study independently extracted by two of the seven reviewers. Discrepancies were resolved by consensus. Data were extracted into an Excel spreadsheet (Microsoft Corp., Redmond, WA). The study selection process is summarized in the PRISMA flow diagram in Figure 1. PRISMA flow diagram of study selection for meta-analysis. The flow diagram summarizes the identification, screening, eligibility assessment, and inclusion of studies evaluating acute brain injury (ABI) in adult patients receiving venoarterial extracorporeal membrane oxygenation (VA-ECMO) for postcardiotomy shock. Of 18,615 records identified through database searches, 16 studies met criteria for qualitative synthesis by reporting ABI outcomes stratified by cannulation type. Among these, 6 studies provided baseline characteristics stratified by cannulation strategy and included both central and peripheral cannulation cohorts and were therefore eligible for cannulation-stratified meta-analyses. The Johns Hopkins single-center cohort (2020–2025) was additionally included, resulting in a total of 7 studies and 2536 patients in the primary analysis.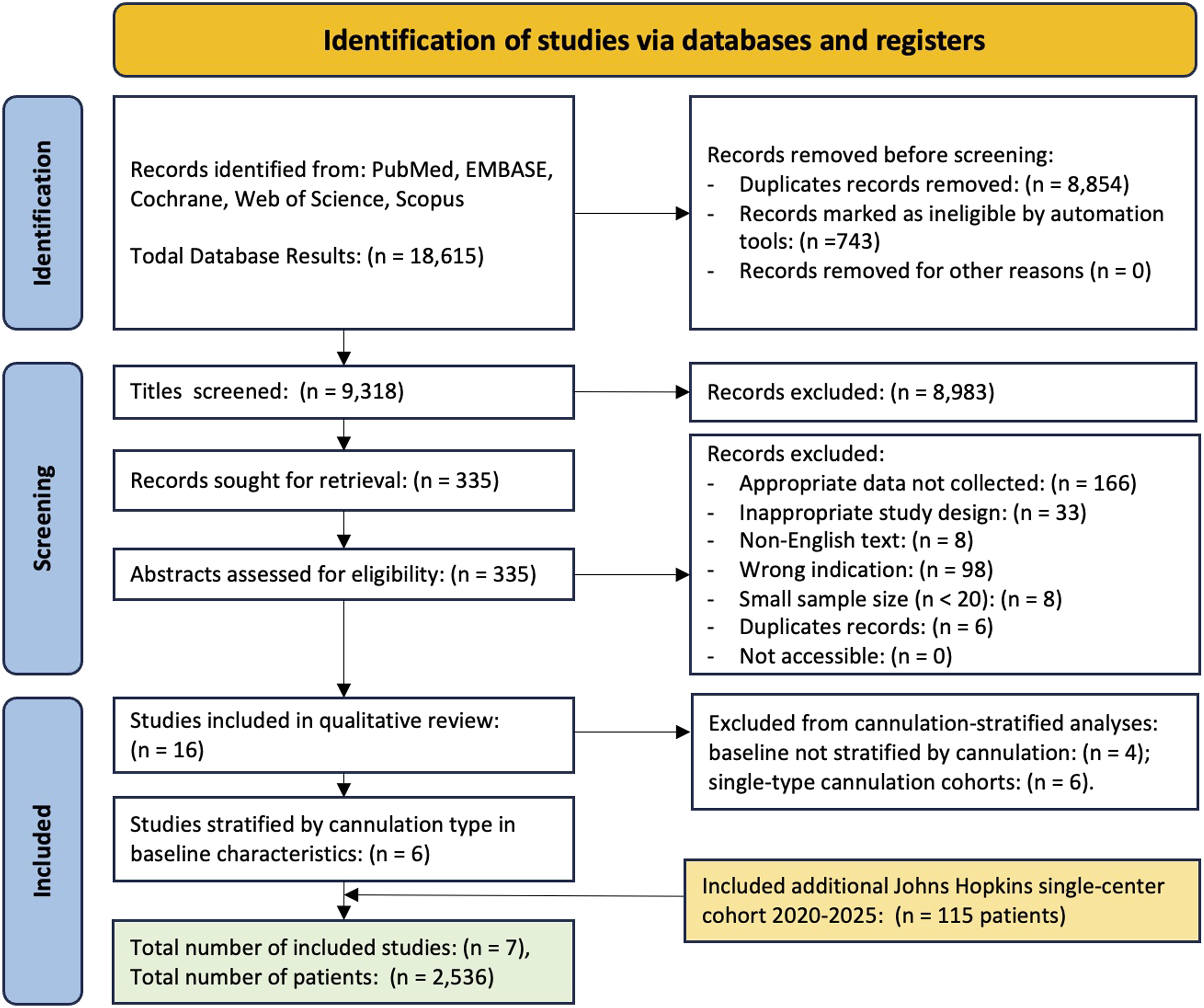
Baseline characteristics extracted included demographics [age, sex, body mass index (BMI)], past medical history [hypertension, diabetes mellitus, atrial fibrillation, chronic kidney disease, peripheral artery disease, pulmonary disease, prior stroke, prior myocardial infarction, smoking history]. Clinical variables included the type of cardiac surgery performed (Supplemental Table 3), pre-ECMO variables [EuroSCORE II, left ventricular ejection fraction (LVEF), preoperative intra-aortic balloon pump (IABP), previous cardiac surgery, prior cardiac arrest, cardiopulmonary bypass (CPB) time, emergency operation], and on-ECMO variables [ECMO duration, IABP use during ECMO]. Clinical outcomes, including mortality and ABI, were also collected.
Definitions and outcomes
The primary outcome was the comparative risk of ABI among adult patients receiving VA-ECMO for PCS, stratified by cannulation strategy. Central VA-ECMO was defined as cannulation of the right atrium for venous drainage and the ascending aorta for arterial return, established intraoperatively through open sternotomy. Peripheral VA-ECMO was defined as venous drainage via the femoral or internal jugular vein with arterial return through a peripheral artery, the most commonly the femoral artery, established either surgically or percutaneously; axillary and subclavian arterial cannulation were also classified as peripheral.
ABI was defined according to study-specific criteria and included only events occurring during ECMO support. For secondary analyses, ABI was categorized into predefined subtypes: (1) ischemic stroke, (2) ICH, (3) HIBI, (4) seizures, (5) unspecified stroke, and (6) brain death. Given the heterogeneity in terminology across included studies, we standardized the definitions a priori. The specific ABI terminologies in each paper are provided in Supplemental Table 4. Neurological complications described as cerebral infarction were classified as ischemic stroke, and those reported as hemorrhagic stroke were classified as ICH. Although ischemic stroke is a recognized subtype of ABI, several studies reported neurological events more generally as “stroke”, “major cerebrovascular accident (CVA)”, or “cerebrovascular insult” without specifying ischemic or hemorrhagic etiology. Such cases were categorized as unspecified stroke unless underlying pathology was clearly defined. HIBI encompassed terms including hypoxic encephalopathy, 10 hypoxic-ischemic brain injury, 11 brain edema, 14 global cerebral ischemia, 15 and anoxic encephalopathy. 16
For the composite ABI outcome, each patient was counted once per cohort. However, for subtype analyses, patients could contribute to more than one ABI subtype category if multiple neurologic injuries were reported. For example, cases reported as “CVA and seizures” were included in both the unspecified stroke and seizure subtype categories. 17
Risk of bias assessments
Two investigators (J.R. and Y.L.) independently assessed the risk of bias for each included study using the Newcastle–Ottawa Scale (NOS), 18 with results summarized in Supplemental Table 5. The NOS evaluates study quality across three domains: selection, comparability, and outcome. Studies were classified as high quality (7–9 points), moderate quality (4–6 points), or low quality (0–3 points). For seven included cohorts, sensitivity analyses were performed by restricting the synthesis to studies rated as high quality (NOS score ≥7). In addition, leave-one-out analyses were conducted to evaluate the influence of individual studies on the pooled effect estimates. Discrepancies between reviewers were resolved through consensus.
The certainty of evidence was assessed using the GRADE framework in Supplemental Table 6. Risk of bias was evaluated based on the NOS. Inconsistency was assessed using statistical heterogeneity (I2). Indirectness was evaluated based on the similarity of population, exposure, and outcomes. Imprecision was assessed based on the width of confidence intervals and whether they crossed the line of no effect. Assessment of publication bias using funnel plots was not performed for the primary meta-analysis due to the limited number of included studies (n = 7), in accordance with Cochrane guidance.
Statistical analysis
The statistical analysis was conducted in accordance with established methods for meta-analysis of observational data. Categorical variables were summarized as counts and percentages. When available, continuous variables describing patient demographics and clinical characteristics were summarized as weighted means with standard deviations (SDs).
The primary analysis compared the risk of composite ABI between central and peripheral cannulation using pooled risk ratios (RRs) with 95% confidence intervals (CIs). Only studies reporting cannulation-stratified composite ABI outcomes and baseline characteristics were eligible for this comparison. Six published studies met this criterion and were combined with the Johns Hopkins single-center cohort, yielding a total of seven cohorts for the primary comparative analysis. Random-effects models were applied to account for between-study variability. Statistical heterogeneity was quantified using the I2 statistic and Cochran’s Q test.
For descriptive purposes, pooled prevalence of composite ABI was estimated using random-effects models with logit transformation. All published studies reporting ABI prevalence were included (n = 16), together with the Johns Hopkins cohort (total n = 17). Prevalence was calculated within each study as the number of patients with ABI divided by the total number of patients in the corresponding cannulation group.
Analyses of ABI subtypes were conducted as pooled prevalence analyses and were restricted to studies reporting subtype-specific outcomes (central cannulation: n = 7; peripheral cannulation: n = 13). Studies were eligible if cannulation-specific subtype counts could be extracted. The number of included studies is explicitly reported in the corresponding figure or table caption for each analysis.
In the Johns Hopkins single-center cohort, multivariable logistic regression was performed to evaluate the independent association between cannulation strategy and ABI, adjusting a priori for pre-ECMO cardiac arrest and CPB time.9,19–21 Given the limited number of ABI events (n = 22), the number of covariates included in the multivariable model was constrained to avoid overfitting. Although other clinically relevant variables were considered, pre-ECMO cardiac arrest and CPB time were prioritized as a priori clinical confounders based on their established associations with neurological injury during ECMO support.
All statistical analyses were conducted using R version 4.5.2 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Study selection
The literature search identified 18,615 records across all databases. After removing duplicates and ineligible records, 9318 titles were screened, yielding 335 articles that were assessed for full-text review. Seven cohorts (six published studies plus Johns Hopkins cohort; n = 2536) met the inclusion criteria for the primary meta-analysis, which reported both baseline characteristics and ABI stratified by cannulation strategy (Figure 1).
In a descriptive analysis of ABI prevalence, 17 cohorts were included, comprising 16 published studies and the Johns Hopkins single-center cohort, which reported ABI stratified by cannulation strategy. These studies were included in the pooled prevalence analyses. Characteristics of the published studies were presented in Supplemental Table 4.1,4,6,10,11,13–17,22–27 Risk of bias for the 16 published studies was assessed using the NOS. All studies were rated as high quality, with five studies receiving a score of 7, two receiving a score of 8, and nine achieving a score of 9 (Supplemental Table 5).
Baseline characteristics of the pooled PCS VA-ECMO cohort
Baseline characteristics of included studies stratified by cannulation strategy (n = 7).
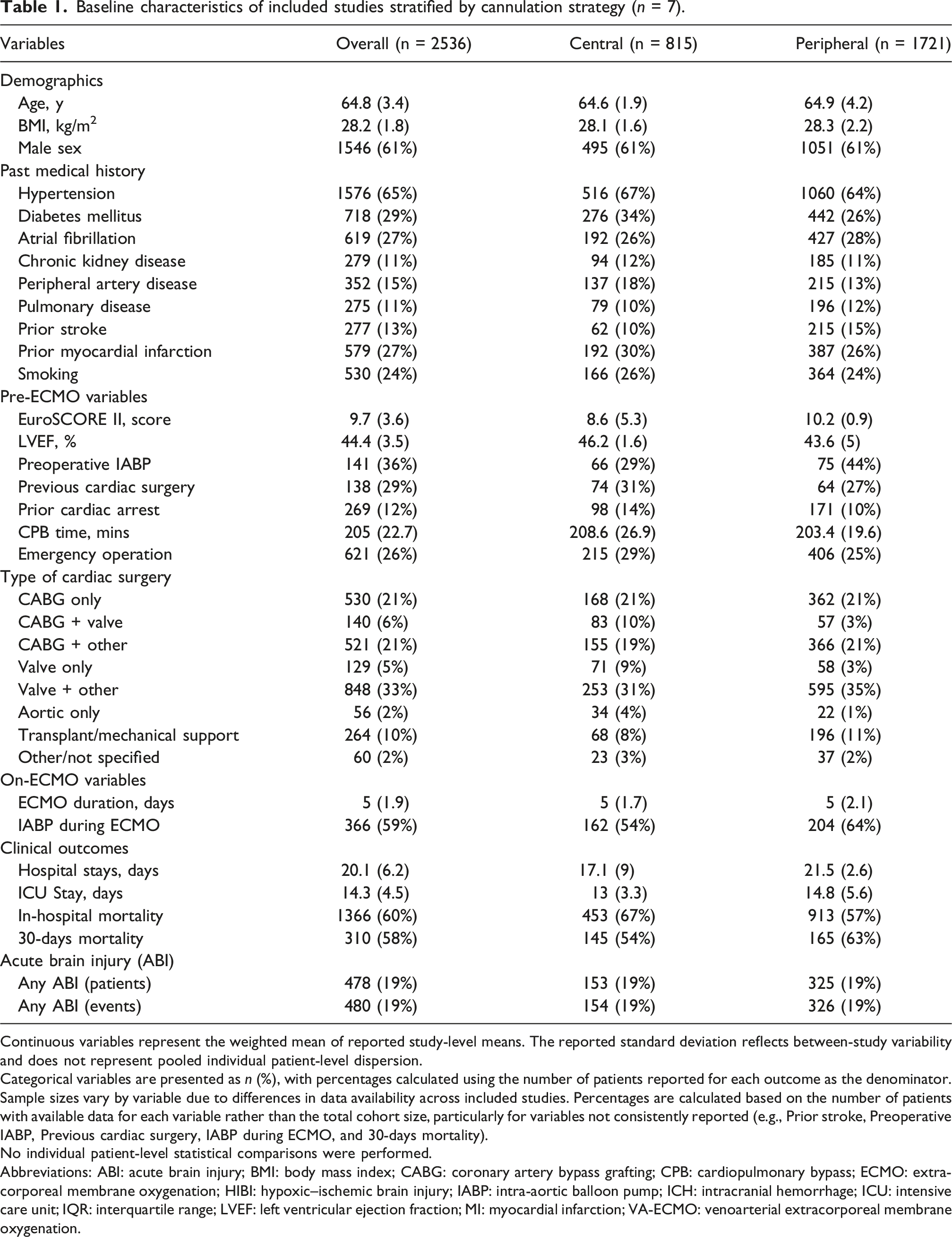
Continuous variables represent the weighted mean of reported study-level means. The reported standard deviation reflects between-study variability and does not represent pooled individual patient-level dispersion.
Categorical variables are presented as n (%), with percentages calculated using the number of patients reported for each outcome as the denominator.
Sample sizes vary by variable due to differences in data availability across included studies. Percentages are calculated based on the number of patients with available data for each variable rather than the total cohort size, particularly for variables not consistently reported (e.g., Prior stroke, Preoperative IABP, Previous cardiac surgery, IABP during ECMO, and 30-days mortality).
No individual patient-level statistical comparisons were performed.
Abbreviations: ABI: acute brain injury; BMI: body mass index; CABG: coronary artery bypass grafting; CPB: cardiopulmonary bypass; ECMO: extracorporeal membrane oxygenation; HIBI: hypoxic–ischemic brain injury; IABP: intra-aortic balloon pump; ICH: intracranial hemorrhage; ICU: intensive care unit; IQR: interquartile range; LVEF: left ventricular ejection fraction; MI: myocardial infarction; VA-ECMO: venoarterial extracorporeal membrane oxygenation.
When stratified by cannulation strategy, patients receiving central VA-ECMO had a higher prevalence of diabetes mellitus (34% vs 26%), peripheral artery disease (18% vs 13%), prior myocardial infarction (30% vs 26%), and prior cardiac arrest (14% vs 10%). In contrast, peripheral VA-ECMO patients had higher EuroSCORE II (10.2 vs 8.6), more frequent preoperative IABP use (44% vs 29%), and a greater prevalence of prior stroke (15% vs 10%). Regarding clinical outcomes, in-hospital mortality was higher in the central group (67% vs 57%), whereas 30-days mortality was higher in the peripheral group (63% vs 54%).
Johns Hopkins single-center cohort
Among 115 patients in the Johns Hopkins single-center cohort, 60 (52%) underwent central cannulation and 55 (48%) underwent peripheral cannulation. The central group had a higher proportion of males (72% vs 49%, p = 0.021) and shorter CPB times (177 vs 226 min, p = 0.024) (Supplemental Table 7). ABI occurred in 22 patients (19%) overall and was more frequent in the central cannulation group than in the peripheral group (25% vs 13%, p = 0.104). Ischemic stroke was more common with central cannulation (18.3% vs 5.5%, p = 0.046), while rates of ICH, seizure, and HIBI were similar between groups. With respect to clinical outcomes, patients in the peripheral cannulation group had longer ICU lengths of stay compared with those in the central cannulation group (25 vs 13 days, p = 0.008). In multivariable logistic regression analysis adjusting for pre-ECMO cardiac arrest and CPB time, central cannulation was associated with higher odds of composite ABI (aOR, 2.31; 95% CI, 0.86–6.72), though this did not reach statistical significance (p = 0.107), likely reflecting the limited number of ABI events in this cohort (Supplemental Figure 1).
Overall prevalence of ABI
Of the 2536 PCS VA-ECMO patients, 478 (19%) had at least one type of ABI (Table 1). There was similar prevalence of ABI between patients undergoing central cannulation versus peripheral cannulation (19% vs 19%). In a descriptive analysis of 17 studies (16 studies included in qualitative review plus the single-center cohort), the pooled prevalence of overall ABI was 19% (95% CI, 17%–21%) (Supplemental Figure 2). When stratified by cannulation type, the pooled prevalence was similar between central cannulation (20%; 95% CI, 14%–26%) and peripheral cannulation (18%; 95% CI, 16%–21%) (Supplemental Figure 3). Across both cannulation strategies, ischemic stroke and unspecified stroke were the most frequently reported ABI subtypes, whereas ICH, HIBI, seizures, and brain death occurred less commonly (Supplemental Figures 4 and 5). Subtype-specific pooled prevalence estimates for ischemic stroke, ICH, HIBI, seizures, and unspecified stroke did not differ significantly between central and peripheral cannulation groups (Supplemental Figure 6).
Risk of ABI: Central versus peripheral cannulation
In the primary pooled meta-analysis of seven studies (six published studies and the Johns Hopkins single-center cohort), cannulation strategy was not associated with a significant difference in ABI risk (RR, 1.01; 95% CI, 0.85–1.21; I2 = 0.0%) (Figure 2). This finding was consistent across multiple sensitivity analyses. Leave-one-out analyses demonstrated the robustness of the primary outcome, with pooled RRs ranging from 0.94 to 1.05, indicating no undue influence of any single study, including the largest study (Supplemental Table 8). Furthermore, exclusion of studies with limited baseline characteristics yielded an identical pooled estimate (RR, 1.01) (Supplemental Figure 7).4,17 Risk ratio of acute brain injury comparing central versus peripheral VA-ECMO cannulation. Forest plot showing study-specific and pooled risk ratios (RRs) for acute brain injury (ABI) in adult patients receiving VA-ECMO for postcardiotomy shock, comparing central with peripheral cannulation strategies. A random-effects model was used to estimate pooled RRs with 95% confidence intervals. The Johns Hopkins single-center cohort (2020–2025) is included as an individual study. Between-study heterogeneity was assessed using the I2 statistic. Abbreviations: ABI: acute brain injury; CI: confidence interval; RR: risk ratio; VA-ECMO: venoarterial extracorporeal membrane oxygenation.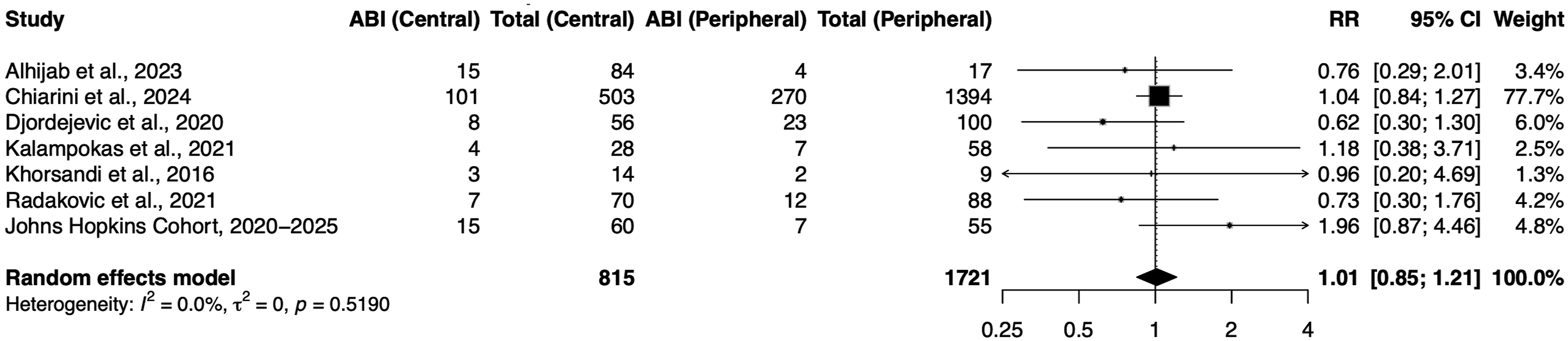
In an exploratory sensitivity analysis, we additionally included four studies that reported cannulation-stratified ABI patient number but lacked detailed baseline stratification. When these studies were combined with the primary seven studies (total n = 11), the pooled analysis similarly demonstrated no significant difference in ABI risk between central and peripheral cannulation strategies (RR, 1.08; 95% CI, 0.93–1.26) (Supplemental Figure 8).
Discussion
In this systematic review and meta-analysis incorporating a contemporary single-center cohort, we found no significant difference in ABI risk between central and peripheral VA-ECMO cannulation strategies in patients with PCS. The pooled estimate demonstrated no statistical heterogeneity across studies (I 2 = 0%), indicating highly consistent effect estimates, and multiple sensitivity analyses produced similar results, supporting the robustness and stability of the findings. These results indicate that cannulation configuration alone is unlikely to be the major determinant of ABI in this population, despite theoretical physiologic differences in flow patterns, cerebral perfusion, and embolic risk between the two approaches.
The mechanism of ABI in PCS is likely multifactorial and often begins prior to ECMO cannulation. Patients with PCS are exposed to numerous high-risk conditions, including profound hemodynamic instability, systemic inflammation, coagulopathy, and embolic burden related to CPB.3,7 These competing drivers of ABI may overshadow the risks of the different hemodynamic and technical differences between central versus peripheral strategies. Central cannulation is typically employed intraoperatively for patients who fail to wean from CPB.7,28 These patients often have greater illness severity and have been shown to experience higher rates of bleeding complications, require more blood transfusions, and undergo more frequent re-operations compared with peripherally cannulated patients.28,29 In contrast, peripheral cannulation, specifically femoral vein and artery cannulation, generates retrograde flow and may predispose to complications such as inadequate venous drainage, left ventricular distension requiring unloading strategies, ventricular stasis with thrombus formation, and differential hypoxia.7,28 Despite higher illness severity and increased in-hospital mortality among patients undergoing central cannulation,8,28 the frequency of ABI was similar between strategies, suggesting that neurologic injury in PCS may be driven more by the underlying postcardiotomy physiology than by cannulation configuration alone. Although ABI frequency was similar, mortality differed between cannulation strategies. Patients who received peripheral cannulation had increased 30-days mortality (63% vs 54%), while centrally cannulated patients had higher in-hospital mortality (67% vs 57%). This temporal discordance suggests that the drivers of mortality operated on different timelines. The higher 30-days mortality in the peripheral cannulation group likely reflects a higher risk patient population in this cohort, with greater EuroSCORE II scores and more reliance on IABP support both pre- and post-ECMO. While not reported in this study, peripheral cannulation is more frequently associated with vascular site infections and sepsis which may contribute to early mortality. 28 Conversely, central cannulation was associated with a higher overall in-hospital mortality. This finding is similar to other studies which demonstrated higher mortality after central cannulation, largely driven by bleeding related complications and re-operations. 28 These bleeding-driven complications manifest as cumulative morbidity over the course of the hospital stay, which may inflate in-hospital mortality relative to 30-days mortality in centrally cannulated patients.
We previously reported a single-center prospective cohort of patients with PCS treated with VA-ECMO between 2017 and 2020. In that cohort, patients receiving central cannulation experienced a higher frequency of ischemic stroke and ICH compared with peripheral cannulation, although the overall prevalence of ABI was not statistically different between cannulation strategies. 13 Our updated institutional cohort (2020–2025) showed a similar pattern, with numerically higher ABI in centrally cannulated patients but no statistically significant difference between strategies, while ischemic stroke remained more frequent in the central group. The rationale for higher frequency of ischemic stroke in the Johns Hopkins central group may reflect differences in illness severity, as central cannulation historically represents a substantially sicker population with greater physiologic instability. This specific finding may stem from technical challenges or intraoperative failures, such as inability to wean from CPB, that are not directly measured. These higher-acuity clinical scenarios may independently increase neurologic risk but are difficult to fully capture in retrospective analyses. At the same time, the Johns Hopkins peripheral cohort demonstrated longer CPB times, and most of these patients underwent transplant or mechanical circulatory support procedures, highlighting the heterogeneity and overlap in illness severity between groups. As such, differences in patient selection, operative indication, and perioperative complexity may have confounded the apparent association between cannulation strategy and neurologic injury.
Although single-center studies allow for more detailed neurologic characterization and improved detection of severe neurologic complications, they may also be influenced by center-specific practice patterns, era differences, and case-mix variation, including preferential use of central cannulation in the most critically ill patients. These factors may account for the discordance between the Johns Hopkins cohort and the pooled meta-analysis ABI risk. The institutional cohort contributed only a small proportion of the overall meta-analytic weight, whereas the pooled estimate was largely driven by larger multicenter data. Consequently, while the pooled analysis suggests no overall difference in ABI risk between central versus peripheral cannulation strategies, it remains possible that specific high-acuity subgroups undergoing central cannulation may carry elevated ABI risk that becomes diluted within aggregated analyses of heterogeneous ECMO populations.
To our knowledge, this study represents the first meta-analysis specifically examining composite ABI according to VA-ECMO cannulation strategy in PCS. Two prior meta-analyses by Mariscalco et al. and Raffa et al. reported no significant difference in neurologic events between cannulation strategies (RR, 0.79; 95% CI, 0.59–1.05; I 2 = 0%; and RR, 0.88; 95% CI 0.46–1.68; p = 0.69, respectively).8,28 However, Mariscalco et al. defined neurologic events broadly as focal or global neurologic deficits (e.g., stroke, hemiplegia, hemiparesis, numbness, sensory loss), whereas Raffa et al. relied on “cerebrovascular events.” Both studies did not systematically evaluate specific ABI subtypes. In addition, Raffa et al. included a heterogenous VA-ECMO population comprising both PCS and non-PCS cohorts. In contrast, our pooled multi-study analysis focused exclusively on PCS patients and evaluated composite ABI as a predefined primary outcome with systematic assessment of subtypes, including ICH, HIBI, seizures, unspecified stroke, and brain death. Despite methodological differences, prior findings are broadly consistent with our results, which demonstrate no significant difference in composite ABI risk between central and peripheral cannulation strategies.
The overall pooled ABI prevalence of 19% underscores the substantial neurologic risk among PCS patients supported by VA-ECMO. Ischemic stroke and unspecified stroke were the most frequently reported events, and pooled prevalence of ABI subtypes did not differ significantly between cannulation strategies. The similar distribution of ABI subtypes supports the concept that shared systemic mechanisms including pre-ECMO physiological/hemodynamic instability, embolic burden, systemic inflammation, anticoagulation-related bleeding risk, and periods of reduced cerebral perfusion, may play a more dominant role in ABI than cannulation-specific factors.7,30,31
These findings carry important clinical implications. Cannulation strategy should be guided primarily by operative context, technical feasibility, and overall patient condition rather than perceived differences in ABI risk. Neuroprotective efforts should instead focus on modifiable risk factors common to both configurations, including limiting low cerebral flow states, avoidance of abrupt PaCO2 and PaO2 shifts, judicious anticoagulation administration, mitigating embolic risk, and structured neurologic monitoring.7,13,30–32 Given the high baseline ABI prevalence, standardized neurologic surveillance protocols may be warranted for all PCS patients receiving VA-ECMO, irrespective of cannulation approach. 33
Limitations
There are several limitations to this study. First, this is a retrospective meta-analysis of observational studies which risks residual confounding related to institutional cannulation practices, variable management strategies, and patient severity of PCS. One study accounted for more than half of the patients (nearly 78% of the meta-analytic weight) in the entire meta-analysis cohort, creating a large risk for dominance bias. Thus, these findings should be interpreted with caution with recognition that this dominance bias limits the generalizability of our results. However, the use of leave-one-out analyses mitigates the variability in reporting of statistical significance. Second, neurological outcomes were heterogeneously defined and variable across studies, requiring post-hoc standardization which introduces risk of misclassification and under detection of specific neurological injury subtypes. Only a subset of studies reported cannulation-stratified ABI outcomes. Aggregate-level meta-analysis precludes adjustment for important patient specific variables, including anticoagulation use, hemodynamic changes, and ECMO parameters. Finally, inclusion of a single-center cohort bolsters the sample population, improves relevance but may limit generalizability to other ECMO institutions. These limitations highlight the need for prospective studies with standardized protocols for neurological assessment in patients with PCS treated with VA-ECMO. Additionally, data on institutional ECMO volume were not consistently reported across included studies, and we were therefore unable to evaluate its potential impact on ABI risk or assess center-level effects on neurologic outcomes. This limitation also precluded analysis of whether the proportion of central versus peripheral cannulation differed between low- and high-volume ECMO centers.
Conclusions
Among PCS patients supported with VA-ECMO, we did not observe a significant difference in composite ABI risk between central and peripheral cannulation strategies. These findings suggest that cannulation configuration alone is unlikely to be a primary determinant of neurological risk in this population. Clinically, cannulation strategy should be guided by operative feasibility and patient-specific factors rather than ABI risk, with neuroprotection and standardized neurologic surveillance prioritized across all VA-ECMO configurations.
Supplemental material
Supplemental Material - Acute brain injury in adult post-cardiotomy cardiogenic shock patients receiving central vs. peripheral VA-ECMO: A single-center experience and systematic review with meta-analysis
Supplemental Material for Acute brain injury in adult post-cardiotomy cardiogenic shock patients receiving central vs. peripheral VA-ECMO: A single-center experience and systematic review with meta-analysis by Juyeon Ryu, Yiting Lin, Hyun Yi (Jacqualine) Woo, Ahmad Hamid, Madison Malfitano, Parth Sutariya, Justin Lu, Melanie Crasta, Abdullah Mahmood, Yaman B. Ahmed, Marcus Spann, Glenn J. R. Whitman and Sung-Min Cho in Perfusion.
Supplemental material
Supplemental Material - Acute brain injury in adult post-cardiotomy cardiogenic shock patients receiving central vs. peripheral VA-ECMO: A single-center experience and systematic review with meta-analysis
Supplemental Material for Acute brain injury in adult post-cardiotomy cardiogenic shock patients receiving central vs. peripheral VA-ECMO: A single-center experience and systematic review with meta-analysis by Juyeon Ryu, Yiting Lin, Hyun Yi (Jacqualine) Woo, Ahmad Hamid, Madison Malfitano, Parth Sutariya, Justin Lu, Melanie Crasta, Abdullah Mahmood, Yaman B. Ahmed, Marcus Spann, Glenn J. R. Whitman and Sung-Min Cho in Perfusion.
Supplemental material
Supplemental Material - Acute brain injury in adult post-cardiotomy cardiogenic shock patients receiving central vs. peripheral VA-ECMO: A single-center experience and systematic review with meta-analysis
Supplemental Material for Acute brain injury in adult post-cardiotomy cardiogenic shock patients receiving central vs. peripheral VA-ECMO: A single-center experience and systematic review with meta-analysis by Juyeon Ryu, Yiting Lin, Hyun Yi (Jacqualine) Woo, Ahmad Hamid, Madison Malfitano, Parth Sutariya, Justin Lu, Melanie Crasta, Abdullah Mahmood, Yaman B. Ahmed, Marcus Spann, Glenn J. R. Whitman and Sung-Min Cho in Perfusion.
Footnotes
Author contributions
Conceptualization, S.-M.C.; methodology, J.R., Y.L., H.Y.W., A.H., Y.A., and M.S.; investigation, J.R., Y.L., H.Y.W., A.H., P.S., J.L., M.C., and A.M.; data curation, J.R., Y.L., A.H., P.S., J.L., M.C., and A.M.; formal analysis, J.R.; writing—original draft preparation, J.R., Y.L., H.Y.W., A.H., and M.M.; writing—review and editing, J.R. and Y.L.; supervision, S.-M.C. and G.W. All authors have read and agreed to the published version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Sung-Min Cho is supported by NIH (1K23HL157610, 1R21NS135045), DARPA (HR001124S0024), Hyperfine Inc. (SAFE MRI ECMO), NeurOptics (SEE ECMO study), StellarCube Inc. (CAPTURE PAIN study), and ASPEN Rhoads Research Foundation (EE-ECMO study).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data needed to evaluate the conclusions in the paper are present in the main manuscript and in the supplemental material.
Trial registration
Our study was registered on PROSPERO with registration number CRD420251007318.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.