
Abstract
Objective
To present the use of retrograde mechanico-chemical endovenous ablation for ablating the remaining below-knee great saphenous vein in patients with venous stasis ulcers persisting after above-knee great saphenous vein ablation.
Methods
This small study includes six patients with persistent C6EpAsPr ulcers following above-knee great saphenous vein ablation with no incompetent perforators. They were treated using retrograde mechanico-chemical endovenous ablation approach followed by Unna therapy, followed up on post op days 3 and 30 with ultrasound, and subsequent weekly visits until the wound healed.
Results
Six patients (four men and two women), have average ulcer size of 4.1 cm2. There was no nerve injury or other complications after mechanico-chemical endovenous ablation. These patients had an average of 28 ± 11 days healing time, compared with a mean of five months in traditional method.
Conclusion
Mechanico-chemical endovenous ablation can be safe and effective in the treatment of patients with below-knee great saphenous vein insufficiency with venous ulcers.
Keywords
Introduction
Chronic venous disorders (CVD) can be manifested by a spectrum of signs and symptoms, including edema, pruritus, pain and venous ulcers. Many treatment modalities have recently evolved, ranging from conservative treatment to surgery to endovenous laser ablation (EVLT) or radiofrequency (RF). These are widely accepted treatments for primary CVD. The overwhelming majority of patients experience excellent results soon after the procedure. The three-year success rate for RF is 84% and for laser therapy is 94%. 1 One major complication of thermal ablative procedures is the incidence of nerve injury, which has been reported in approximately 1% of patients. 2 Owing to the proximity at the great saphenous vein (GSV) and the saphenous nerve below the knee, most practitioners do not routinely use thermal energy in this anatomical region. We were interested in using mechanico-chemical endovenous ablation (MOCA) to treat recurrent and persistent venous ulcers in those who had previous successful ablation of the GSV. MOCA is an option for this discrete subset of patients because it eliminates the need of thermal energy thereby minimizing the risk of nerve damage, 3 so it could be safely used below the knee GSV. In our patient population, we treated all the way down to the ulcer at the level of the medial malleolus and had no nerve injury. Initially, the decision to make a venous puncture at the level of the knee and advance the catheter distally was made to make the procedure technically easier as the vein diameter is greater at the knee as opposed to the ankle. It is also easier to perform a successful venous puncture through the supple skin at the knee rather than the chronically inflamed tissue around the ulcers. We were pleasantly surprised how quickly the ulcer healed after using this technique. It was also very easy with the small caliber angle tip to inject sclerosant directly into the venous branches feeding the ulcers.
A few studies have shown the effectiveness and safety of using Clarivein® catheter (Vascular Insights, Madison, Wisc) in the GSV and the small saphenous vein.4,5 This paper presents the feasibility and efficiency of using Clarivein® in treating the GSV below the knee and the branches that directly feed the ulcer.
Method
This small study looks at eight patients with venous ulcers all of whom had C6EpAsPr classification unresolved after RF ablation of the GSV above knee. Patients were seen from January 2011 to December 2012. All had a reflux of GSV below the knee and a diameter greater than or equal to 4 mm.
Venous insufficiency examinations were performed in an IAC accredited laboratory following approved protocols. Evaluations were performed with a duplex ultrasound machine utilizing a 3–8 MHz or 5–14 MHz linear array transducers. Initial examinations for venous reflux were evaluated for deep and superficial venous thrombosis, and deep and superficial venous and perforator reflux. Diameter measurements were obtained for the great and small saphenous and perforator veins. The patients were evaluated in reverse Trendelenburg, standing and sitting positions. Manual distal and proximal compressions were utilized. Diagnostic criteria for venous incompetence was >1 s for deep veins, >0.5 s for superficial veins and >0.35 s for perforating veins. None of patients in this study had any incompetent perforating veins.
MOCA was used to treat the distal portion of the GSV in these patients. Two patients are excluded from this study as they are on high-dose chronic prednisone for their rheumatologic diagnoses, which delayed the healing process. The results of the remaining six patients are the basis for this paper.
A veni-puncture was performed at the level of the knee and the catheter was advanced distally to the vein directly below the ulcer. As the distal tip is angled, sclerosant was injected directly into the veins which fed the ulcers. If the branches were too small to allow the wire to rotate, sclerosant was injected and the wire was pulled back until the vein diameter would allow rotation. The remaining below-knee great saphenous vein (BK-GSV) was treated with MOCA from the ankle to the knee. A single layer ace wrap was applied.
Patients were followed up with an ultrasound on post op days 3 and 30. They had a weekly examination until the ulcers healed. If an ulcer recurred, they would have gotten a follow-up ultrasound but no ulcers recurred. Each patient was seen three months after the wound completely healed. Ulcers were measured at every visit. These patients were treated with Unna therapy until the wound healed. Subsequently, these extremities were checked during medical visits.
Results
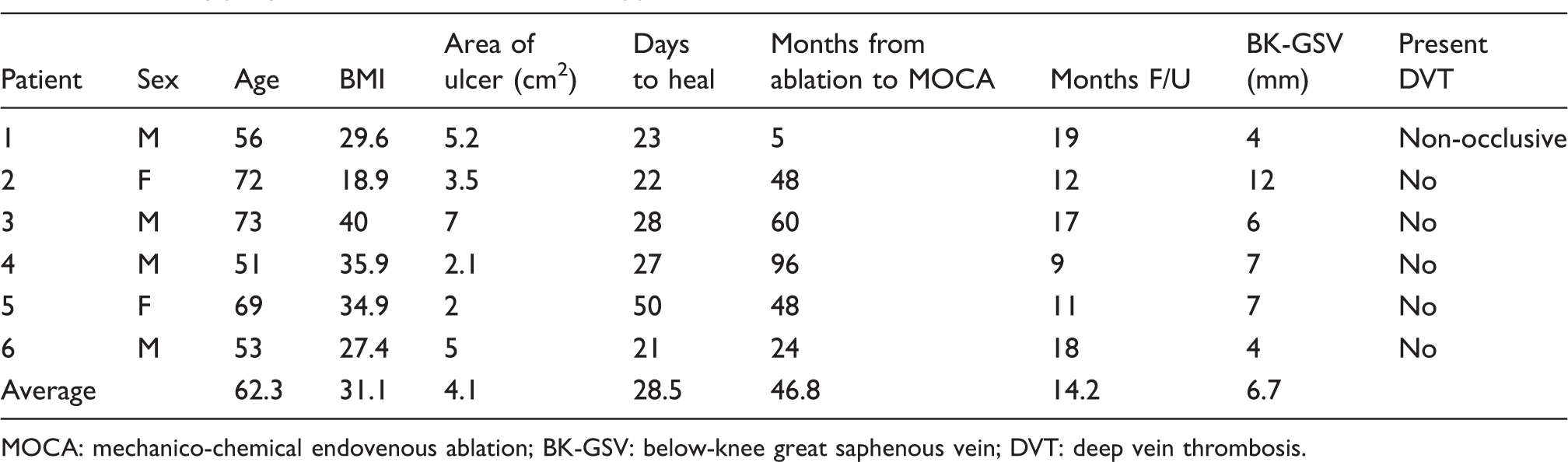
This small study consisted of six patients (four men and two women), average age 62 (51–79) (Table 1). One of these six patients had a non-occlusive deep vein thrombosis (DVT) prior to MOCA therapy. The remaining five had no evidence of DVT on ultrasound. No patient had incompetent perforating veins or posterior arch vein. We only treated the BK-GSV and not the posterior arch vein with the MOCA procedure. All these ulcers had an average area of 4.1 cm2 but they all had persisted for a prolonged period of time despite compression therapy, with average of 46.8 months (from 5 to 96 months) from the time of above-knee great saphenous vein (AK-GSV) ablation to the time of MOCA. In all six cases, the BK-GSV was occluded on follow-up ultrasound. No patient experienced a DVT. These patients healed in 50 days or less, with an average of 28 ± 11 days and the median time was 25 days after being treated with this MOCA technique, compared with a mean time to achieve healing of five months and a median time for healing of nine weeks in traditional method, which includes compression stockings or bandage like the Unna’s boot
6
(Figure 1). With an average follow up of 14 ± 4 months, no ulcers have recurred. All patients have been instructed to wear below-knee support hose (10–20 mmHg) indefinitely. No nerve injury or other complications have been identified with this modified MOCA.
Healing time comparison between retrograde MOCA and compression stockings. Healing progress from modified MOCA approach. MOCA: mechanico-chemical endovenous ablation; BK-GSV: below-knee great saphenous vein; DVT: deep vein thrombosis.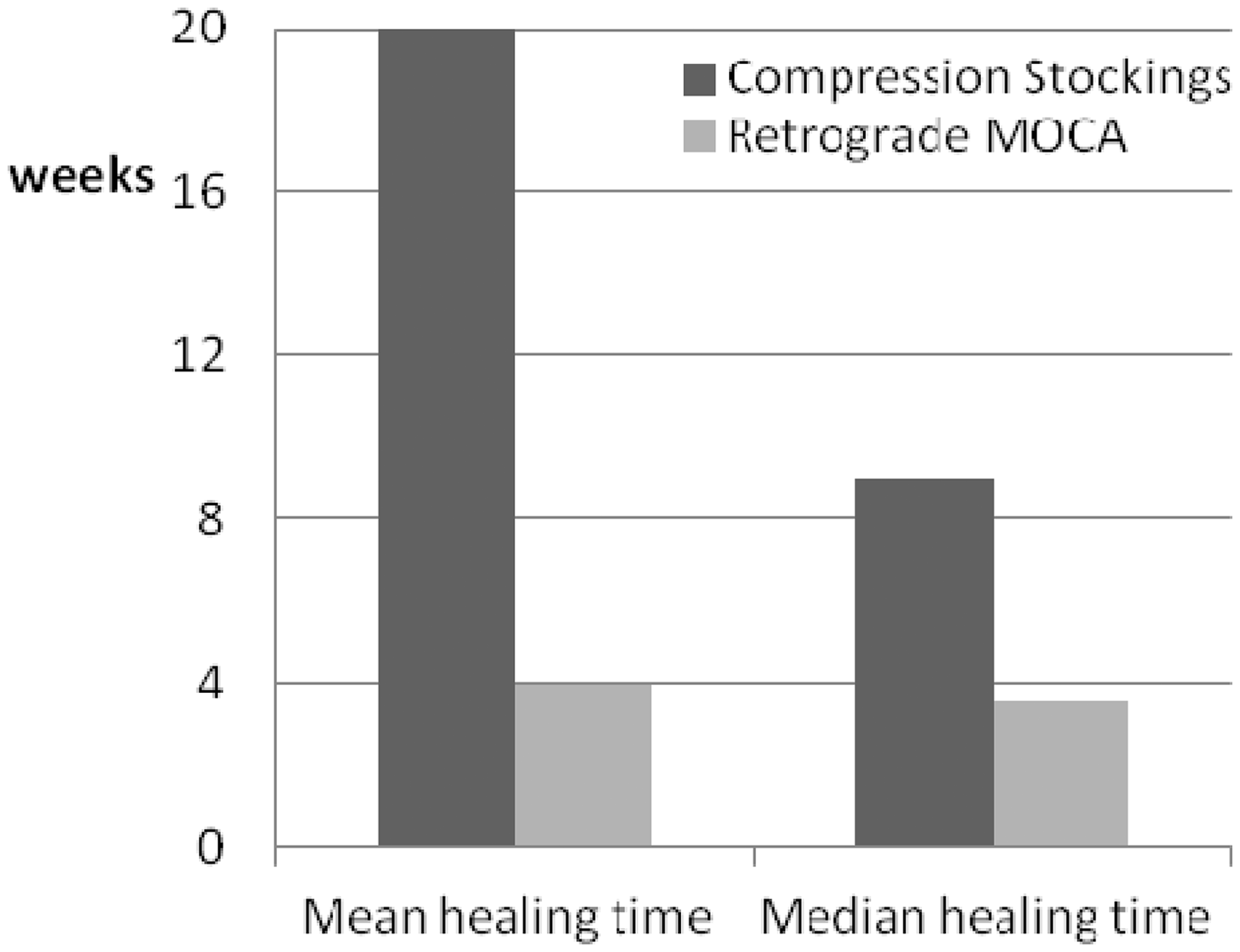
Two patients on high-dose steroid did not benefit from this procedure. They both had persistent venous ulcers 13 months later despite aggressive treatment with compression, repeat debridement and artificial skin substitutes.
Discussion
Our small number of patients had previous successful RF ablation of the GSV above the knee but still experienced persistent venous stasis ulcers secondary to a patent GSV below the knee. It was impressive how quickly these ulcers healed after the GSV was obliterated below the knee.
MOCA has recently shown significantly less postoperative pain, faster recovery and earlier work resumption compared with RFA in the treatment of GSV incompetence. 7 MOCA has another unique advantage in that a venous puncture can be performed at the level of the knee and the catheter can be advanced distally to the tissue, directly below the ulcer. As the distal tip is angled, sclerosant can be injected directly into the veins which feed the ulcer.
The venous puncture at the knee and not the ankle is chosen to make the procedure easier. Also, a venous puncture at the knee avoided going through the desmoplastic reaction of the ulcer and surrounding tissue. Surprisingly, this technique appeared to expedite wound healing.
Carandina 8 has previously utilized CHIVA (Ambulatory Conservative Haemodynamic Management of Varicose Veins) to preserve normally functional segments of GSV while stripping areas of reflux. He selectively identified and preserved non-refluxing varicose veins. As a corollary, we selectively obliterated all refluxing segments contributing to the venous ulcers. By closing branches that fed directly to the ulcers, we appeared to expedite wound healing in comparison to historical control.
Conclusions
Treatment of venous ulcers is an exciting and rapidly expanding field. In the last 15 years, a variety of new innovations have evolved. Each treatment option has its own specific benefits. Practitioners have been reluctant to utilize EVLT and RFA below the knee due to concern of possible nerve injury. The use of MOCA below the knee avoids this particular concern. The result of this study indicates that by selectively treating these pathologic veins or its branches may actually expedite wound healing. Our findings contradict the accepted results from the ESCHAR study, 9 which indicates that surgical intervention does not affect ulcer healing rates but only reduce the recurrent rate compared with solely compression therapy. Some clinicians have anecdotally noted that some venous ulcers do heal more quickly after treatment. This paper attempts to identify that subset of patients.
Retrograde below knee MOCA treating from the knee down to the ankle is the opposite way that this treatment is routinely done. However, if subsequent larger studies confirm our results, this will prove to be one more weapon in our armamentarium to combat venous ulcers.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.