
Abstract
Objective
We report a case of advanced follicular thyroid cancer with innominate vein involvement. To our knowledge, this seems to be the first case treated in emergency surgery, reported in literature.
Method
A 59-year-old woman with a five-year history of a large and mainly right-sided cervical mass presented with dyspnea, unilateral arm swelling, facial flushing, and venous congestion. An emergency computed tomography scan revealed a thyroid mass extending into the upper mediastinum with displacement and compression of the right jugular vein and carotid artery and apparent adherence to the superior vena cava and left innominate vein.
Results
An emergency total thyroidectomy was performed by means of a sternotomy. The lower portion of the retrosternal goiter projected directly into the left innominate vein, with tumor floating in its lumen. Removal of the neoplastic thrombus was performed, through an incision in the vein, en bloc with the thyroid mass. Both goiter and thrombus were completely replaced by follicular carcinoma.
Conclusions
Accurate preoperative assessment through contrast-enhanced computed tomography is strongly suggested in the presence of enlarged thyroid gland extending into the mediastinum whenever angioinvasion is suspected. This could prevent blinded maneuvers such as digital externalization of the thoracic component of the gland, which can be fatal in cases of cervico-mediastinal goiter extending into great cervical or mediastinal veins.
Introduction
Macroscopic angioinvasion from follicular thyroid carcinoma is rare and usually leads to a poor outcome. 1 Thompson was the first to describe a successful thrombectomy of an extended tumor thrombus in the mediastinal great veins from follicular thyroid carcinoma.
We report a case of follicular thyroid carcinoma with extensive mediastinal invasion into the left brachiocephalic vein, treated in emergency setting.
Case report
A 59-year-old woman with a five-year history of a large and mainly right-sided cervical mass was referred to our Academic Institution with worsening dyspnea, unilateral arm swelling, facial flushing, and venous congestion. An emergency contrast-enhanced computed tomography (CT) scan revealed a grossly enlarged thyroid mass extending into the upper mediastinum with complete obstruction of the tracheal lumen, displacement and compression of the right jugular vein and carotid artery and apparent adherence to the superior vena cava and left innominate vein (Figure 1).
Contrast-enhanced CT scan: a grossly enlarged thyroid mass extending into the upper mediastinum with complete obstruction of the tracheal lumen, displacement and compression of the right jugular vein and carotid artery and apparent adherence to the superior vena cava and left innominate vein.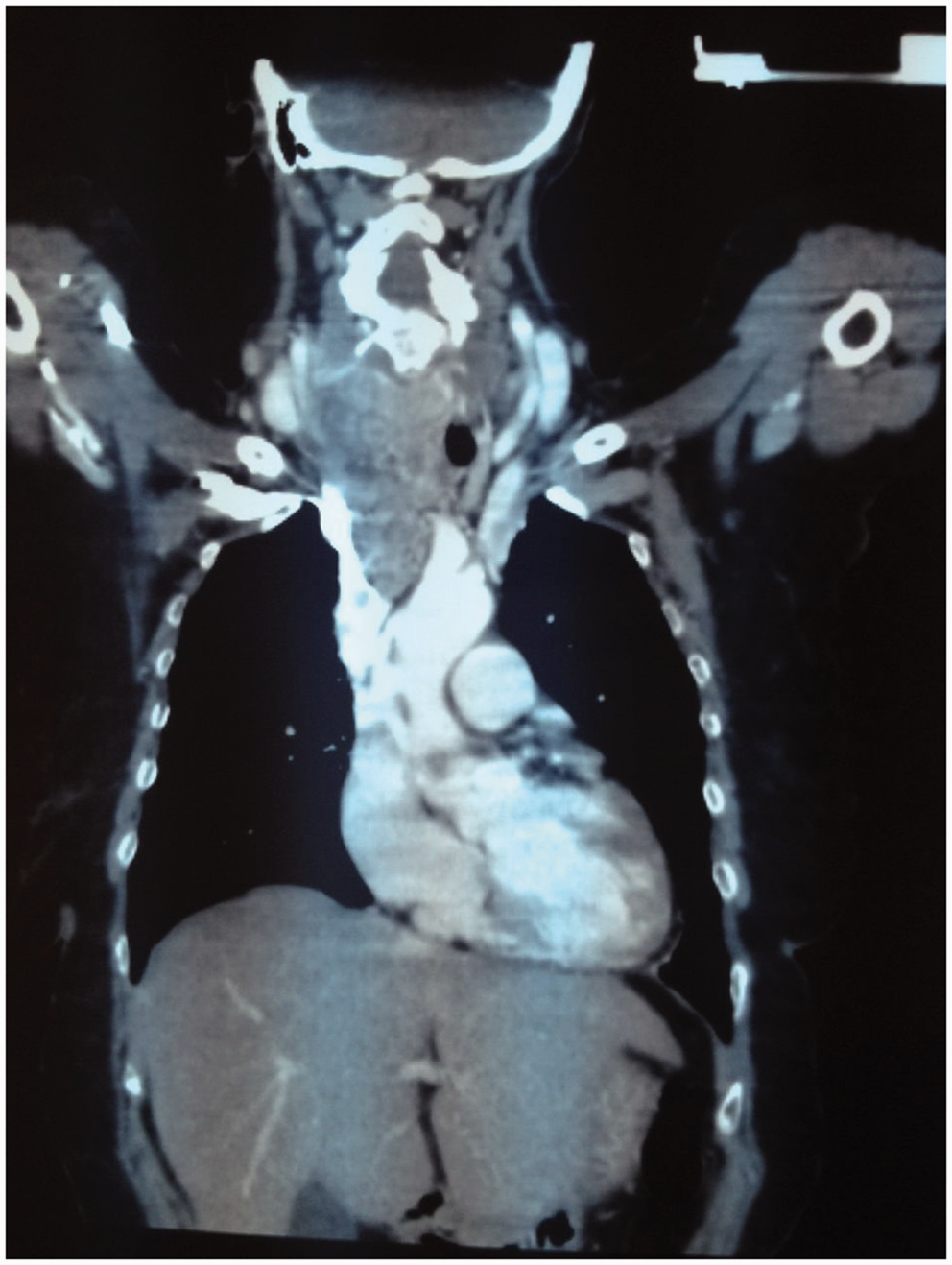
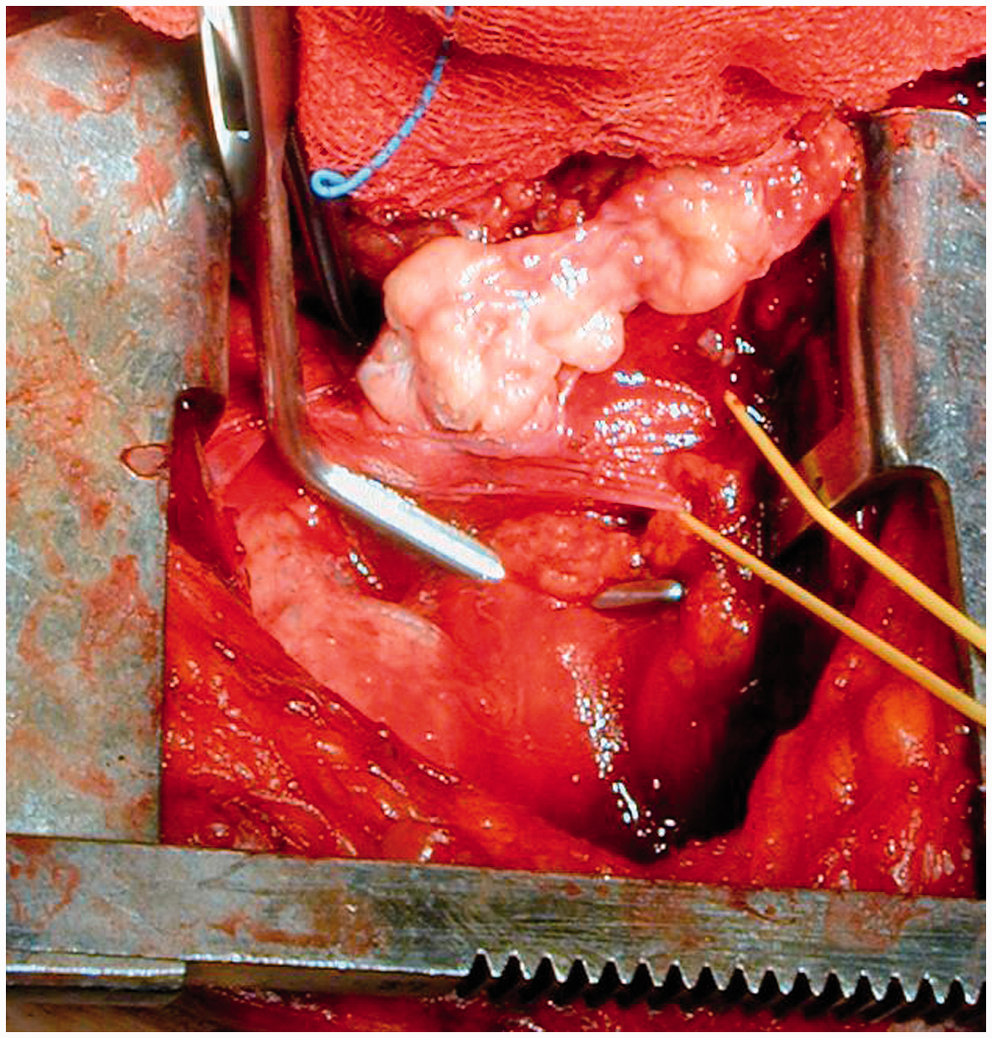
An emergency total thyroidectomy and a prophylactic lymph node dissection of the central compartment were performed by means of a sternotomy, preserving the parathyroid glands and the recurrent laryngeal nerves on both sides, also using 3 × magnification loupe. The tumor mass extended directly into the left innominate vein (Figure 2), with a thrombus arising from the lower portion of the retrosternal goiter, projecting into the vein and floating in its lumen (Figure 3). The vein was clamped at both proximal and distal sites, and an elliptical excision was performed on the anterior wall. The extended tumor thrombus was successfully removed en bloc with the thyroid mass achieving complete primary tumor resection. The left brachiocephalic vein was repaired with 5-0 polypropylene suture. The post-operative course was uneventful and the patient was discharged without complications.
The tumor mass extended directly into the left innominate vein. The tumor thrombus projected into the left innominate vein, floating in its lumen.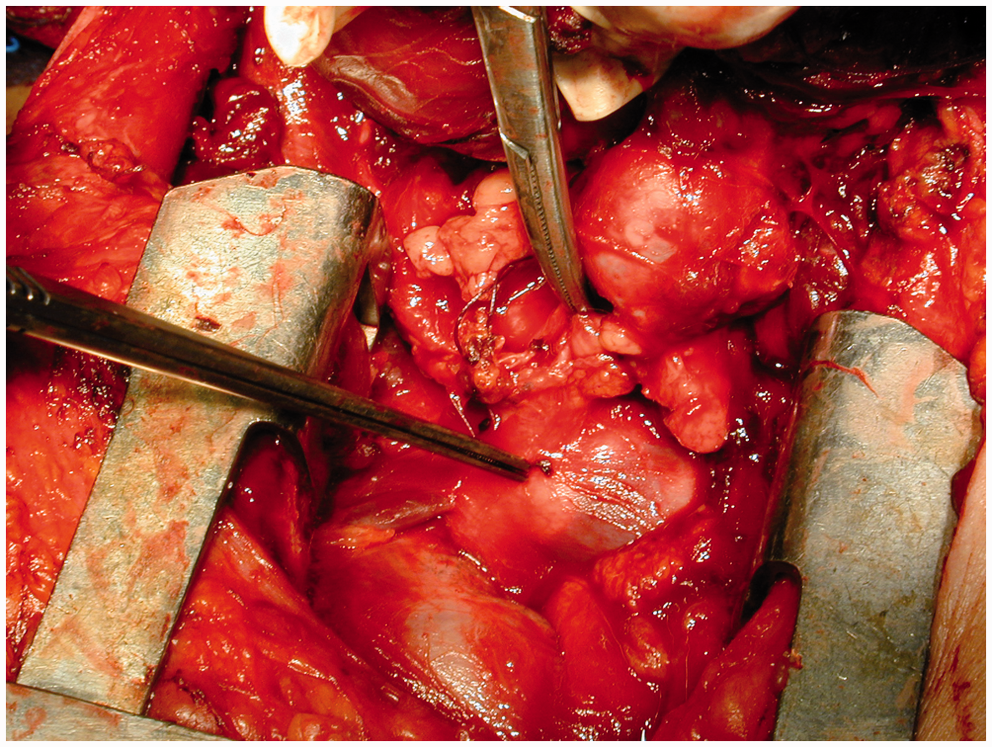
A histological examination later revealed that both the goiter and thrombus were completely replaced by follicular carcinoma. The patient received 131I radioisotope and external radiation beam therapy (ERBT) and died five years later due to the progression of the metastatic disease.
Discussion
Vascular invasion is more frequently associated with follicular thyroid carcinoma. Even though the microscopic vascular invasion is well recognized in follicular thyroid cancer, the macroscopic one is a less recognized cause of morbidity and mortality. 2
The management of these patients is challenging as they typically present with an advanced and rapidly progressive disease.
Reported cases of thyroid carcinoma with tumor thrombus in the mediastinum great veins.
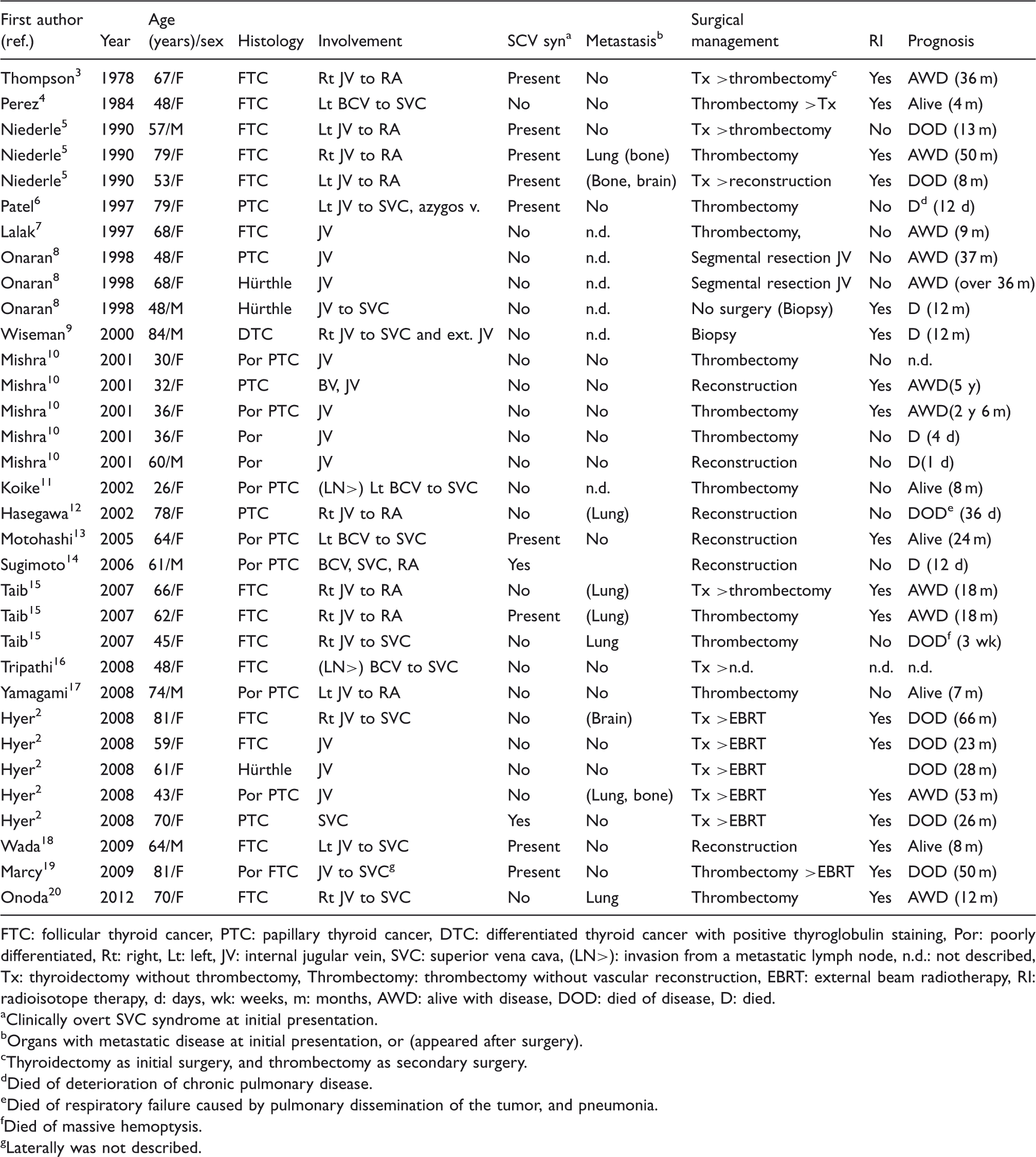
FTC: follicular thyroid cancer, PTC: papillary thyroid cancer, DTC: differentiated thyroid cancer with positive thyroglobulin staining, Por: poorly differentiated, Rt: right, Lt: left, JV: internal jugular vein, SVC: superior vena cava, (LN>): invasion from a metastatic lymph node, n.d.: not described, Tx: thyroidectomy without thrombectomy, Thrombectomy: thrombectomy without vascular reconstruction, EBRT: external beam radiotherapy, RI: radioisotope therapy, d: days, wk: weeks, m: months, AWD: alive with disease, DOD: died of disease, D: died.
Clinically overt SVC syndrome at initial presentation.
Organs with metastatic disease at initial presentation, or (appeared after surgery).
Thyroidectomy as initial surgery, and thrombectomy as secondary surgery.
Died of deterioration of chronic pulmonary disease.
Died of respiratory failure caused by pulmonary dissemination of the tumor, and pneumonia.
Died of massive hemoptysis.
Laterally was not described.
Intrathoracic extension of thyroid tumors should raise suspicion of great vessels involvement and alert the surgeon to the possibility that a sternotomy or cardiopulmonary by-pass may be required.
Depending on the site and degree of the vascular obstruction, the patient may exhibit different clinical manifestations ranging from slight occlusion symptoms to superior vena cava syndrome. But, sometimes the evidence of a venous obstruction may not present itself until the patient undergoes imaging assessment or surgical procedures. 2
Since the clinical presentation may be vague or misleading, appropriate preoperative vascular imaging is mandatory whenever angioinvasion is suspected in order to prevent potential lethal complications such as pulmonary embolism or intracranial/intracardiac propagation of the thrombus. 19
An enhanced CT scan can be useful in the diagnosis of great vein thrombosis and the typical findings include: a smooth defect, external compression, a distended vein with an enhanced wall, low-attenuation intraluminal filling defects, and adjacent soft tissue swelling. Taib and Hisham 15 described the importance of the “ring sign,” a rim of contrast around the tumor thrombus on an enhanced CT scan examination which is important in the decision making, indicating whether a thrombectomy is a feasible surgical procedure.
Venous involvement can also be assessed by magnetic resonance imaging and multidetector computed tomography with sagittal, coronal, and 3D vascular reconstructions, which may be helpful to define the localization, extent and nature of the mass, and distinguish between compression and invasion. 19
Thrombectomy and/or resection with reconstruction are the operative procedure of choice. Vascular resection and reconstruction might be chosen in poorly differentiated and papillary thyroid cancers, whereas thrombectomy is often performed for follicular tumors, and is the most effective surgical treatment when it is feasible. 1
Conclusion
We report a case of advanced follicular thyroid cancer with innominate vein involvement. To our knowledge, this seems to be the first case treated in emergency surgery, reported in literature. Accurate preoperative assessment through contrast-enhanced computed tomography is strongly suggested in the presence of enlarged thyroid gland extending into the mediastinum whenever angioinvasion is suspected. This could prevent blinded maneuvers such as digital externalization of the thoracic component of the gland, which can be fatal in cases of cervico-mediastinal goiter extending into great cervical or mediastinal veins. 21
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.