
Abstract
Objectives
Comparing clinical outcomes after cardiopulmonary bypass with hemodsorption (HA) versus cardiopulmonary bypass without HA in patients undergoing cardiac surgery in terms of mortality and major complications.
Methods
PubMed, Scopus, and Web of Science databases were searched for relevant randomized control trials (RCTs) that compared postoperative clinical outcomes between patients receiving intraoperative HA with cardiopulmonary bypass versus patients receiving cardiopulmonary bypass without intraoperative HA in cardiac surgery.
Results
Sixteen RCTs with 851 patients (433 in the HA group and 418 in the control group), were included in our meta-analysis. Our meta-analysis found no significant differences between the intraoperative HA group and the control group in patients undergoing cardiac surgery in terms of 30-days/in-hospital mortality, new-onset atrial fibrillation, stroke or cerebrovascular events, postoperative delirium, renal failure/acute kidney injury, need for renal replacement, postoperative liver dysfunction, thrombocytopenia, bleeding, volume of blood loss, pneumonia, sepsis, respiratory insufficiency, duration of postoperative ventilation, distributive/septic shock, pericardial tamponade, need for extracorporeal membrane oxygenation (ECMO) support, sequential organ failure assessment (SOFA) score at ICU admission, plasma-free hemoglobin levels, and fibrinogen levels. However, the pooled analysis showed a significant association between HA and decreased albumin at ICU admission (MD = − 0.28, 95% CI [0.55 to 0.01], p-value = 0.04), decreased length of ICU stay (MD = −0.66, 95% CI [−1.24 to 0.08], p-value = 0.03), and decreased length of hospital stay (MD = −0.99, 95% CI [−1.88 to −0.10], p-value = 0.03).
Conclusion
Our findings suggest that there is not enough evidence to endorse the role of routine intraoperative HA during cardiopulmonary bypass in improving clinical outcomes after cardiac surgery. Factors such as patient risk profile, procedure complexity, and cost implications should be taken into account when considering this adjunct therapy.
Introduction
Cardiopulmonary bypass (CPB) revolutionized heart surgery by facilitating safe, motionless, and bloodless surgical field while maintaining adequate end organs perfusion. 1 Despite its benefits, CPB is typically associated with an intense inflammatory reaction that can result in significant organ injury, such as. 2 CPB duration is an independent predictor of morbidity and mortality; each 30-min increment increases the odds of death by 57%, renal complications by 31%, and multiorgan failure by 21% 3 This translates into increased inotrope requirements, prolonged mechanical ventilation, and longer hospital stay.4,5 To mitigate the inflammatory response associated with CPB, hemoadsorption (HA) has emerged as a new intraoperative intervention. This technique involves the use of adsorptive devices, particularly Cytosorb®, which is aimed at removing pro- and anti-inflammatory mediators from circulation during CPB. 6 In 1965, Yatzidis and colleagues pioneered sorbent-based HA in the use of barbiturate poisoning. 7 Over five decades, improvements in sorbent technology and the use of biocompatible polymer sorbents as in CytoSorb have made it safer and more feasible. Since then, its use in scenarios such as sepsis, ECMO, and cardiac surgery has been studied but with mixed inconclusive results. 6 Cytosorb® uses porous polymer pearls to adsorb hydrophobic molecules, including cytokines, to attenuate systemic inflammation during and immediately after CPB. 8 There are other devices that vary in mechanism, and clinical use like DrugSorb used for removal of antithrombotic drugs; Oxiris, used in AKI because it also combines dialysis and cytokine adsorption; Seraph-100, that was used in COVID and Toraymyxin (PMX-DHP), used for endotoxemia in gram-negative sepsis.9,10,11,12
The inflammatory burden of CPB is not the same across all scenarios. 13 HA appears more justified in high-risk cases like infective endocarditis, complex aortic surgery and cardiac reoperations, than routine elective procedures.6,14 Acute infective endocarditis cases have higher in-hospital mortality rates than non-endocarditis cases. 13 Similarly, complex aortic surgery with hypothermic circulatory arrest carries perioperative mortality up to 14.9%. 15 Reoperative cardiac surgery is an independent predictor of 30-days and long-term mortality. 16
In patients with acute infective endocarditis undergoing cardiac surgery, HA has been proposed as a strategy to improve hemodynamics, reduce sepsis-related mortality, and preserve organ function. However, recent reviews highlighted the ongoing debate about its clinical efficacy, emphasizing the need for more robust data. 14 Studies such as the REMOVE and RECCAS trials have shown promising reductions in cytokine levels, less need for vasopressor support, and improved hemodynamic parameters. However, these findings did not translate into significant improvement in postoperative outcomes.17,18 Due to lack of comprehensive studies assessing the effect of intraoperative HA on post-operative clinical outcomes in patients undergoing cardiac surgery, this systematic review and meta-analysis aimed to assess the effect of HA on clinical outcomes, including mortality, myocardial infarction (MI), atrial fibrillation (AF), and AKI in patients undergoing cardiac surgery.
Methods
This meta-analysis was conducted in compliance with the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines 19 and the Cochrane handbook for systematic reviews of interventions. 20
Search strategy
Using this search strategy ((haemoadsorption OR cytosorb OR adsorber) AND (cardiac surgery)), we searched PubMed, Web of Science, and Scopus databases for relevant randomized control trials from inception to January 3, 2025.
Inclusion and exclusion criteria
We included only randomized control trials that compared intraoperative HA with CPB versus CPB without intraoperative HA in patients undergoing cardiac surgery in terms of clinical outcomes. We excluded cross sectional, cohort, and case-control studies. Animal studies, case reports, case series, editorials, non-English studies, and conference abstracts were also excluded. The inclusion criteria were randomized control trials that compared clinical outcomes post-cardiac surgery between patients receiving intraoperative HA with CPB versus patients undergoing CPB without intraoperative HA.
Study selection process
Two independent authors (K.R.M & L.A) revised the titles and/or abstracts of the searched papers to determine relevant studies. Then, the two authors revised the full texts of the retrieved reports independently. Any conflicts between authors were solved by mutual agreement after discussion.
Data extraction and management
Two independent authors used an excel sheet to extract the following data: the first author’s last name, year of publication, age, gender, number of patients, baseline hemoglobin, type of surgery and outcome measurements: primary outcome; mortality (30-days)/in-hospital mortality, and secondary outcomes including stroke/cerebrovascular events, renal failure or acute kidney injury, thrombocytopenia, renal replacement therapy, postoperative liver dysfunction, postoperative delirium, albumin at ICU admission (g/dl), bleeding, pericardial tamponade, pneumonia, respiratory insufficiency, infectious complications, sepsis, distributive shock (septic shock), ECMO Support, new-onset atrial fibrillation, ICU length of stay (days), hospital length of stay (days), sequential organ failure assessment (SOFA) at ICU admission, volume loss/blood loss (ml), plasma free hemoglobin post CBP (ICU Admission) (mg/ml), fibrinogen at ICU admission (mg/dl), duration of postoperative ventilation (hours). Any conflicts between authors were solved by the first author.
Risk of bias
The Risk of Bias 2 (RoB 2) tool was used to assess the risk of bias of the included randomized control trials; each study was classified as: high risk, some concerns, or low risk of bias.
Data analysis
Data were analyzed using Review Manager (RevMan) software, version 5.4. Sensitivity analysis (leave-one-out test) was used. Continuous data were presented as mean difference (MD) with 95% confidence interval (CI), and dichotomous data were presented as risk ratio (RR) with 95% confidence interval (CI). If no heterogeneity was observed, results were presented in a fixed –effect model, and a random-effect model was used if significant heterogeneity was observed. Results were considered significant if the p-value was less than 0.05.
Results
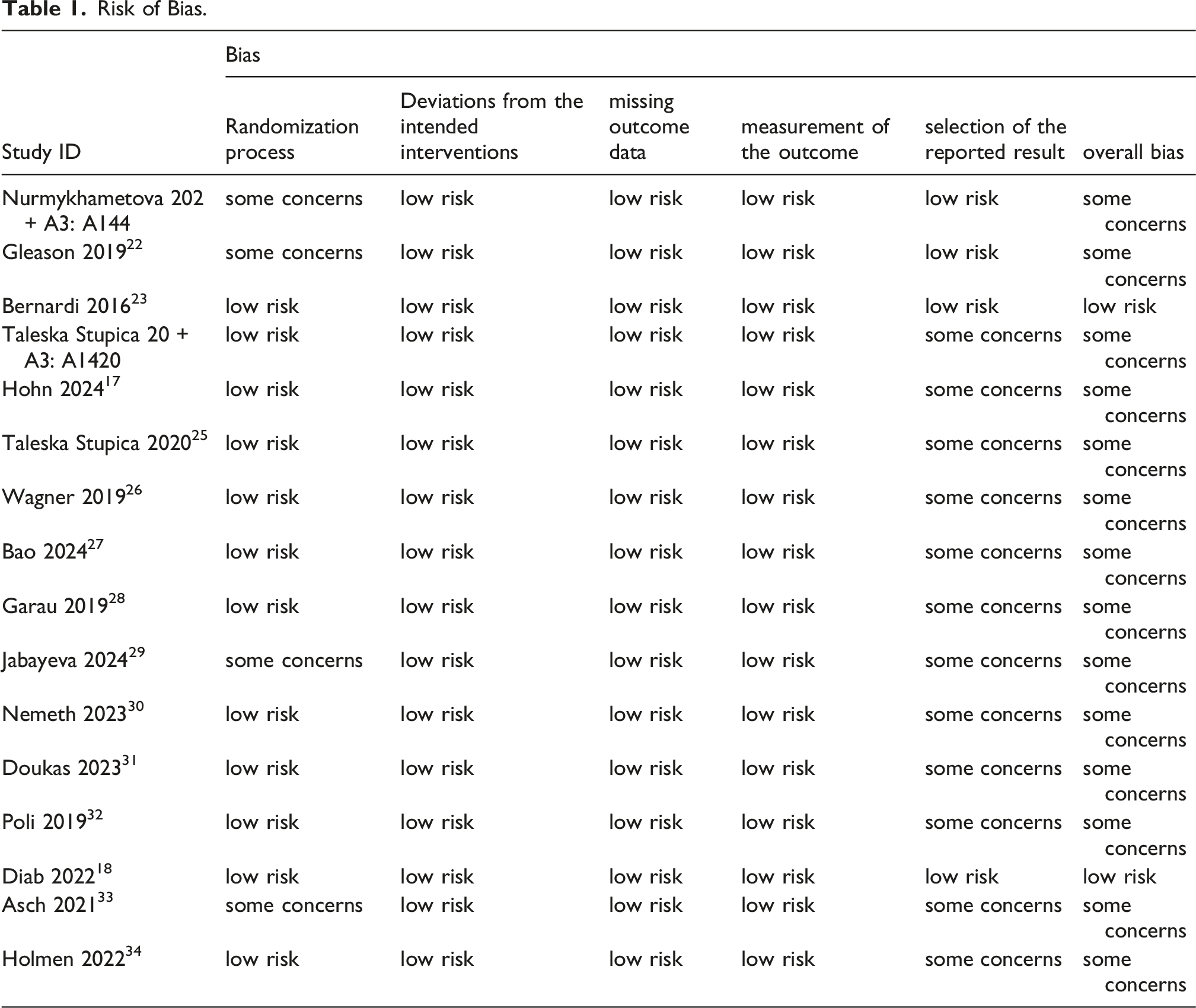
Our search strategy identified a total of 556 studies, of which 399 were eligible for title and abstract screening after duplicate removal. A total of 71 studies were eligible for full-text screening. Ultimately, 16 studies were included in our meta-analysis17,18,21–34 as shown in the PRISMA (Figure 1). The overall risk of bias was low risk in two studies, and some concerns in 14 studies as shown in Table 1. PRISMA flow diagram. Risk of Bias.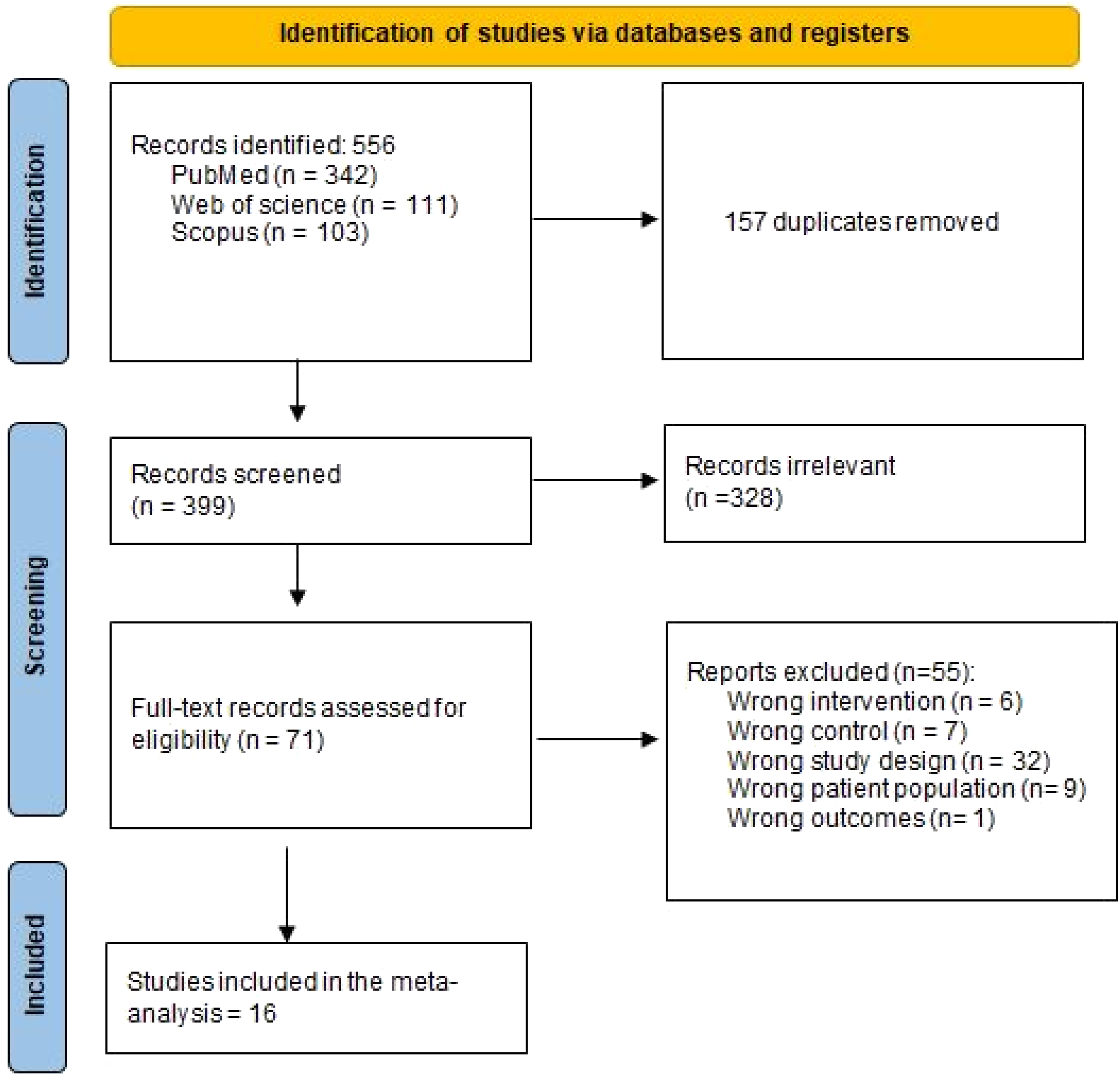
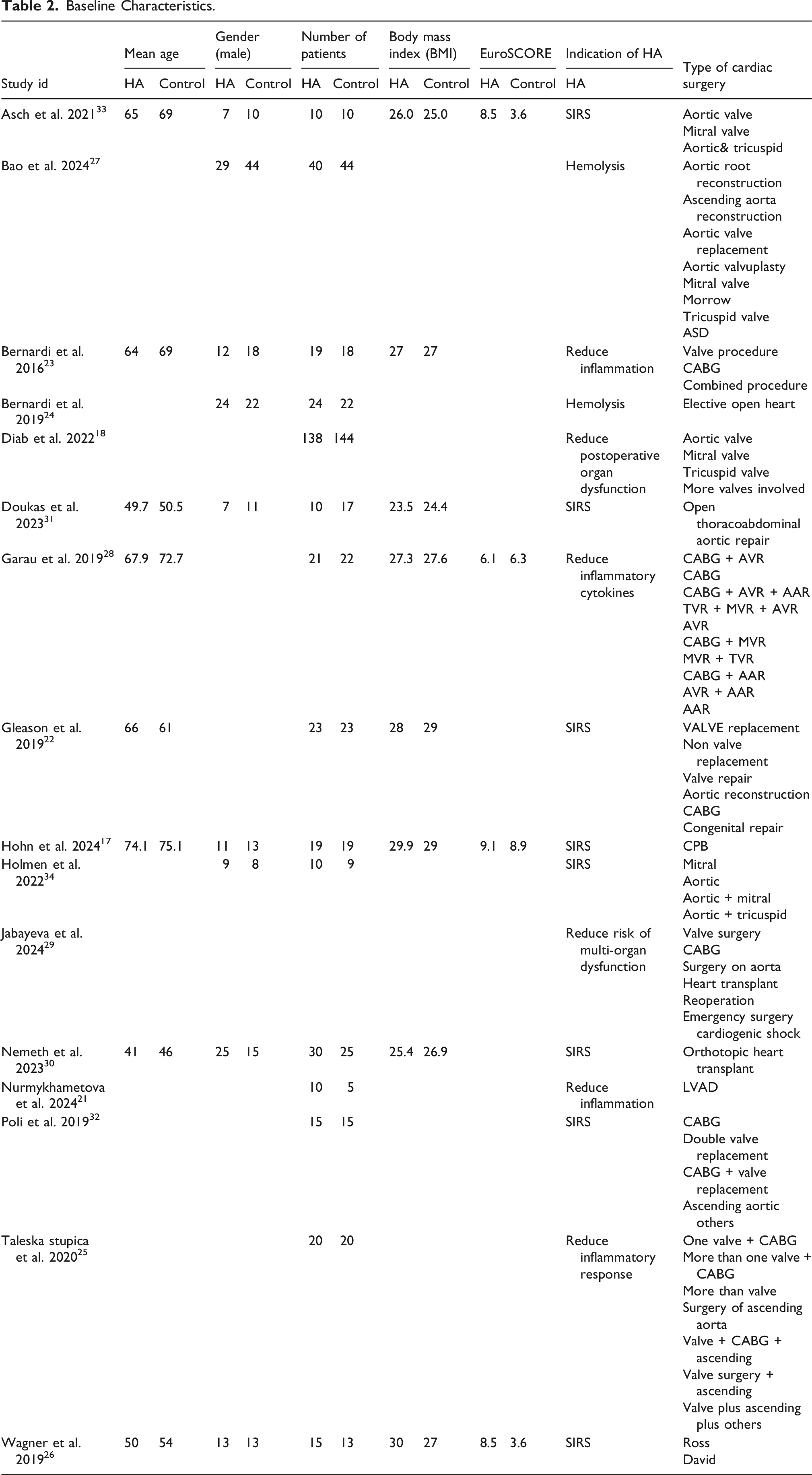
Baseline Characteristics.
Primary outcome
The pooled analysis showed no statistically significant difference between HA group and control group in terms of mortality (30-days)/in-hospital mortality (RR = 0.99, 95% CI [0.68–1.46], p-value = 0.97) (Figure 2). We observed no statistically significant heterogeneity among studies in mortality (30-days)/in-hospital mortality (I2 = 0%, p-value = 0.64). Mortality (30-days)/In-hospital mortality.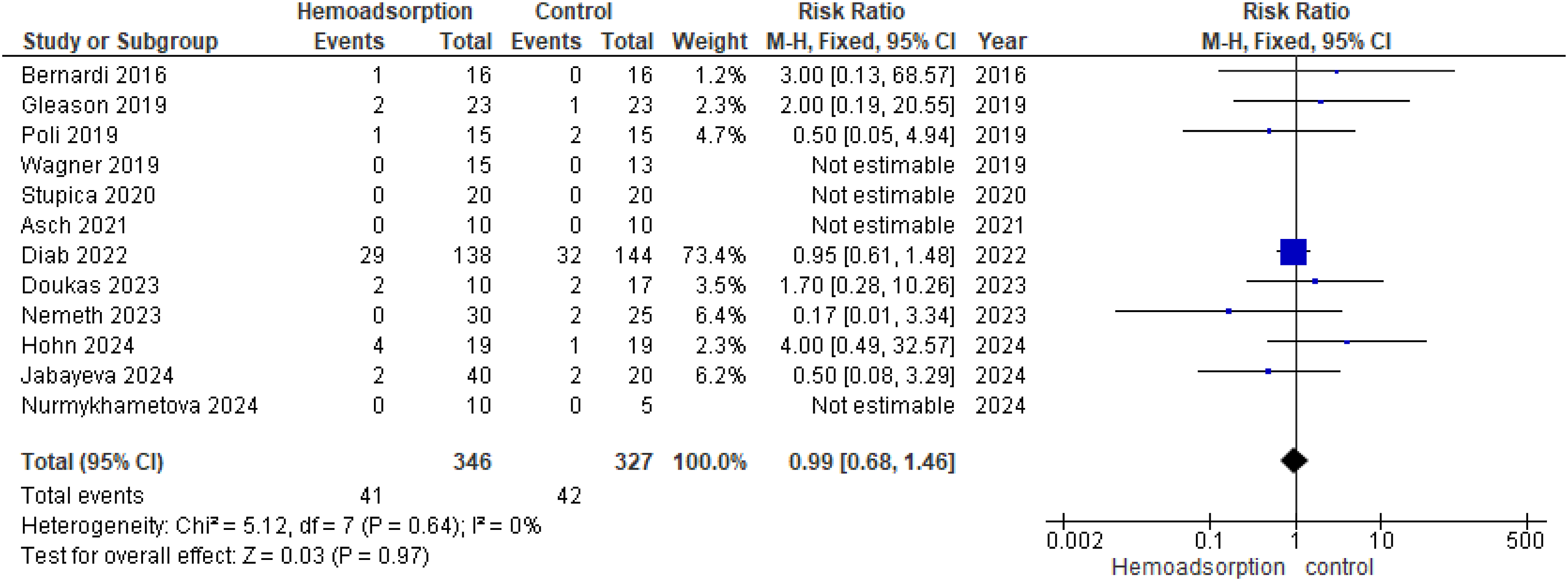
Secondary outcomes
The pooled analysis showed no statistically significant difference between HA group and control group regarding stroke/cerebrovascular events (RR = 0.86, 95% CI [0.35–2.13], p-value = 0.75) (Figure 3(a)), renal failure/acute kidney injury (RR = 0.84, 95% CI [0.71–1.00], p-value = 0. 06) (Figure 3(b)), thrombocytopenia (RR = 1.23, 95% CI [0.74–2.07], p-value = 0.43) (Figure 3(c)) and renal replacement therapy (RR = 0.84, 95% CI [0.31–2.24], p-value = 0.72) (Figure 3(d)). We observed no statistically significant heterogeneity among studies in stroke/cerebrovascular events (I2 = 37%, p-value = 0.19), renal failure/acute kidney injury (I2 = 32%, p-value = 0.17), thrombocytopenia (I2 = 0%, p-value = 0.68), and renal replacement therapy (I2 = 0%, p-value = 0.40). Clinical outcomes 1.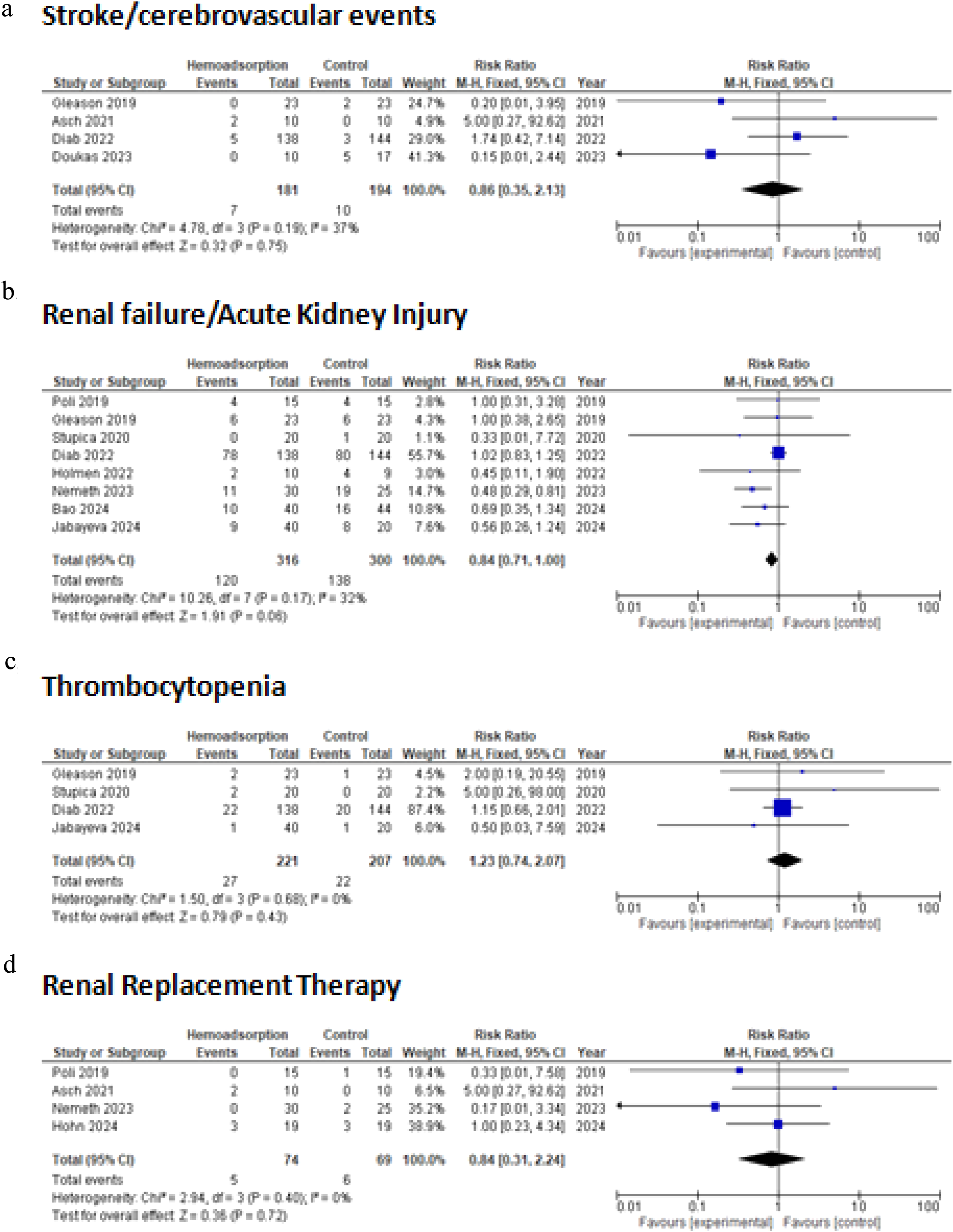
The pooled analysis showed no statistically significant difference between HA group and control group regarding post-op liver dysfunction (RR = 0.69, 95% CI [0.31–1.52], p-value = 0.36) (Figure 4(a)), and postoperative delirium (RR = 0.67, 95% CI [0.36–1.24], p-value = 0.20) (Figure 4(b)). The pooled analysis revealed a statistically significant association between HA and decreased albumin at ICU admission (MD = − 0.28, 95% CI [0.55 to 0.01], p-value = 0.04) (Figure 4(c)). We observed no statistically significant heterogeneity among studies in post-op liver dysfunction (I2 = 41%, p-value = 0.16), postoperative delirium (I2 = 41%, p-value = 0.16) and albumin at ICU admission (g/dl) (I2 = 0%, p-value = 0.47). Clinical outcomes 2.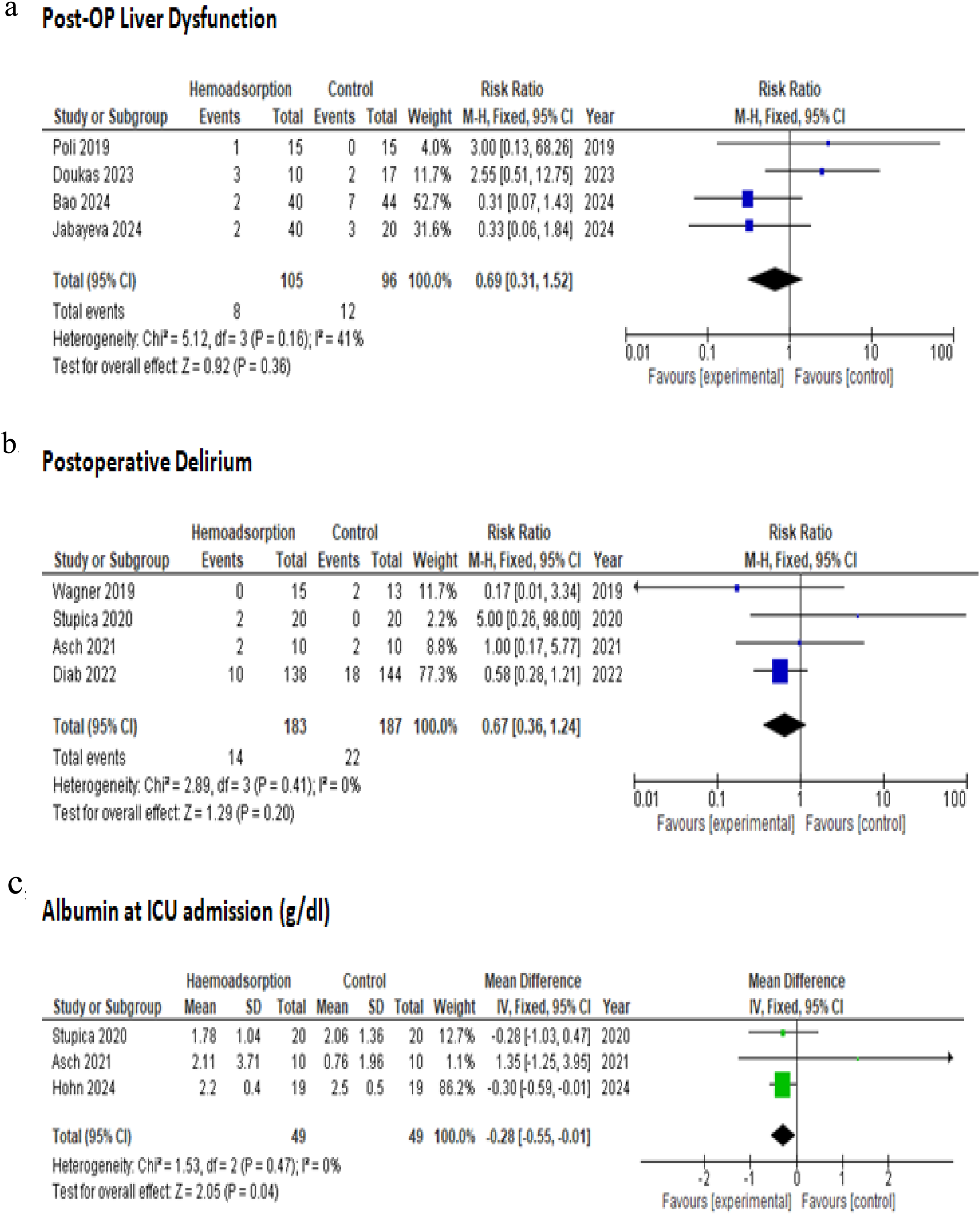
The pooled analysis showed no statistically significant difference between HA group and control group regarding bleeding (RR = 1.01, 95% CI [0.62–1.65], p-value = 0.96) (Figure 5(a)), pericardial tamponade (RR = 1.04, 95% CI [0.37–2.89], p-value = 0.94) (Figure 5(b)) and pneumonia (RR = 1.19, 95% CI [0.71–2.00], p-value = 0.51) (Figure 5(c)). We observed no statistically significant heterogeneity among studies in bleeding (I2 = 0%, p-value = 0.61), pericardial tamponade (I2 = 0%, p-value = 0.98) and pneumonia (I2 = 0%, p-value = 0.42). Clinical outcomes 3.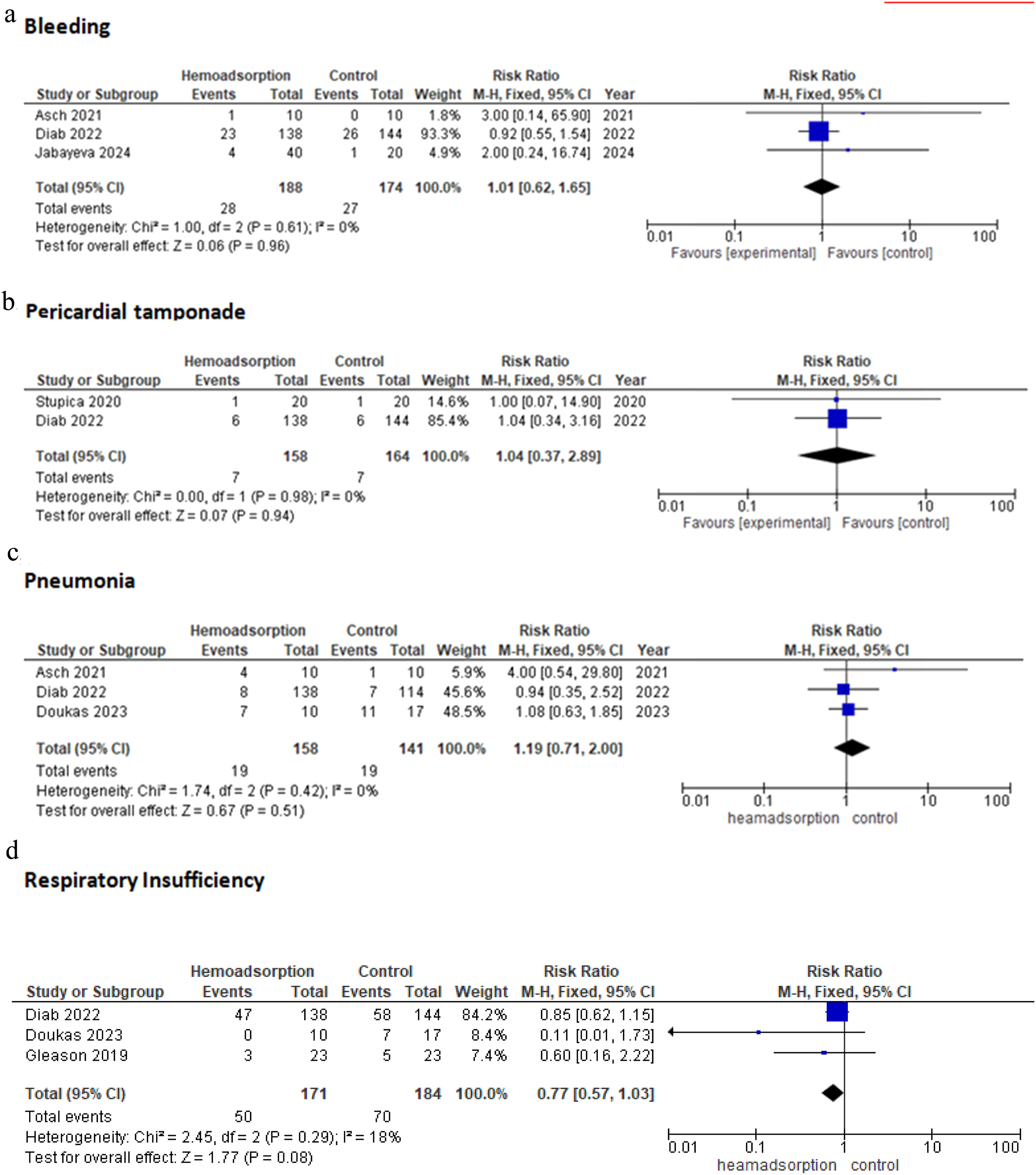
The pooled analysis showed no statistically significant difference between HA group and control group regarding respiratory insufficiency (RR = 0.77, 95% CI [0.57–1.03], p-value = 0.08) (Figure 5(d)), infectious complications (RR = 0.78, 95% CI [0.34–1.81], p-value = 0.57) (Figure 6(a)) and sepsis (RR = 0.62, 95% CI [0.22–1.76], p-value = 0.37) (Figure 6(b)). We observed no statistically significant heterogeneity among studies in respiratory insufficiency (I2 = 18%, p-value = 0.29), infectious complications (I2 = 28%, p-value = 0.25), and sepsis (I2 = 0%, p-value = 0.57). Clinical outcomes 4.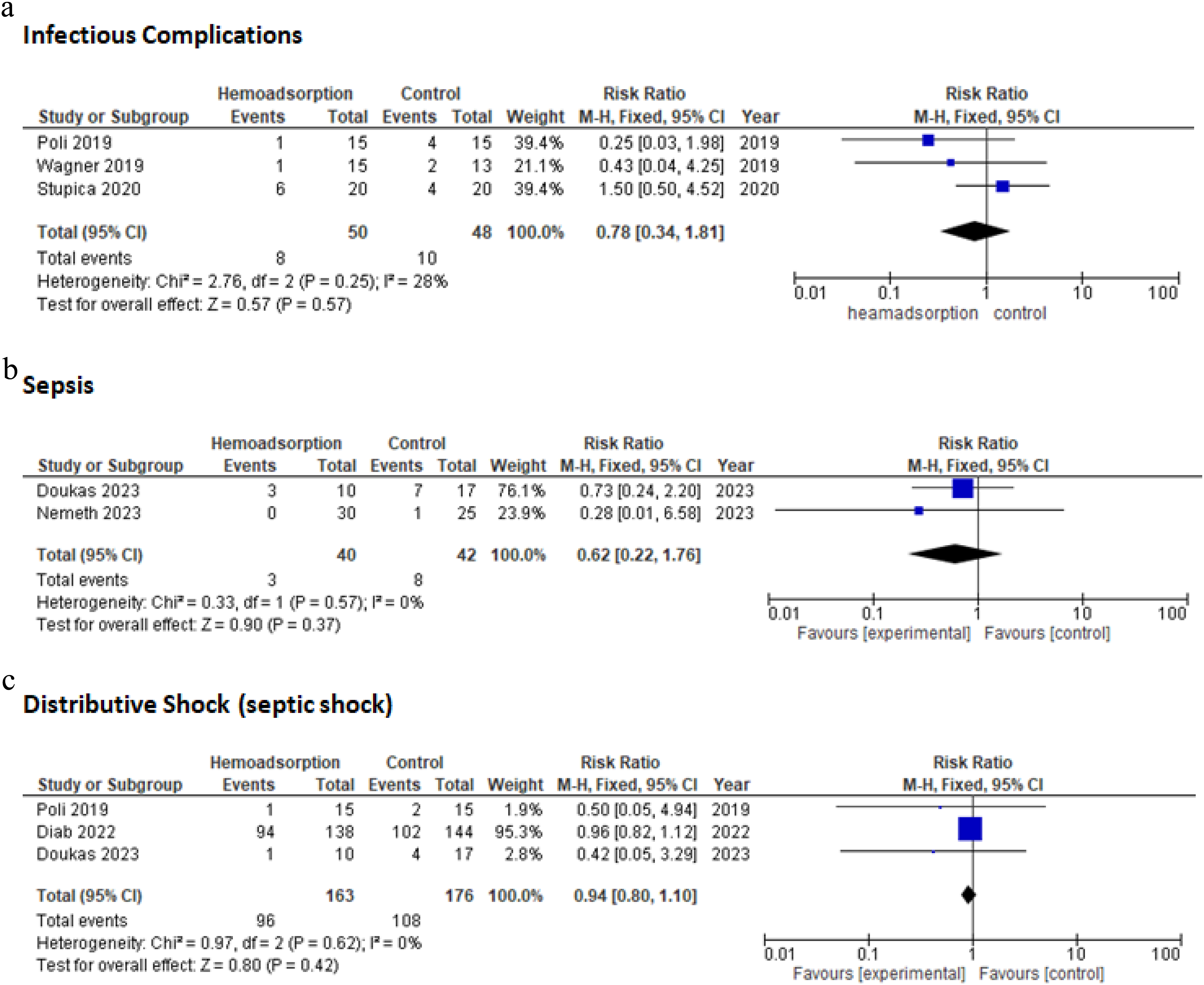
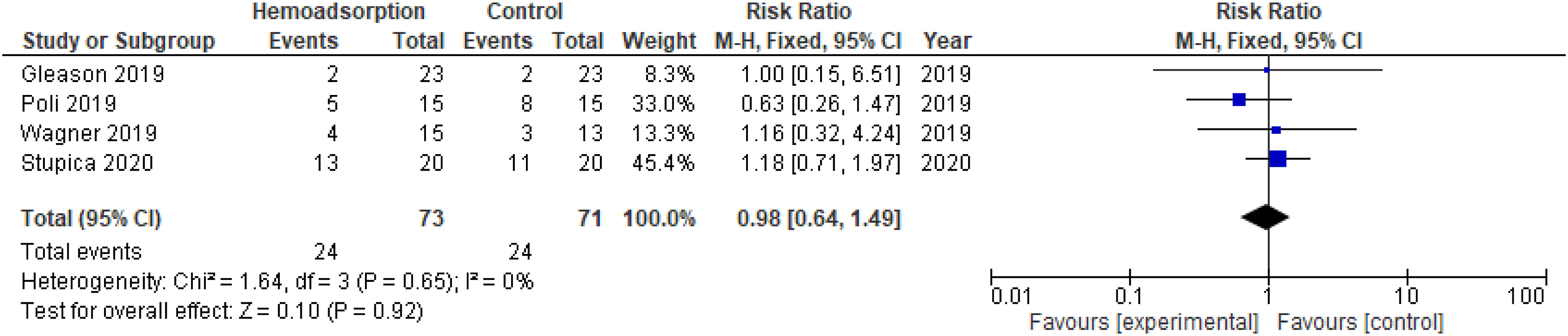
The pooled analysis showed no statistically significant difference between HA group and control group regarding distributive shock (septic shock) (RR = 0.94, 95% CI [0. 80–1.10], p-value = 0.42) (Figure 6(c)), ECMO Support (RR = 1.50, 95% CI [0.62–3. 60], p-value = 0.36) (Figure 7) and new-onset atrial fibrillation (RR = 0.98, 95% CI [0.64–1.49], p-value = 0.92) (Figure 8). We observed no statistically significant heterogeneity among studies in distributive shock (septic shock) (I2 = 0%, p-value = 0.62), ECMO Support (I2 = 5%, p-value = 0.38) and new-onset atrial fibrillation (I2 = 0%, p-value = 0.65). Ecmo support. New onset atrial fibrillation.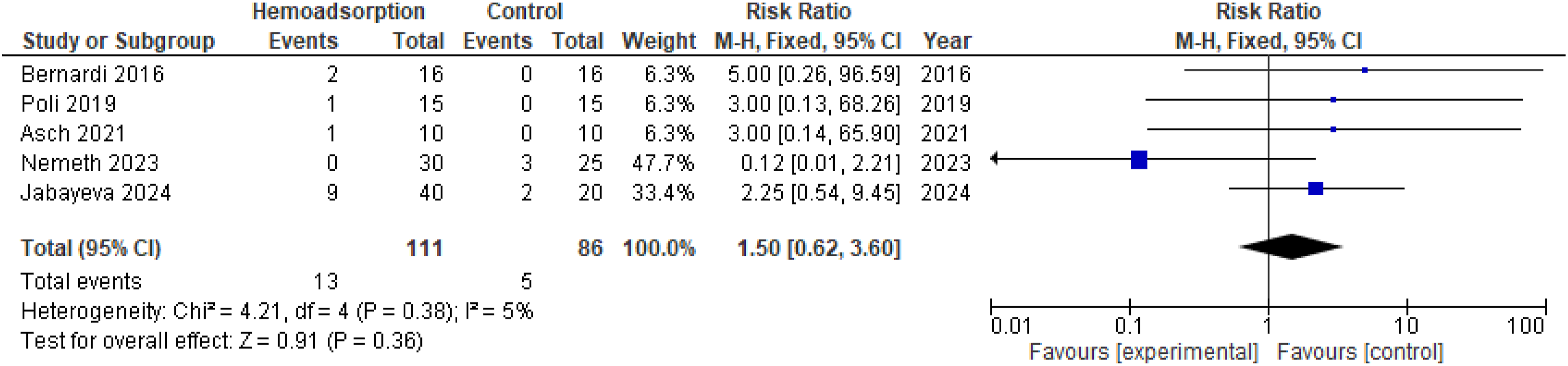
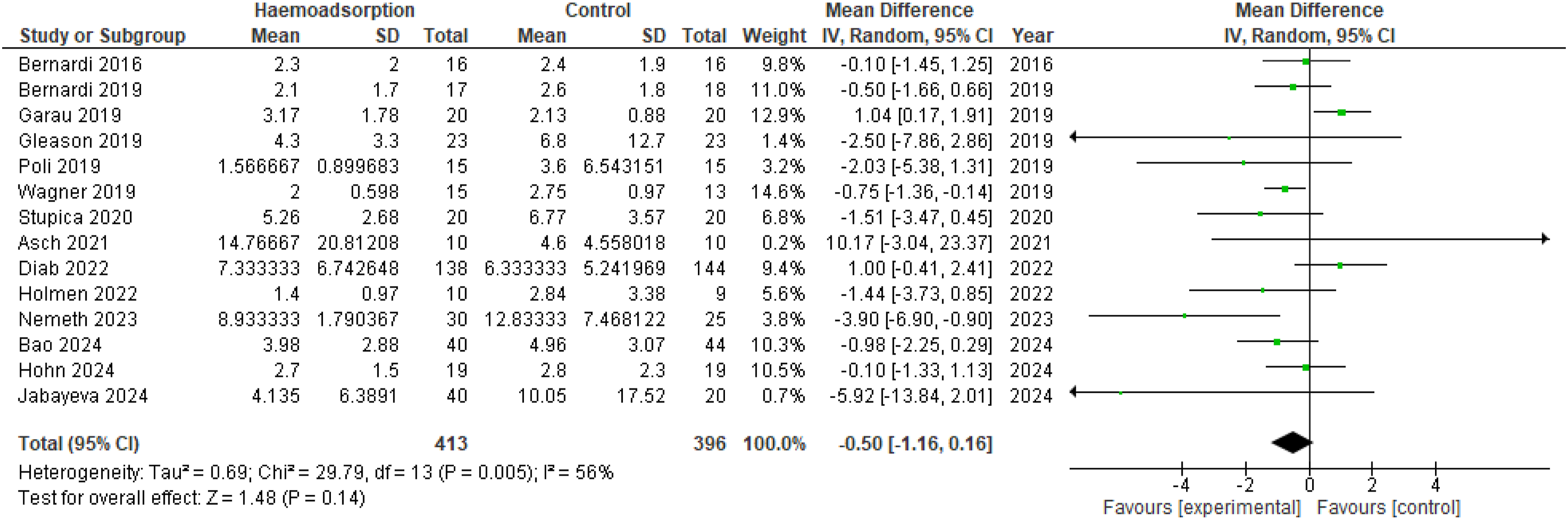
The pooled analysis showed no statistically significant difference between HA group and control group regarding duration of postoperative use of vasopressors/catecholamine therapy (NE) (MD = −3.58, 95% CI [−27.16 to 20.00] p-value = 0.77) (Figure 9), and ICU length of stay (MD = −0.50, 95% CI [−1.16 to 0.16], p-value = 0.14) (Figure 10). Duration of postoperative use of vasopressors/Catecholamine therapy (NE) (hours). ICU length of stay (days).
In terms of duration of post-operative use of vasopressors/catecholamine therapy, we observed a significant heterogeneity among studies (I2 = 67%, p-value = 0.03) that was solved by leave-one-out test (I2 = 0%, p-value = 0.68) by removing the study (Diab 2022). After solving heterogeneity, the pooled analysis also showed no statistically significant difference between HA group and control group (MD = −14.09, 95% CI [−29.33 to 1.15], p-value = 0.07). In ICU length of stay outcome, we observed a significant heterogeneity among studies (I2 = 56%, p-value = 0.005) that was solved by leave-one-out test (I2 = 34%, p-value = 0.11) by removing the study (Garau 2019). After solving heterogeneity, the pooled analysis showed a statistically significant association between HA group and decreased length of ICU stay (MD = −0.66, 95% CI [−1.24 to 0.08], p-value = 0.03).
The pooled analysis showed a statistically significant association between HA group and decreased length of hospital stay (MD = −0.99, 95% CI [−1.88 to −0.10], p-value = 0.03) (Figure 11). However, the pooled analysis showed no difference between both groups regarding sequential organ failure assessment (SOFA) at ICU admission (MD = 0.79, 95% CI [−0.38 to 1.97], p-value = 0.19) (Figure 12(a)) and volume loss/blood loss (MD = −0.96, 95% CI [−200.39 to 198.47], p-value = 0.99) (Figure 12(b)). We observed no statistically significant heterogeneity among studies in duration hospital length of stay (I2 = 11%, p-value = 0.34), sequential organ failure assessment (SOFA) at ICU admission (I2 = 0%, p-value = 0.63) and volume loss/blood loss (ml) (I2 = 0%, p-value = 0.40). Hospital length of stay (days). Clinical outcomes 5.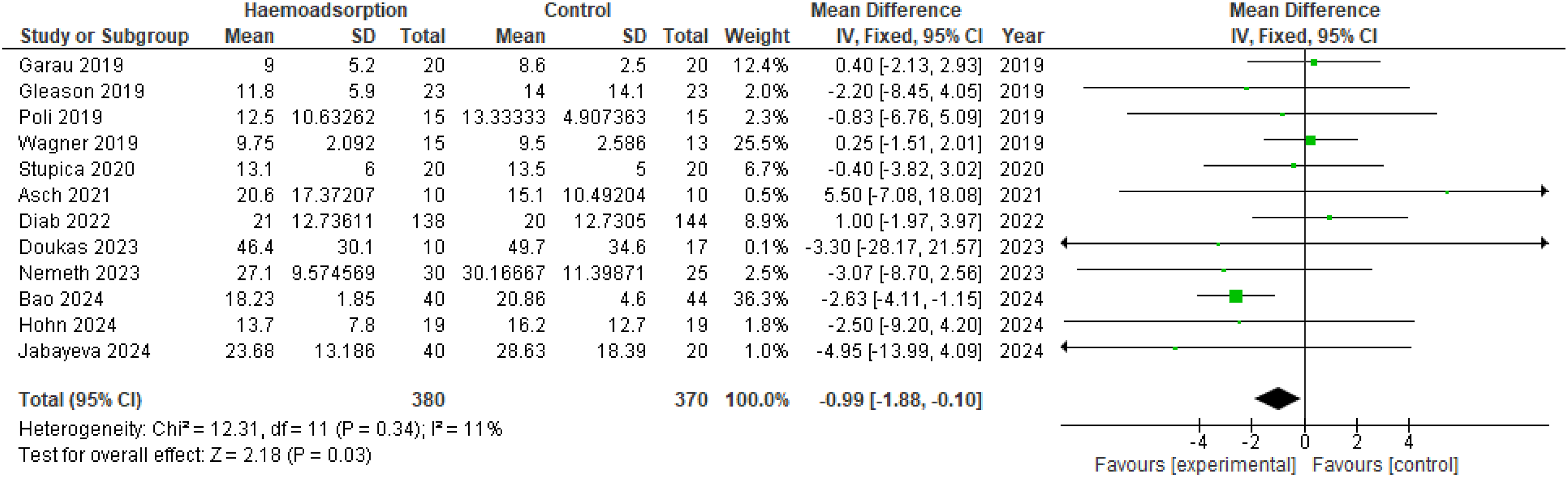
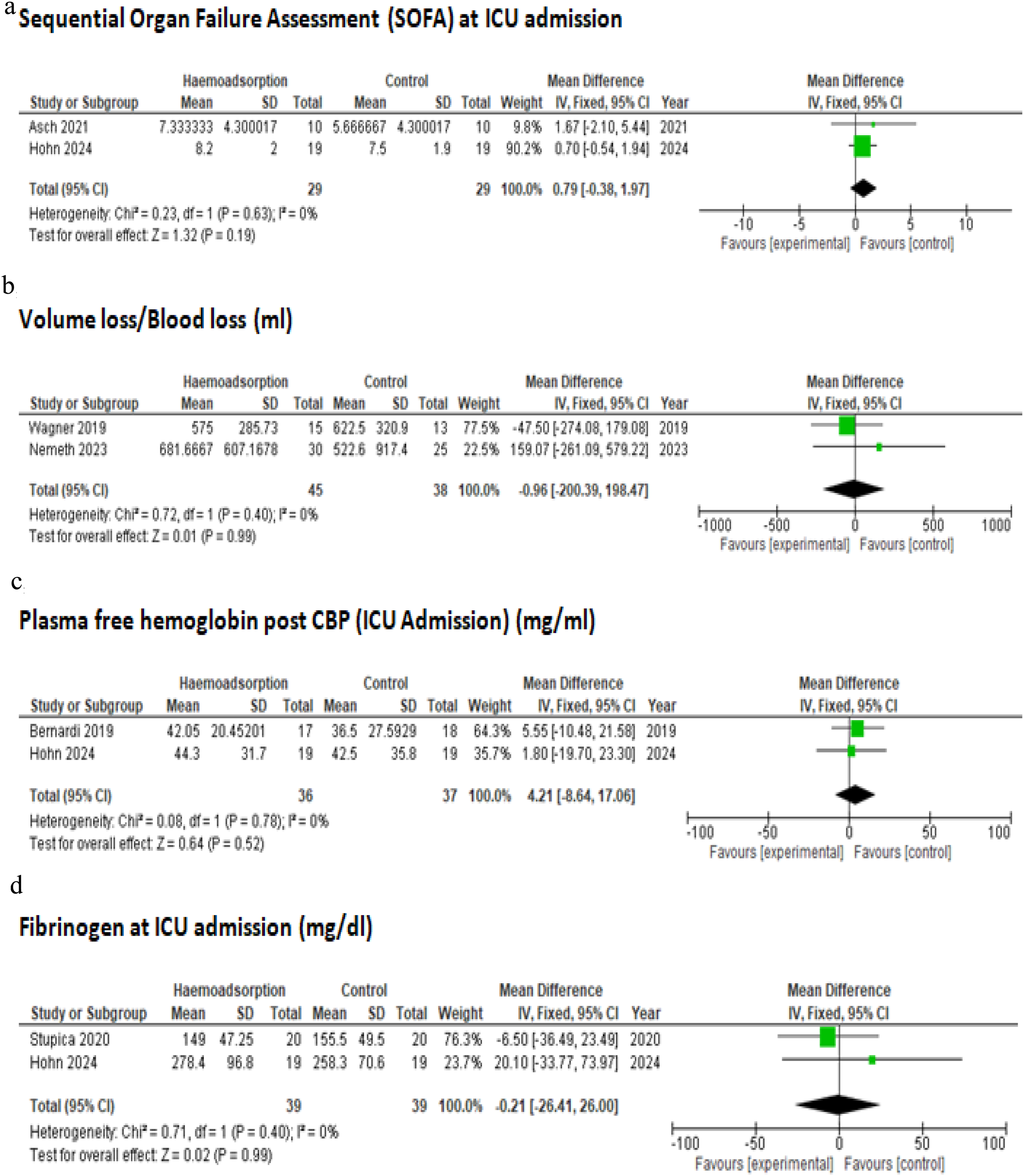
The pooled analysis showed no statistically significant difference between the HA group and control group regarding plasma-free hemoglobin post CBP (ICU Admission) (MD = 4.21, 95% CI [−8.64 to 17.06], p-value = 0.52) (Figure 12(c)), fibrinogen at ICU admission (MD = −0.21, 95% CI [−26.41 to 26.00], p-value = 0.99) (Figure 12(d)) and duration of post-operative ventilation (MD = −2.38, 95% CI [−16.62, 11.58], p-value = 0.74) (Figure 13). We observed no statistically significant heterogeneity among studies in plasma free hemoglobin (I2 = 0%, p-value = 0.78) and fibrinogen at ICU admission (mg/dl (I2 = 0%, p-value = 0.40). We observed a significant heterogeneity among studies in duration of post-operative ventilation outcome (I2 = 74%, p-value <0.0001) that wasn’t solved by leave-one test. Duration of post-operative ventilation (hours).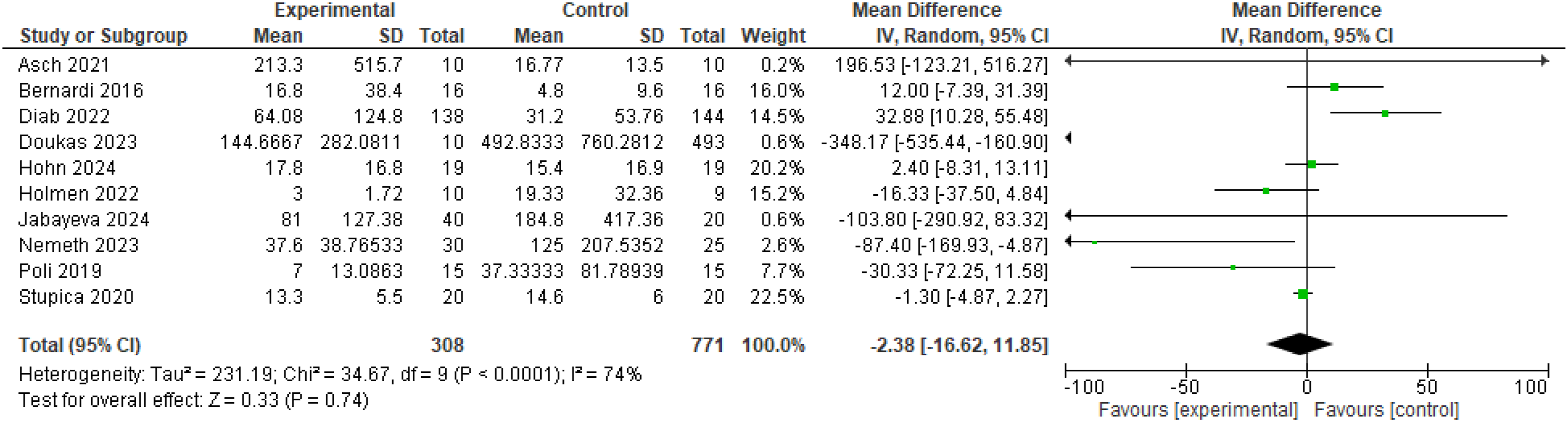
Discussion
Our meta-analysis found no significant differences between the intraoperative HA group and the control group in patients undergoing cardiac surgery in terms of the primary outcome of 30-days/in-hospital mortality. In terms of the secondary outcomes, the analysis also found no significant differences between the intraoperative HA group and the control group regarding new-onset atrial fibrillation, neurological complications (stroke or cerebrovascular events, and postoperative delirium), renal outcomes (renal failure or acute kidney injury, and need for renal replacement therapy), hepatic dysfunction (postoperative liver dysfunction), hematologic parameters (thrombocytopenia, bleeding, and volume or blood loss), infectious complications (pneumonia, sepsis, and other infectious events), respiratory outcomes (respiratory insufficiency and duration of postoperative ventilation), and hemodynamic instability (distributive or septic shock), consistent with previously published studies by Hohn et al., Bernardi et al., and Poli et al.17,23,32
Additionally, there was no significant difference in surgical complications (re-thoracotomy, reoperation, or re-exploration; pericardial tamponade), need for extracorporeal membrane oxygenation (ECMO) support, or intensive care metrics such as, SOFA score at ICU admission, plasma-free hemoglobin levels, fibrinogen levels. Nonetheless, our meta-analysis showed a significant decrease in albumin at ICU admission, decreased ICU length of stay, and decreased hospital length of stay in patients receiving intraoperative HA during cardiac surgery compared with patients in the group without HA, which is consistent with a previously published study. 31 A lack of benefit was also observed in patients with higher inflammatory burden in a larger multicentric study published by Diab et al., 2022, which enrolled 288 high-risk patients undergoing cardiac surgery for infective endocarditis. 18 On the contrary, a study published by Asch et al. showed that patients with endocarditis who received HA had longer ICU stays. 33 However, patients undergoing heart transplantation had better outcomes on HA than without, but no differences in mortality rates were observed. 30 One of the potential reasons why intraoperative HA did not improve clinical outcomes is that it might not be sufficient in general cardiac surgery patients who have intermediate burden, but its effect may be tangible in higher burden patients. The intraoperative window may represent too short duration to capture the potential benefits of cytokine clearance, as opposed to prolonged or repeated HA used in critical care settings like septic shock. Intended advantage of HA may be countered by the removal of protective or necessary circulating proteins, such as decreasing levels of albumin, as shown in our meta-analysis. Although mortality and ICU metrics were not affected, shorter ICU and hospital length of stay could reflect faster clinical stabilization in selected patients. Moreover, the inclusion of studies with varying indications for HA therapy and various cardiac surgery procedures may have caused the overall non-significant results of the outcomes. HA duration or frequency might not have been sufficient to achieve therapeutic effect post-cardiac surgery.
Our findings suggest that the hemadsorption might be beneficial in select high-risk subgroups, such as transplant patients, but not in the general cardiac surgery population undergoing CPB. Future studies should focus on identifying patient phenotypes most likely to benefit from HA and explore whether extended HA in the postoperative phase yields different outcomes than the in the intraoperative approach.
Strengths and limitations
Our meta-analysis included only randomized control trials and there was no detected heterogeneity among studies in most of the reported outcomes, giving strong evidence for our study. However, there are some limitations in the study. First, the overall relatively small sample size may limit the generalizability of our conclusions. Second, there is a range of differences between studies in how HA is applied, including the timing of initiation, duration of use, and blood flow rates. Finally, the included studies focused on general cardiac surgery and did not categorize the effect of HA on different patient sub-populations which may have influenced the results.
Conclusion
Our findings suggest that currently there is not enough evidence to endorse the role of intraoperative hemadsorption in improving postoperative outcomes in patients undergoing cardiac surgery. Larger multi-center randomized controlled trials are needed to better define its potential benefit in specific high-risk populations and justify its incorporation in the routine clinical practice.35,36
Footnotes
Ethical considerations
Not applicable, as it is a meta-analysis study.
Consent to participate
Not applicable, as it is a meta-analysis study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are available within the manuscript, as it is a systematic review and meta-analysis. Data excel sheet is available upon a request.