
Abstract
Chronic venous ulcers (CVUs) occur in approximately 1% of the general population. Risk factors for chronic venous disease (CVD) include heredity, age, female sex and obesity. Although not restricted to the elderly, the prevalence of CVD, especially leg ulcers, increases with age.1 CVD has a considerable impact on health-care resources. It has been estimated that venous ulcers cause the loss of approximately two million working days and incur treatment costs of approximately $3 billion per year in the USA.2 Overall, CVD has been estimated to account for 1–3% of the total health-care budgets in countries with developed health-care systems.1 The pathophysiology of dermal abnormalities in CVU is reflective of a complex interplay that involves sustained venous hypertension, inflammation, changes in microcirculation, cytokine and matrix metalloproteinase (MMP) activation, resulting in altered cellular function and delayed wound healing.3,4
Keywords
Inflammatory cells and CVUs
Leukocytes have been demonstrated to be increased in the lower extremities of patients with CVD. In fact, as the disease clinical class progresses there are increasing number of leukocytes in the dermis of the lower extremity that are independent of limb position. 5 In patients with severe lipodermatosclerotic (LDS) skin changes, a study determined that the predominant cell types found were T-lymphocytes and macrophages but rarely were neutrophils observed, and expression of intercellular adhesion molecule-1 (activation of leukocytes to adhere to the endothelium) was elevated. This indicates that the accumulation and adhesion of macrophages and T-lymphocytes in the perivascular and dermal matrix was associated with chronic venous insufficiency (CVI) skin changes and ulceration. 6 Further interactions with endothelial cells (leukocyte/endothelial signaling) to allow the leukocytes to reach the dermal tissue have been investigated. Immunohistochemical analysis of biopsies obtained adjacent to ulcerated skin evaluated changes in adhesion molecules in patients with severe LDS and active ulceration, demonstrated that increased expression of intracellular adhesion molecule-1 (CD54, expressed on macrophages, endothelial and dendritic cell, cell surface marker antigen that activates T-cells via LFA-1) and vascular cell adhesion molecule-1 was present. In addition, the expression of lymphocyte function-associated antigen-1 and very late activated antigen-4 was dramatically increased on perivascular leukocytes compared with healthy skin, indicating that the upregulation of adhesion molecules in CVI patients are important mediators that can facilitate leukocyte endothelial adhesion, activation and trans-endothelial migration into the extracellular space. 7 In an elegant study of patients with CVD (varicose veins with and without skin changes), patients were subjected to 30 minutes of venous hypertension and then returned to the supine position prior to sampling blood from the foot vein in order to study leukocyte endothelial adhesion in patients who were subjected to short-term venous hypertension. This resulted in decreased levels of neutrophil and monocyte CD11b (leukocyte surface expression) and L-selectin, and increased plasma levels of soluble L-selectin, suggesting that leukocytes shed L-selectin upon attachment to the endothelium. The authors concluded that venous hypertension resulted in sequestration of activated neutrophils and monocytes in microcirculation in patient limbs with venous disease, which persisted despite reversal of venous hypertension. 8
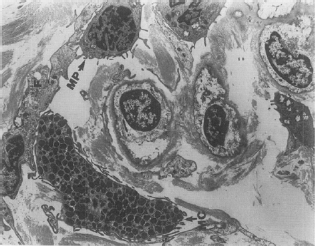
An important study determined that tissues with severe LDS and healed ulcers contained significant numbers of mast cells around arterioles and postcapillary venules, and in active ulcers macrophages were predominantly located in the postcapillary venule (Figure 1). In addition, the effects of mast cells and macrophages appear to be mediated in part by transforming growth factor-β1 (TGF-β1) probably released by leukocytes and mast cells in venous leg ulcers.
9
The importance of leukocytes, in addition to other cell types including endothelial cells, fibroblast and keratinocytes, is their ability to produce and secrete cytokines, growth factors and MMPs.
10
Leukocytes are an important source of proteinases, and mast cells are known to release chymase which is a potent activator of MMP-1 and MMP-3.
9
Postcapillary venule surrounded by a mast cell (MC) and a macrophage (MC)
9
Cytokines and growth factors in CVUs
The determining factors of CVU that heal versus those that remain non-healing involve a complex interplay of inflammatory cells, inflammatory cytokines, growth factors and MMPs.
3
In LDS there is an increase in interleukin-1a (IL-1a) and IL-1β in the dermis but not in the epidermis, and no increases in tumour necrosis factor-α (TNF-α).
6
In a study of patients with CVU, healing and non-healing ulcers were assessed by examining the composition of cytokines present in the ulcer wound fluid. In non-healing ulcers IL-1a, IL-1β, IL-6 and TNF-α were significantly increased compared with healing ulcers. When growth factors were assessed, there was no statistical difference between healing and non-healing venous ulcers in antigen concentration of the growth factors platelet derived growth factor (PDGF), epidermal growth factor (EGF), basic fibroblast growth factor (bFGF) and TGF-β1.
11
Further analysis of the mitogenic potential of wound fluid collected from healing and nonhealing on 3T3 fibroblast demonstrated that healing wound fluid caused significant increased proliferation, suggesting an improved extracellular environment.
11
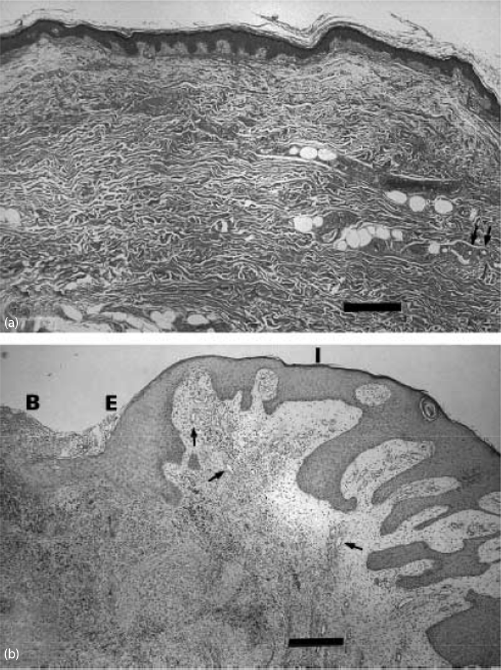
In another study evaluating CVU versus normal control biopsies, growth factors and cytokines in keratinocytes were evaluated by immunohistochemistry There are significant and striking differences in the histology of normal and CVU skin, which may reflect the activity of cytokines (Figure 2). There was increased expression in the keratinocytes of adjacent skin next to the ulcer edge for TNF-α (and its receptors TNF-rI and TNF-rII), IL-1a, IL-6, TGF-β1, PDGF-A, EGF, bFGF and vascular endothelial growth factor (VEGF). The ulcer edge had increased expression of PDGF and VEGF
12
The significance of this study is the presence of upregulated production of cytokines and growth factors in keratinocytes of non-healing CVUs. It is important to note from the latter study that these cytokines and growth factors are all being produced in increased amounts, and the impaired healing in CVU is not due to a failure to stimulate their production. Indeed, when the ulcers begin to heal the production is reduced, indicating that in the absence of active healing continued increased stimulation is occurring. This concept was studied further from biopsies obtained from healthy and ulcerated tissue before and after compression therapy in 30 limbs (29 patients) with CVU using four-layer compression bandaging. The biopsies were on the ulcer edge taken at zero and four weeks. Pro-inflammatory cytokine protein levels (TNF, IL, interferon-γ [IFN-γ]) were elevated in ulcer tissue compared with healthy tissue, but compression therapy significantly reduced these cytokines and had an increase in TGF-β1, after compression. Evaluation of healed versus non-healed CVU, defined as a greater than 40% reduction in ulcer surface area at four weeks, was assessed. It was found that increased levels of inflammatory cytokines are necessary prior to compression but rapidly decrease in healing venous ulcer, and the anti-inflammatory cytokine interleukin-1 receptor antagonist (IL-1 Ra, anti-inflammatory cytokine) increase is necessary after compression (Table 1). In addition, IFN-γ decrease is critical for healing to occur following compression.
13
Histological examination of tissue biopsies. In normal skin (a) there is epidermis, dermis and hypodermis, with the arrows pointing to a sweat gland. In ulcerated skin (b) there is the ulcer base (B), ulcer edge (E) and intact skin (I). Note hyperproliferative keratinocytes at E, elongation of the rete ridges at I, and increased thickness of the papillary layer of the dermis with a perivascular inflammatory infiltrate, and an increased number of small blood vessels (arrows)
12
Cytokines displaying significantly different protein levels in rapid (healed >40%) compared with delayed (healed <40%) healers (pg/μg protein)
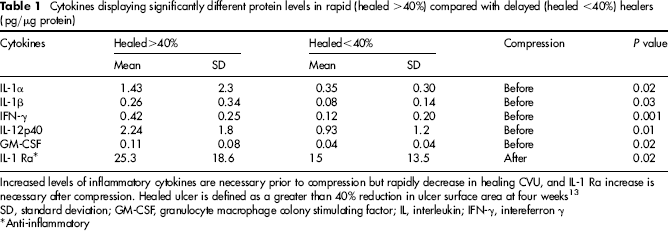
Increased levels of inflammatory cytokines are necessary prior to compression but rapidly decrease in healing CVU, and IL-1 Ra increase is necessary after compression. Healed ulcer is defined as a greater than 40% reduction in ulcer surface area at four weeks SD, standard deviation; GM-CSF, granulocyte macrophage colony stimulating factor; IL, interleukin; IFN-γ, intereferron γ
Anti-inflammatory
The role of TGF-β1 in venous ulcer healing was investigated in a study comprising 80 patients treated with multilayer compression bandaging. In the wound fluid and venous blood, cytokines reflecting inflammation (IL-1β, TNF-α), proteolysis (MMP-2 and MMP-9), angiogenesis (bFGF, VEGF) and matrix deposition/proliferation/fibrosis (TGF-β1) were measured at zero and five weeks postcompression. Although there was a significant positive correlation between ulcer size and initial concentration of wound fluid bFGF (larger CVU had increased levels of bFGF), ulcer healing only correlated with increased concentrations of TGF-β1 in the venous ulcer wound fluid, indicating the multiple roles of TGF-β1 involved in fibrogenesis, matrix deposition and proliferation (Table 2). 14
Relationship between changes in wound cytokines and ulcer healing from zero to five weeks

Increasing concentration of TGF-β1 was the only significant cytokine that correlated with venous ulcer healing 14
MMP, matrix metalloproteinase; VEGF, vascular endothelial growth factor; TNF-α, tumour necrosis factor-α; TGF-β1, transforming growth factor-β1; bFGF; basic fibroblast growth factor; IL, interleukin
Spearman rank test
MMPs and the role of inflammation in CVUs
The inflammatory process in CVUs involves MMPs, which are important biomolecules in the extracellular matrix (ECM) degradation processes. MMPs have been demonstrated to be critical in CVU pathophysiology, and likely represent an activated pathway in response to various cytokine and signaling pathways initiated by leukocytes. Cytokines such as IL and TNF are known to activate MMPs in endothelial and fibroblast cells in vitro. 10 In a study of acute wound fluid it was found that it contained markedly increased levels (5- to 10-fold) of gelatinases MMP-2 and MMP-9 compared with serum, consistent with acute inflammatory response during wounding. However, in chronic leg ulcers the wound fluid levels and activity of MMP-2 (3–5 × higher versus acute MWF) and MMP-9 (5–20 × higher versus acute MWF) were increased significantly over acute wound fluid, and demonstrated the presence of both activated enzyme and proenzyme species, suggesting that non-healing ulcers develop an environment containing high levels of activated MMPs, which may result in failed wound closure. 15 Other studies investigating CVU wound fluid compared with acute wounds determined that there is elevated MMP-2 and MMP-9 activity. In addition, there was increased degradation of the growth factor EGF in CVU fluid, but as the CVU healed there was a reciprocal decrease in gelatinases activity. The study supported the notion that proteinase inhibition may be a possible means to treat chronic wounds and CVUs. 10 Analysis of CVU exudates also revealed elevated collagenase and gelatinase activity compared with acute wound fluid. Furthermore, the CVU gelatinase profiles were characterized by high expression of 92/82 (MMP-9) and 72/62-kDa (MMP-2) duplex bands and by the presence of low molecular mass activation products. 16 These data further supported the presence of MMPs in CVU wound fluid leading to a chronic state of inflammation, tissue turnover and persistent chronic wound.
Inhibitors of metalloproteinases (TIMP) also play a crucial role in the remodeling process of venous ulceration. A sudden disruption of the balance between proteinase activity and inhibitor level may deteriorate wound healing. In comparison to acute wounds, non-healing venous ulcers contain high levels of activated gelatinases and low levels of tissue inhibitor of metalloproteinase-1 (TIMP-1). LDS skin is often associated with active or healed ulcers, or is a significant precursor to ulcer formation. In a study comparing skin biopsies from LDS and normal skin, the mRNA and protein expression of MMP-1, MMP-2 and TIMP-1 were significantly increased in LDS, whereas the total amount of MMP-9 and TIMP-2 mRNA and protein was not altered. 17 In addition, there was significantly increased MMP-2 proteolytic activity in LDS versus controls, and elevated collagen type I and type IV degradation by MMP-2 indicating functional activity by MMP-2. 17 Increased diffuse staining was found for MMP-1 in the epidermis and dermis in comparison with controls. In LDS, MMP-2 was predominantly localized in the basal and suprabasal layers of the epidermis, in perivascular regions and the reticular dermis. 17
Activation of recombinant MMP-2 is controlled by the activity of the urokinase-type plasminogen activator (uPA), which acts as a fibrin-independent plasminogen to form plasmin which activates pro-enzymes of MMPs. The activity of MMP-2 is potentiated by binding of uPA to the uPA receptor (uPAR). Elevated expression of uPA and uPAR at the mRNA and protein levels in CVUs, in comparison with healthy skin was demonstrated. Histological analysis, uPA and uPAR were located in the capillary and dermis. Fibrin zymography showed significantly elevated endogenous uPA activity in CVUs in comparison with healthy controls. 18 These findings indicated that venous leg ulcers are characterized by elevated uPA activation, suggesting that the uPA:uPAR cascade plays a crucial part in maintaining proteolytic activity in CVUs.
Two important molecules in the activation of MMPs are membrane type 1 MMP (MT1-MMP) and the extracellular MMP inducer EMMPRIN (CD147).
By a immunohistochemistry assay, MMP-2, MT1-MMP, MT2-MMP and EMMPRIN were significantly elevated in venous ulcer dermis compared with control dermis, and EMMPRIN and MMP-2 were overexpressed in the perivascular regions (Table 3). 19 These data indicate the presence of MMP activators that favours ECM turnover and unrestrained MMP activation in CVUs.
Immunohistochemistry of chronic venous ulcer (CVU) versus normal tissue (Nl)
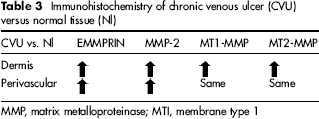
MMP, matrix metalloproteinase; MTI, membrane type 1
To summarize the role of MMPs in CVUs, there is evidence that suggests the essential role for MMPs in linking ulceration and repair. In particular, there is a significantly higher MMP activity in wound fluid and tissue of CVU and LDS. Binding of uPA to uPAR potentiates the activity of MMPs. EMMPRIN also regulates MMP induction in the dermis and perivascular regions of CVU. These processes lead to unrestrained MMP activity and the degradation of the provisional matrix, resulting in persistent venous ulcer.
Pro-inflammatory cytokines are considered as potent inducers of MMP expression in chronic wounds, and they have been shown to down-regulate the expression of TIMPs, thus creating an environment with a relative excess of MMP activity.
10
Unrestrained protease activity is one of the major underlying pathological mechanisms of non-healing wounds and leads to degradation of the provisional matrix. Ulcer formation, therefore, may be favoured by enhanced turnover of the ECM mediated by unrestrained activity of specific MMPs. Non-healing CVUs are associated with greater MMP-2 activity. However, PDGF-AA activity instead is associated with ulcer healing, as suggested by an analysis of wound fluid of 40 patients with CVU. In this study, a significant increase of PDGF-AA was noted in the perivascular region on immunohistochemistry, and by enzyme-linked immunosorbent assay of healing ulcers, suggesting that the growth factor PDGF-AA appears to be essential in promoting healing, and an important marker of CVU healing (Figure 3).
20
immunoassay of the wound fluid platelet derived growth factor AA (PDGF-AA) was present at a concentration of 102 SD 16 pg/mL in the healing group in comparison with 88 SD 12 pg/mL in the non-healing group of ulcers. This difference was statistically significant (P<0.021). The presence of PDGF-AA is a marker indicative of chronic venous ulcer healing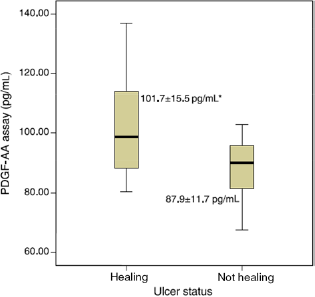
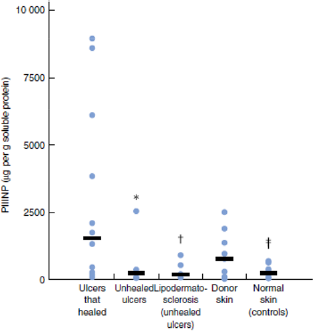
Collagen turnover and MMP activity are also important elements in CVU healing. In a recent study, biopsies were taken from 12 patients whose venous ulcers went on to heal, 15 patients whose ulcers failed to heal despite 12 months of compression bandaging and 15 controls. Collagen III N-terminal propeptide (PIIINP, propeptide extensions at both ends of procollagen III and released during synthesis, deposition and degradation of type III collagen) and degraded collagen (collagen turnover) levels were higher in ulcers that healed compared with ulcers that failed to heal (Figure 4). Collagen type III turnover appears to be an important biological event that is necessary during the healing of CVU. MMP-1 activity was also higher in healing ulcers than resistant ulcers and normal skin. Rapidly healing CVU had increased collagen turnover and MMP-1 activity, which differentiates them from those that failed to heal within 12 months.
21
Comparison of collagen III N-terminal propeptide (PIIINP) levels in tissues from patients with leg ulcers and controls. In chronic venous ulcers that healed there is significant collagen type III turnover. Bars indicate median values. *P = 0.005, †P = 0.018, ‡P = 0.003 versus ulcers that healed
21
Conclusions
The summary of all the potential markers of chronic venous healing described so far is listed in Table 4. Understanding both cellular and biomolecular mechanisms involved in CVD initiation and progression will allow us to identify new targets for possible future pharmacological intervention, which are mainly related to the cellular and biomolecular aspects of disease. 1 A proactive approach to the treatment of the early and late stages of CVD may be focused on inflammation-related and MMP-dependent proteolysis. In fact, actually the inhibition of MMPs may represent a realistic, novel and possibly therapeutic intervention to limit progression of leg ulceration.
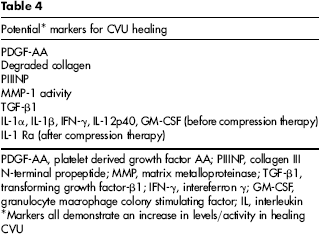
PDGF-AA, platelet derived growth factor AA; PIIINP, collagen III N-terminal propeptide; MMP, matrix metalloproteinase; TGF-β1, transforming growth factor-β1; IFN-γ, intereferron γ; GM-CSF, granulocyte macrophage colony stimulating factor; IL, interleukin
Markers all demonstrate an increase in levels/activity in healing CVU
Funding
This research received no specific grant from any funding agency in the public, commercial, or not for-profit sectors.
Footnotes
The authors have no conflicts of interest to declare.