
Abstract
Objective
The aim of this study was to investigate a possible relationship between obesity and decreased mobility of the talocrural joint and in turn chronic venous disease.
Subjects and methods
One hundred obese patients recruited at Hospital Santa Casa de Maringa, Parana were enrolled by order of arrival at the hospital in a randomized quantitative cross-sectional study. Inclusion criteria were patients with a body mass index above 30 kg/m2 and the exclusion criteria were infectious conditions that would interfere with the assessment. Patients were graded according to the clinical, etiological, anatomical and pathophysiological classification. Talocrural goniometry was performed to assess the degree of mobility of the legs. The Kolmogorov–Smirnov normality test, Kruskal–Wallis test, Dunn's Multiple comparison test and analysis of variance were used for statistical analysis tests with an alpha error of 5% being considered acceptable.
Results
The increase in body mass index is correlated to the reduction in joint mobility (Kruskal–Wallis test: p-value <0.0001) and increase in clinical, etiological, anatomical and pathophysiological classification is correlated to a decrease in joint mobility and the increase in age is associated with an increase in clinical, etiological, anatomical and pathophysiological classification (Kruskal–Wallis test: p-value <0.0001).
Conclusion
Obesity is associated with deterioration in joint mobility and worsening of chronic venous disease.
Introduction
Studies show that venous disease is more clinically severe in obese limbs and the venous reflux is worse. However, measurements of muscle pump function are better including the residual volumes and fractions, ambulatory venous pressure, venous filling index and the ejection volume. The foot venous pressure was significantly greater in the obese in all positions. 1
Another study shows that in about half of patients with unilateral varicosities, chronic venous disease (CVD) developed in the contralateral, initially asymptomatic, limb in five years. CVD progression consists in the development of reflux and clinical deterioration of the affected limbs. Obesity, orthostatism, and noncompliance with compression therapy are independent risk factors for CVD progression. 2
There appears to be a relationship between obesity, CVD and popliteal venous compression. Popliteal vein compression syndrome may clarify the previously unexplained venous presentations. Surgical decompression provides good results in patients unresponsive to conservative treatment. 3
Bilateral clinical manifestations of CVD are twice as common in the obese subset compared with the non-obese with the incidence increasing with body mass index (BMI). Resting and exercise femoral vein pressures were similar to the non-obese. Raju et al. 4 reported that compression by increased intra-abdominal pressure associated with obesity is the likely mechanism of obstruction in 11% of limbs. Additionally, increasing the clinical, etiological, anatomical and pathophysiological (CEAP) classification is correlated with an increased mean BMI. 5
The association of BMI with clinical severity independent of reflux measurements indicates that the effect of overweight may involve a mechanism separate from local effects on venous flow. Overweight appears to be a separate risk factor for increased severity of skin changes in patients with CVD. 6 The aim of this study was to investigate a possible relationship between obesity and decreased mobility of the talocrural joint and in turn CVD.
Method
One hundred obese patients recruited at Hospital Santa Casa de Maringa, Parana were enrolled by order of arrival at the hospital in a randomized quantitative cross-sectional study.
Inclusion criteria were patients with a BMI above 30 kg/m2 and the exclusion criteria were infectious conditions that would interfere in the assessment.
Patients were graded according to the CEAP classification: C0 (venous insufficiency – no varicose veins), C1 (telangiectasias – small varicose veins), C2 (varicose veins and edema), C4 (trophic changes), C5 (healed ulcer) and C6 (open sore). Talocrural goniometry was performed to assess the degree of mobility of the legs (range of ankle motion (ROAM)). The Kolmogorov–Smirnov normality test, Kruskal–Wallis test, Dunn's Multiple comparison test and analysis of variance were used for statistical analysis with an alpha error of 5% being considered acceptable.
The study was approved by the Research Ethics Committee of the institution and the Trial was registered – ACTRN12610000761066. (URL: http://www.ANZCTR.org.au/ACTRN12610000761066.aspx).
Results
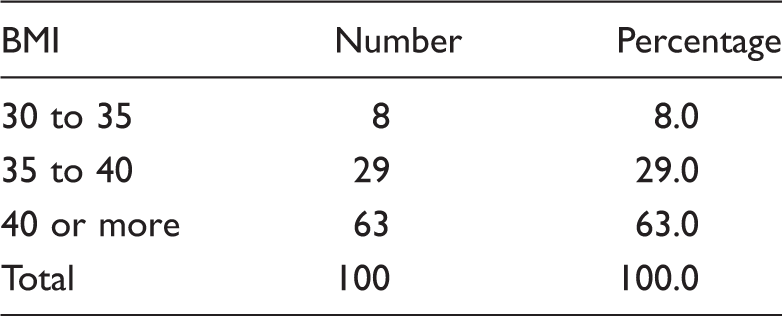
BMI (kg/m2) of patients.
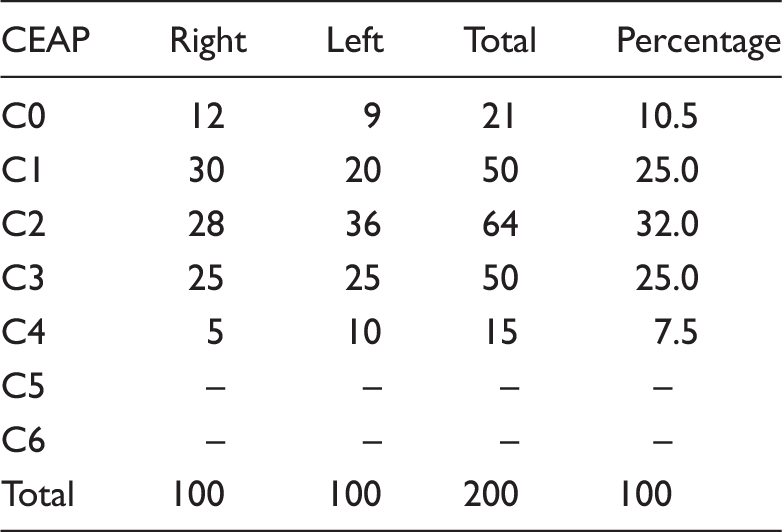
Distribution of CEAP classifications.
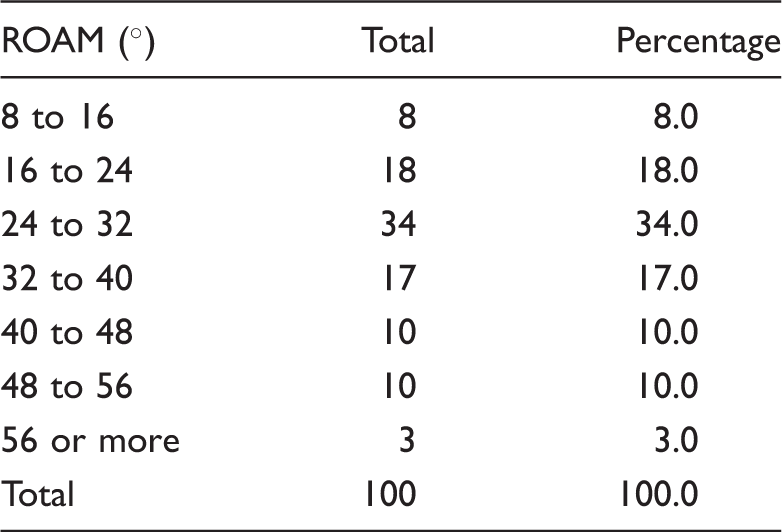
ROAM in degrees of the right leg.
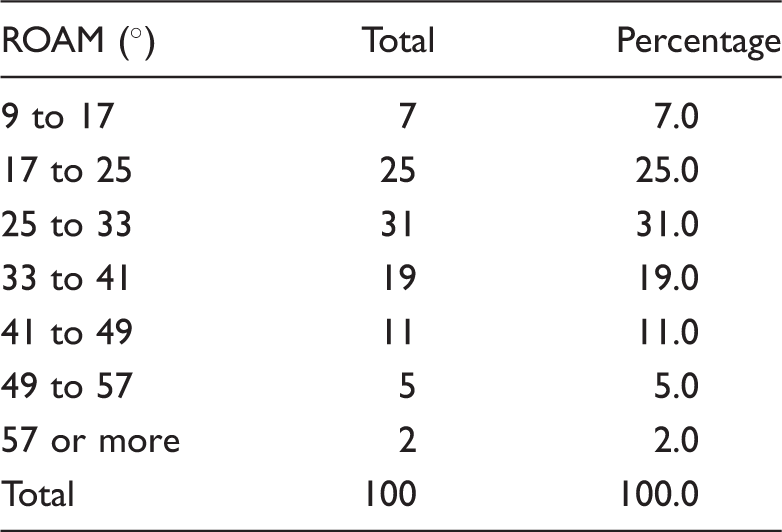
ROAM in degrees of the left leg.
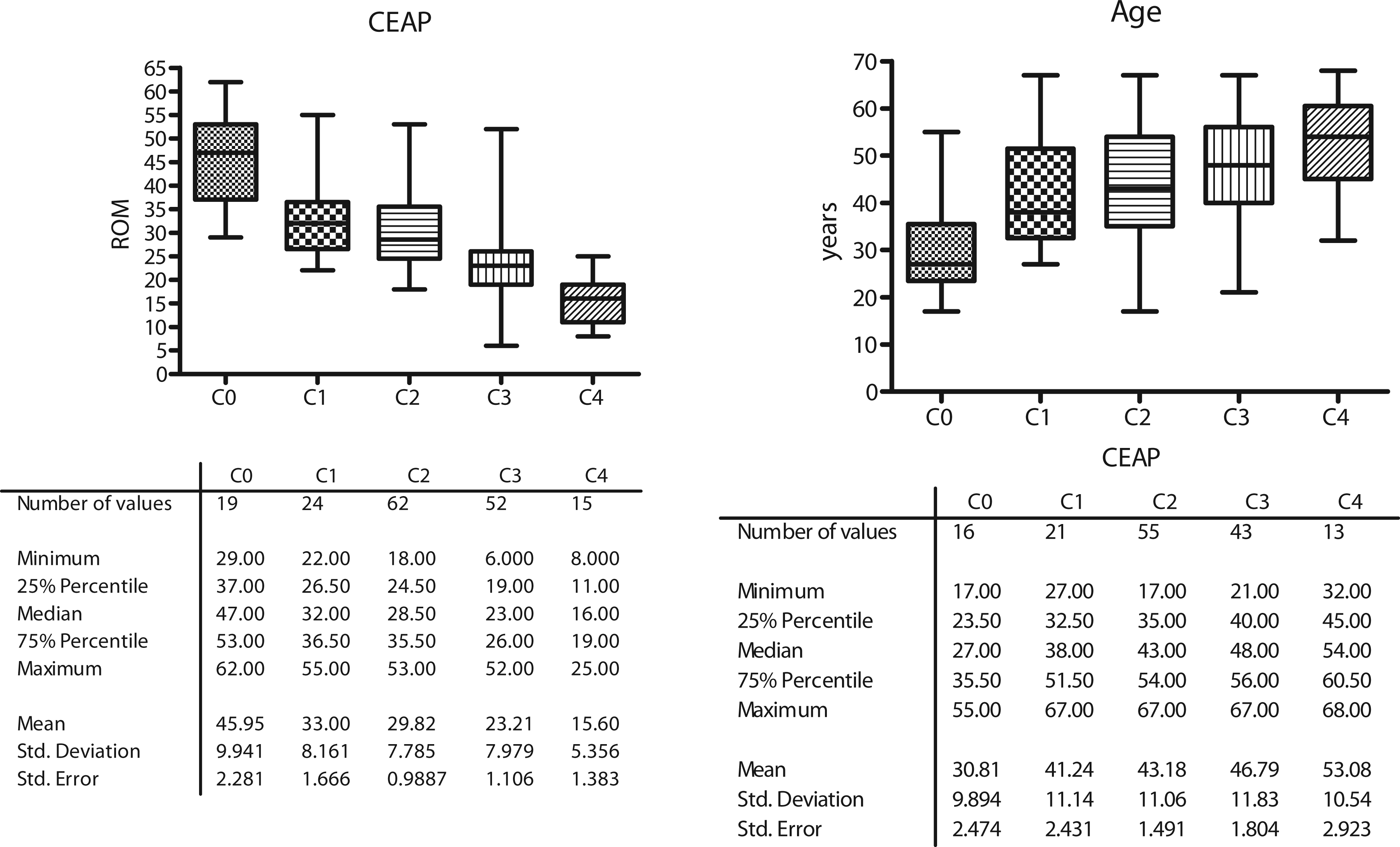
The increase in BMI is correlated to the reduction in joint mobility (Kruskal–Wallis test: p-value <0.0001 – Figure 1). The increase in CEAP is correlated to a decrease in joint mobility and the increase in age is associated with an increase in CEAP (Kruskal–Wallis test: p-value <0.0001 – Figure 2).
The increase in BMI is correlated to the reduction in joint mobility (Kruskal–Wallis test: p-value <0.0001). The increase in CEAP is correlated to a decrease in joint mobility and the increase in age is associated with an increase in CEAP (Kruskal–Wallis test: p-value <0.0001).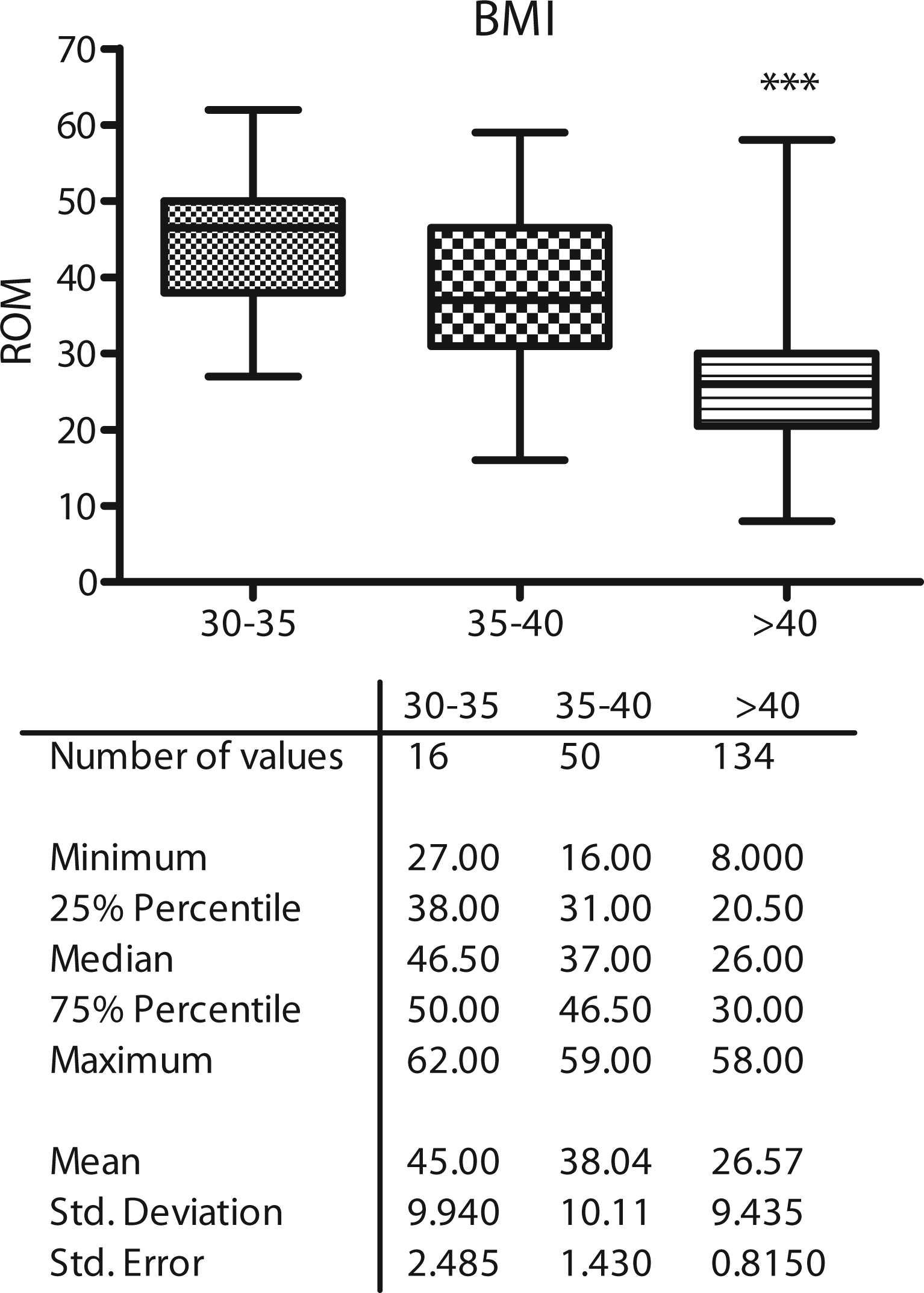
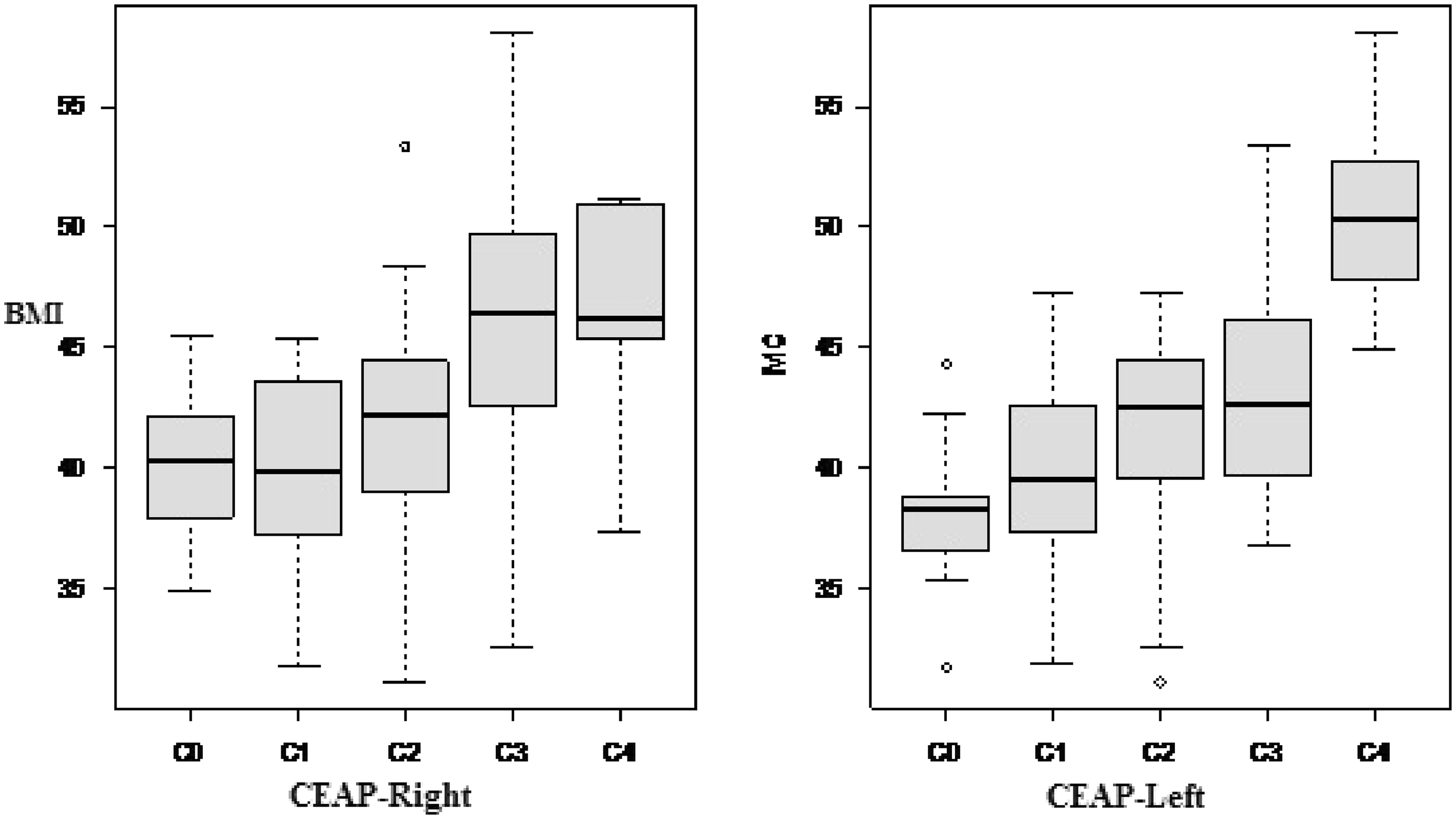
Analysis of variance was used to check whether there are differences in the mean BMIs of patients in respect to the CEAP classification of both legs. This analysis showed that there is a significant difference (p-value <0.001) between the CEAP classifications, that is, the classifications are different between legs.
The Box-plot graph in Figure 3 shows that the CEAP classification increases as the BMI increases and the box-plot graph in Figure 4 shows that the BMI may not correlate to the CEAP classification of both right and left legs.
Box-Plot of BMI according to the CEAP. Box-Plot of BMI according to the CEAP classifications of the right and left legs.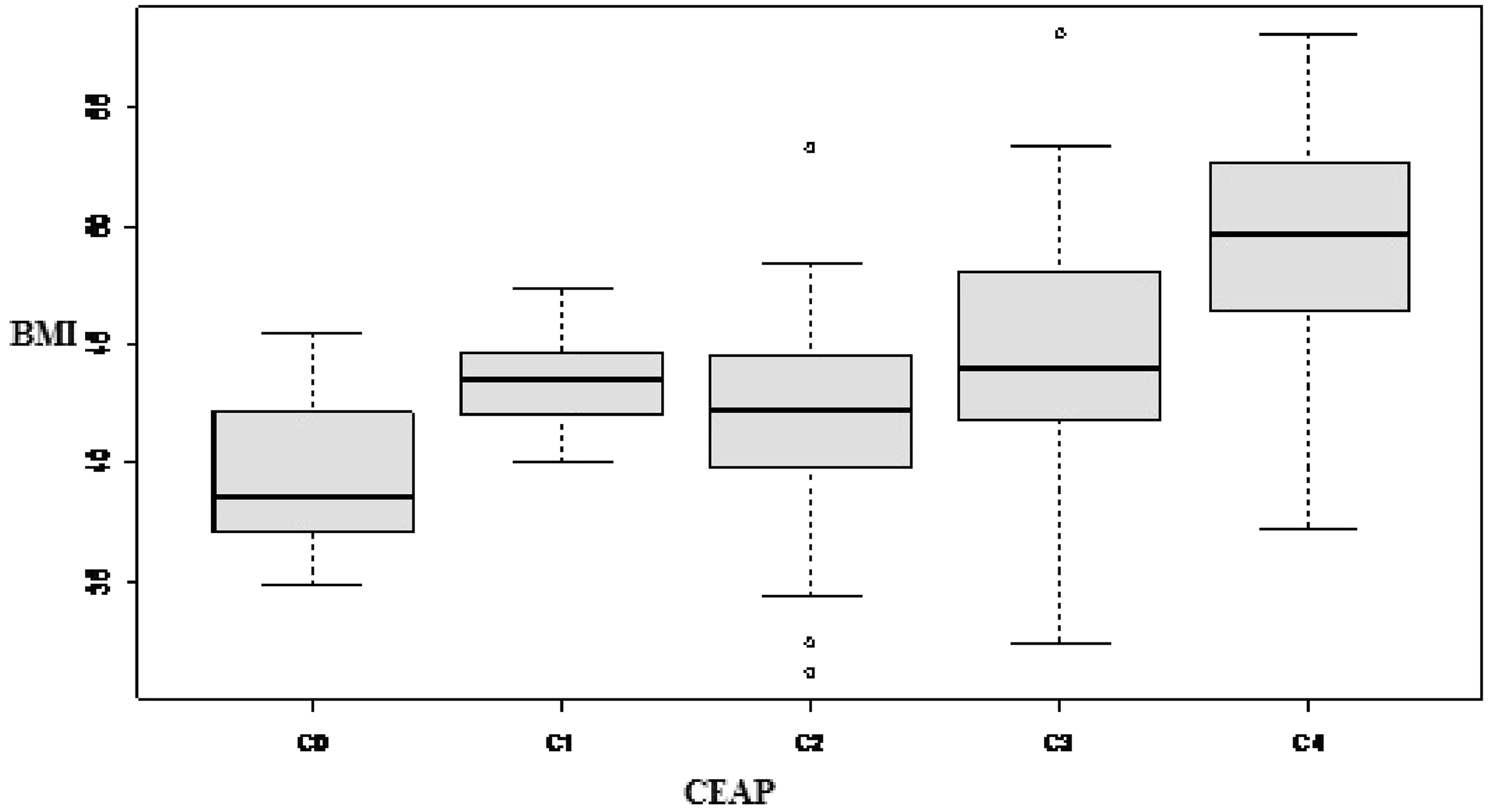
Discussion
This study demonstrates that there is a reduction in joint mobility with increases with BMI and the CEAP classification and an increase in the CEAP classification with increased BMI and age.
Therefore, we suggest that there is an impairment of the suction-impulse pumps in obesity, which is exacerbated with aging and the deterioration of CEAP. We believe the aspiration-impulsion pump is functionally well; however, the increased abdominal pressure in obese patients may compromise its effectiveness. Further studies are necessary to try to test this theory.
The worsening of joint mobility may influence the contractile mechanisms of the suction-impulse pumps, but the study found no impairment in pump function. 1 This may be associated with the degree of impairment of joint mobility. A study evaluating joint mobility and the clinical stages of CEAP identified that in later stages, the C5 and C6 classifications of CEAP, hemodynamic changes occur as can be seen by plethysmography and joint mobility.7,8 In this study, no patients were in these stages, stages in which the talocrural joint mobility could be further undermined.
Among the pathophysiological mechanisms proposed is external compression of both intra-abdominal and popliteal veins.3,4 One study suggests that lower limb venous flow parameters differ significantly between healthy obese and non-obese individuals. These findings support the mechanical role of abdominal adipose tissue potentially leading to elevated risk for both venous thromboembolism and chronic venous insufficiency. 9 The pump is working, but the intra-abdominal resistance may limit its efficacy. Another aggravating factor is standing for long periods and failure to use protective devices such as compression garments. 2
Associations between obesity and erysipelas 10 have been described; this also contributes to aggravating lymphatic system diseases and may worsen fibrosis and the lack of joint mobility.
Studies describe that there are many elements associated to this complex condition of CVD, for example, microvascular dysfunction, calf muscle pump efficiency, dermal inflammation; disordered fibroblast function and matrix production; failure of epithelialization, congenital and acquired thrombophilia, malnutrition, obesity and diet; and bacterial colonization. 11 This association may contribute to aggravate the disease.
None of the currently available treatment modalities is entirely satisfactory and novel therapies based upon a clearer understanding of the disease at the psychological, genetic, mechanical, microvascular and microscopic level are required.
Conclusion
Obesity is associated with deterioration in joint mobility and worsening of CVD.
Footnotes
Acknowledgements
The authors wish to thank Dr. Hugo Partsh for his suggestions in the text and his contribution to the statistical analysis.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not for-profit sectors.
Conflict of interest
None declared.