
Abstract
A 68-year-old woman presented with palpitations, though ECG monitoring showed sinus rhythm. Multimodal imaging (cardiac magnetic resonance and echocardiography) showed asymmetric septal hypertrophy with left ventricular outflow tract obstruction (resting gradient of up to 87 mmHg). Echocardiography showed severe mitral regurgitation with multiple regurgitant jets and systolic anterior motion of the mitral valve. Mitral valve anatomy was abnormal, with anterior leaflet restriction and a clefted posterior leaflet. Symptoms persisted despite medical therapy (beta-blockers), and following multidisciplinary discussion, she proceeded to surgery on symptomatic and prognostic grounds. The patient underwent successful septal myectomy and bioprosthetic mitral valve replacement with excellent valve function. Following a generally uneventful postoperative recovery, she was discharged on postoperative day ten with stable cardiac function. This case highlights a rare trileaflet configuration of the mitral valve contributing to severe mitral regurgitation in hypertrophic obstructive cardiomyopathy and underscores the importance of detailed anatomical assessment in guiding surgical decision-making.
Keywords
Introduction
Hypertrophic cardiomyopathy (HCM) is the most common genetic cardiac condition, with hypertrophic obstructive cardiomyopathy (HOCM) representing approximately 60% of HCM cases. 1 HOCM is characterised by asymmetric septal hypertrophy and dynamic left ventricular outflow tract (LVOT) obstruction. The primary mechanism of LVOT obstruction reflects anatomical narrowing of the outflow tract combined with a reduced aortomitral angle and anterior displacement of the mitral and subvalvular apparatus. Multivariate geometric analyses have confirmed that aortomitral angle and mitral coaptation height are independent echocardiographic predictors of LVOTO,2,3 and the clinical relevance of this anatomical framework is further supported by the efficacy of transapical septal reduction therapies that target LVOT geometry directly.4,5 Mitral leaflet elongation, extensively characterised by Sherrid and colleagues, 6 is an important amplifying HCM phenotype confirmed at histopathology. 7 Systolic anterior motion (SAM) of the mitral valve commonly results in significant mitral regurgitation (MR), the severity of which generally correlates with the magnitude of the LVOT gradient. 8
While LVOT obstruction due to SAM is often the principal driver of symptoms, a subset of patients presents with additional mitral valve abnormalities necessitating more complex management strategies.
Congenital mitral valve anomalies are distinctly rare. Among these, a trileaflet mitral valve is an exceptionally uncommon congenital variant, with only around 10 published cases in the literature. 9 This configuration has been associated with early degenerative changes and severe MR, as well as being particularly associated with HOCM. 9 We report the case of a 68-year-old woman with HOCM, severe MR, and SAM, in whom preoperative transoesophageal echocardiography (TOE) revealed a trileaflet mitral valve.
Case report
A 68-year-old woman presented to her local hospital with self-resolving palpitations and progressive exertional dyspnoea and was subsequently referred to our centre for mitral valve surgery with septal myectomy. Her past medical history included well-controlled hypertension, mild asthma, and primary biliary cholangitis. ECG and Holter monitoring showed no significant arrhythmias. Echocardiography revealed left ventricular hypertrophy with asymmetrical septal thickness of 17 mm and a resting LVOT gradient of up to 87 mmHg, though systolic function was preserved (LVEF 66%). There was also severe MR with two regurgitant jets and severe left atrial dilatation (51.1 ml/m2). Cardiac MRI confirmed HCM with a septal-to-lateral wall ratio of 1.9:1 and elevated mass (96 g/m2). Despite maximally tolerated bisoprolol (10 mg daily), the patient remained NYHA Class III with chest tightness and fatigue on routine exertion.
Transoesophageal echocardiography was performed to further characterise the mitral valve and guide management planning. This identified a trileaflet mitral valve with a cleft in the posterior leaflet, anterior leaflet restriction, and multiple severe regurgitant jets. Three-dimensional TOE demonstrated a trifoil orifice morphology in diastole and an abnormal coaptation pattern in systole, consistent with three distinct leaflet components (Figure 2). MR was attributed to both intrinsic valvular disease and SAM, precluding alcohol septal ablation and mandating surgical referral.
Following median sternotomy, cardiopulmonary bypass was established with bicaval cannulation. Cold blood cardioplegia was given into the aortic root and directly down the coronary ostia for myocardial protection. Intraoperative inspection confirmed the preoperative findings: the anterior leaflet was fibrotic and tethered, and the posterior leaflet harboured a deep central cleft creating three distinct segments (Figure 1). Via an aortotomy, an extended septal myectomy was performed under direct vision, followed by excision of the native mitral leaflets and implantation of a 33-mm bioprosthesis (Mitris Resilia, Edwards Lifesciences). Post-bypass TOE confirmed no residual MR, resolution of the LVOT gradient, and preserved biventricular function. Cardiopulmonary bypass was weaned without difficulty, and the patient was transferred to the ICU in a stable condition. Direct intraoperative needle manometry of the LVOT gradient was not performed; echocardiographic assessment served as the primary modality for haemodynamic surveillance throughout. Intraoperative view of the mitral valve, showing the clefted posterior mitral valve leaflet.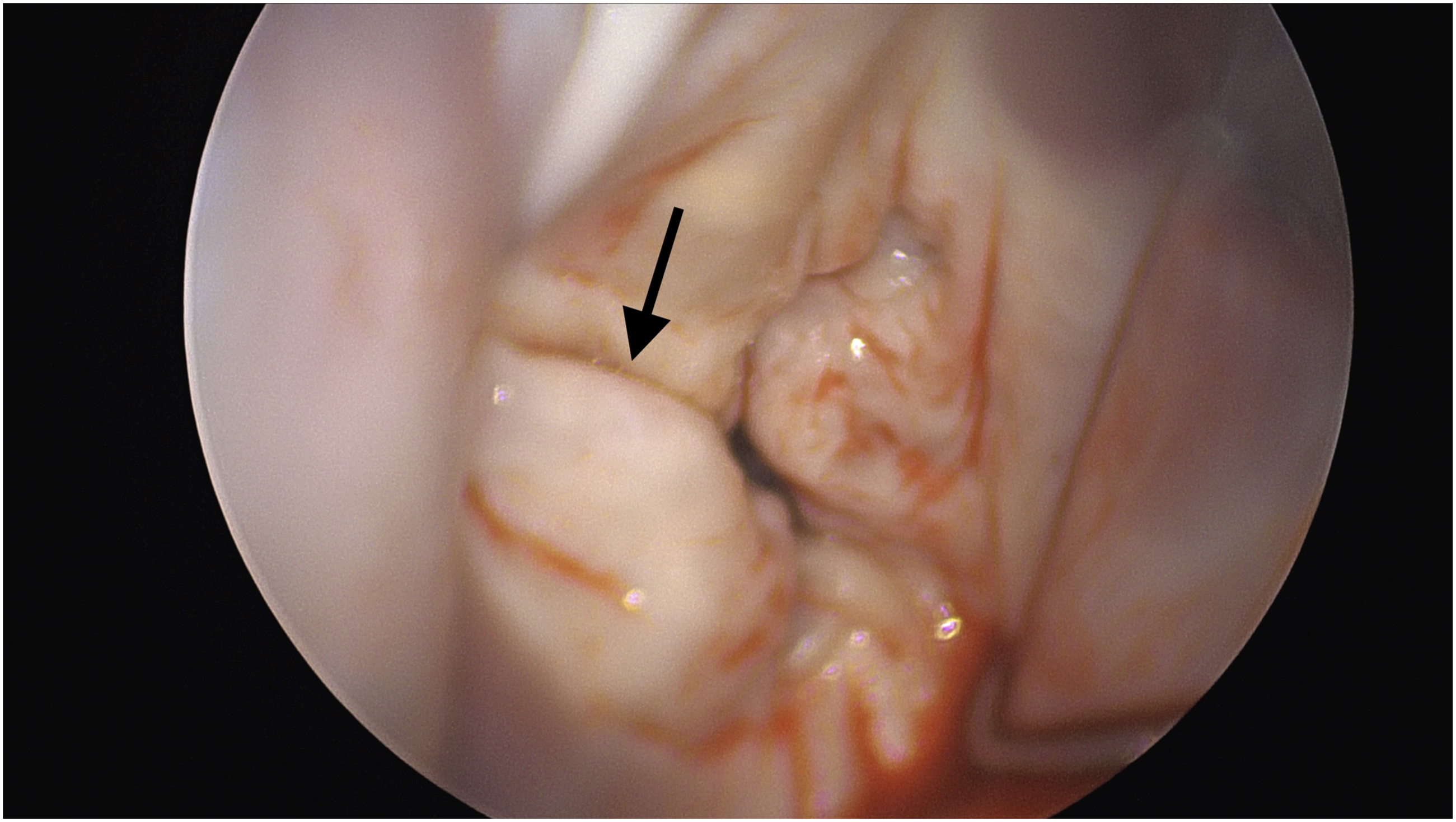
Following an uneventful 1-day ICU admission, she was transferred to the ward. She developed post-operative fast atrial fibrillation on postoperative day five, requiring cardioversion and oral amiodarone loading, but otherwise recovered well and was discharged home on postoperative day ten. At 6-month follow-up, she was recovering well, with improved exercise tolerance (>1h/day). Her breathing had significantly improved from her pre-operative state, and she denied any chest discomfort even upon moderate exertion. ECG confirmed sinus rhythm, with echocardiography showing no resting (gradient of 12mmHg) or provocable LVOT obstruction, and a well-seated mitral valve bioprosthesis with normal transvalvular gradients (mean peak gradient of 4mmHg).
Discussion
While HOCM is classically associated with SAM-related MR from secondary leaflet elongation, the co-existence of a congenital trileaflet mitral valve is exceedingly uncommon 9 and contributed in this case to a complex mechanism of MR and LVOT obstruction.
The bifid posterior leaflet, with its deep central cleft creating three discrete leaflets, produced abnormal coaptation and anterior displacement of the coaptation line, potentiating SAM and generating dual regurgitant jets. The aberrant leaflet morphology may have predisposed the patient to more severe MR than typically observed in standard HOCM pathology, underscoring the importance of meticulous valve assessment in such patients. Such complex valvular pathophysiology is readily missed on transthoracic echocardiography alone, underscoring the indispensable role of TOE in surgical planning, particularly three-dimensional TOE (Figure 2). Three-dimensional transoesophageal echocardiography of the mitral valve. (a) En-face view from the left atrial perspective in diastole, demonstrating a trifoil orifice morphology with a restricted anterior leaflet and clefted posterior leaflet creating distinct medial and lateral components, in contrast to the normal bileaflet ‘fish-mouth’ appearance. (b) Systolic frame demonstrating an abnormal coaptation pattern with a central zone of non-coaptation between the posterior leaflet segments, corresponding to the centrally directed regurgitant jet identified on colour doppler.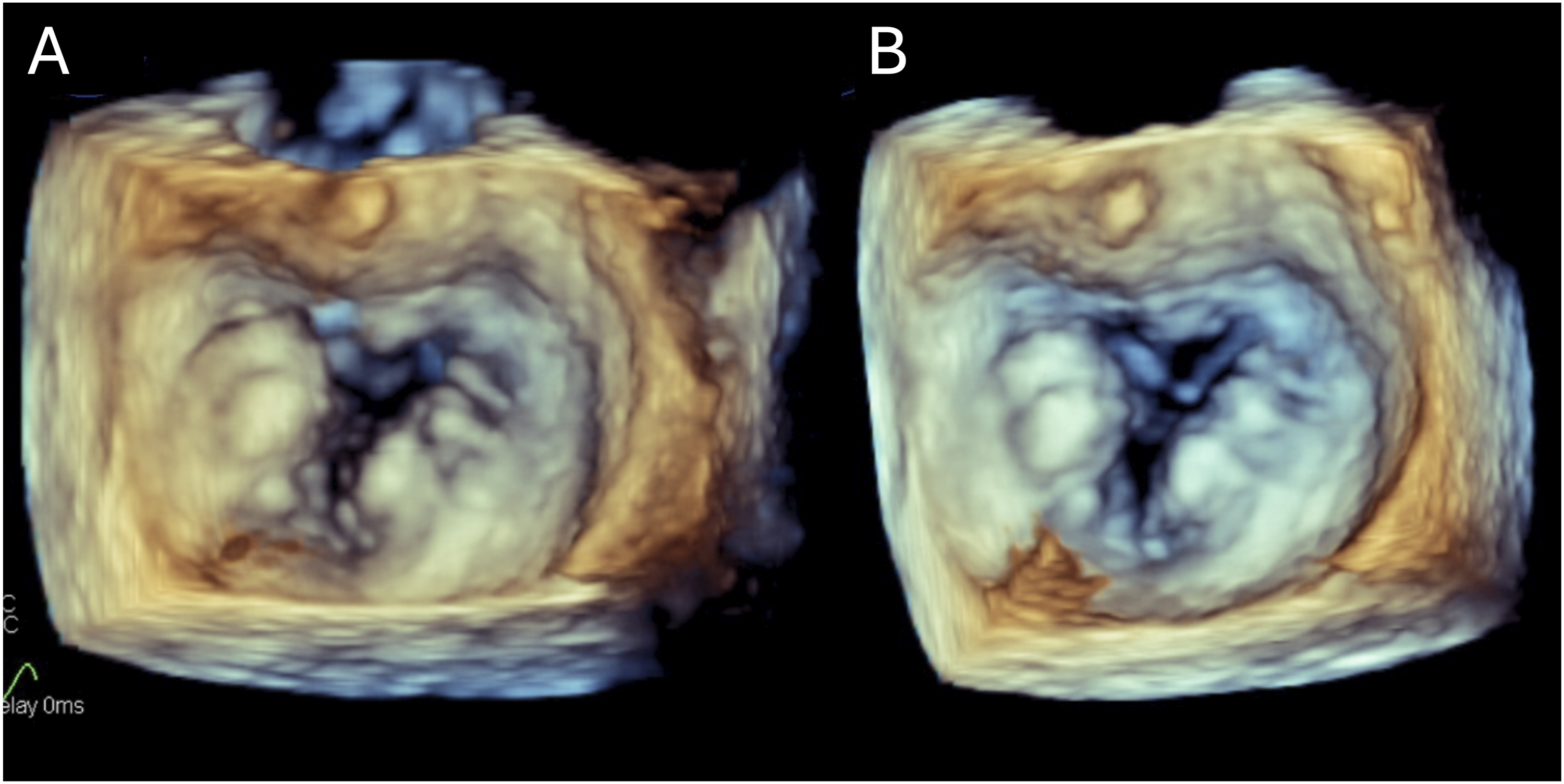
An important consideration in this case is the morphological distinction between a true trileaflet mitral valve and a bifid posterior leaflet with a deep central cleft. As highlighted in a systematic review of the trileaflet mitral valve literature, this entity remains definitionally controversial: it is debated whether reported cases represent a genuinely distinct third leaflet or improved visualisation of deep posterior leaflet clefts, given the lack of universally accepted morphological criteria. 10 Morphological distinction rests on the presence of three equal-sized leaflets with three evenly spaced commissures and three independent papillary muscles with separate chordal origins. 11 In the current case, three-dimensional TOE demonstrated the trifoil orifice morphology regarded as the accepted echocardiographic hallmark of a trileaflet configuration (Figure 2), and intraoperative inspection confirmed a deep central cleft producing three discrete leaflet segments, as previously described in the only other published case of trileaflet mitral valve specifically associated with hypertrophic cardiomyopathy. 12
The presence of multiple regurgitant jets at rest is itself a clinically important diagnostic signal. In HOCM, pure SAM-mediated MR typically produces a single posteriorly directed jet; detection of multiple jets, or a non-posteriorly directed component, indicates likely coexistent structural valve disease and should prompt detailed TOE assessment before committing to any septal reduction strategy. 13 In the largest published myectomy series, intrinsic mitral valve disease was identified pre-operatively in approximately 5% of patients and required concomitant mitral valve surgery. 14 In the present case, the combination of a centrally directed jet arising from the posterior leaflet cleft and an anteriorly directed jet from restriction of the anterior leaflet, alongside the 3D TOE morphological findings, was critical in recognising that alcohol septal ablation was contraindicated and that septal myectomy alone would be insufficient.
While medical management remains the first line for HOCM, patients with complex anatomy and persistent symptoms require surgical solutions.15–17 When MR arises from intrinsic valvular disease rather than SAM alone, septal myectomy is insufficient in isolation. Here, the distorted leaflet architecture and restricted anterior leaflet precluded repair, necessitating replacement. Congenital mitral valve anomalies, though rare, must be considered when regurgitation appears disproportionate to the degree of SAM or LVOT obstruction. Their presence may fundamentally alter operative strategy, tipping the balance toward replacement over repair, and surgery over catheter-based intervention.
This case highlights the importance of differentiating MR due to SAM versus intrinsic mitral valve disease in patients with HOCM. Further awareness and reporting of such rare anatomical variants are essential to inform surgical decision-making and improve long-term outcomes in this subset of patients.
Conclusion
This case highlights the diagnostic and surgical complexity when HOCM coexists with a congenital trileaflet mitral valve. Transoesophageal echocardiography, including three-dimensional assessment, was pivotal in identifying the true mechanism of MR and guiding surgical strategy, ultimately favouring mitral valve replacement over repair alongside septal myectomy. Rare congenital mitral anomalies should be actively considered when MR appears disproportionate to the degree of LVOT obstruction, as failure to recognise these variants risks suboptimal management. Continued reporting of such cases is essential to refine surgical decision-making in this uncommon but important subset of HCM patients.
Footnotes
Acknowledgements
The authors thank the clinical teams at both Royal Papworth Hospital and Hinchingbrooke Hospital for their contributions to the care of this patient. The authors would also specifically like to thank Dr Lynne Williams, Consultant Cardiologist at Royal Papworth Hospital for her contributions.
Ethical considerations
Ethical approval not required for reporting individual cases per our institutional policy.
Consent to participate
The patient provided written informed consent for all clinical care, as well as research participation and publication prior to the operation.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
No original data were generated for this report, other than that presented within it.