
Abstract
Diagnostic imaging in cerebral venous sinus thrombosis poses difficulties due to the relatively rare incidence of this pathology and its usually inconclusive clinical and radiological symptoms. The preliminary examination is usually performed using computed tomography, whereas magnetic resonance imaging (MRI) provides better visualisation of the lesion. Computed tomography and magnetic resonance imaging angiography enable the characterisation of the blood flow in the pathologically affected vessels in more detail. Familiarity with the anatomic variations of the venous system and with the advantages and limitations of computed tomography/magnetic resonance imaging enables faster diagnosis of the pathology. This is significant for treatment, which, in many cases, can be efficient only if introduced at a sufficiently early stage.
Keywords
Introduction
Cerebral venous sinus thrombosis (CVST) is a relatively rare cause of cerebral stroke. The detection rate of CVST has grown over the recent years, in part due to the increased use of modern imaging techniques. In a recent study of CVST in children, the population incidence was 0.67 cases per 100,000 children per year; incident rates were highest in neonates. 1 In the adult population, the rate is 3–4 cases per 2 million per year. The disease is considered to be an atypical form of cerebral stroke that is more frequent in young adults.2,3
As early as 1856, Virchow’s triad described risk factors of venous thrombosis: an injury of a blood vessel wall, hypercoagulability and stasis of blood flow. CVST occurs following endothelial damage and slowed blood flow, conditions that are associated with accelerated coagulation and increased blood density. The risk factors include the use of oral contraceptives (up to 70% of cases), congenital and acquired coagulation disorders, inflammatory processes in the head and neck, cardiac defects, systemic diseases of the connective tissue, neoplastic processes, injuries, surgical procedures, pregnancy, childbirth, nephrotic syndrome, diarrhoea and other conditions involving dehydration. In children, the most frequent cause of CVST is dehydration and shock. 3
The clinical symptoms of CVST are non-specific and diverse, ranging from subtle to pronounced. Non-characteristic symptoms, such as headache, focal symptoms and consciousness disorders, considerably delay correct diagnosis.
In as many as 40% of cases, the patient displays exclusively non-specific symptoms associated with increased intracranial pressure due to disorders of cerebrospinal fluid absorption. Apart from headache, symptoms include vomiting, blurred vision and papilloedema, with no hydrocephalus detectable by imaging.1,4–6
The diagnosis of thrombosis is based on neuroimaging, although radiological symptoms are often subtle. Computed tomography (CT) does not always detect thrombosis; the false-negative rate can be as high as 40%. Therefore, a more sensitive screening method, CT angiography or magnetic resonance imaging (MRI), is recommended for thrombosis detection. MRI is an especially sensitive test when combined with angiography. In ambiguous cases, digital subtraction angiography (DSA) may be used for diagnosis.
A radiological diagnosis of CVST obliges the clinician to broaden the scope of diagnostic examinations to determine the aetiology of the thrombotic process.
The mortality rate in the first month after the onset of the disease reaches a high of 13%. Recurrences of the thrombotic process in the cerebral venous sinus affect approximately 15% of patients. A frequent complication is a recurrence of intracranial hypertension symptoms and epilepsy. 7 It is believed that in over 80% of cases, the prognosis may be good, with patients suffering no neurological or cognitive deficits. 2 If diagnosed correctly, CVST may be successfully treated; hence, diagnostic imaging plays a paramount role in the therapeutic process.
The aim of this article is to present the problem of CVST and the applicability of CT and MRI examination for detecting this problem in everyday practice.
Anatomy
The venous system displays considerable anatomical variability; therefore, good knowledge of the variations of the cerebral venous sinuses is essential for a correct diagnosis. The venous sinuses constitute the main draining routes for the cerebral veins. The terminology of the superficial cerebral veins carrying blood to the sagittal sinus corresponds to a given area of the brain, for example. the vein of Labbé and the superficial middle cerebral vein (Sylvian vein). The deep system includes the vein of Galen, the basal vein of Rosenthal, and the medullary and subependymal veins, which drain the white matter of the cerebral hemispheres.
The most frequent anatomical variations of the venous system are transverse sinus asymmetry (detected in nearly 50% of patients examined) and hypoplasia or aplasia of a part of or the whole transverse sinus (detected in 20% of patients). Often, a lack of the frontal part of the superior sagittal sinus is detectable in patients.
Apart from anatomical variations of the sinus drain (usually a direct opening of the superior sagittal sinus into the transverse sinus), it is also important to detect arachnoid granulations – anatomical structures that frequently protrude into the sinuses. The most frequent anomalies include persistent falcine vein and lambdoid-torcular inversion (also called a high tentorial insertion) with high location of the sinus confluence. Persistent falcine vein often co-occurs with a malformation of the vein of Galen and high tentorial insertion often co-occurs with Dandy–Walker spectrum anomalies.4,8 It is also essential to pay attention to artefacts that are usually revealed in the time-of-flight (TOF) technique and that result from complex and slow blood flow in the sinuses.
Clinical symptoms suggesting CVST
CVST often manifests with non-specific symptoms, such as headache, consciousness disorders, convulsions, focal deficit symptoms, papilloedema and meningeal signs. In cavernous sinus thrombosis, symptoms may include exophthalmos with eyeball pain on pressure, ophthalmoedema and damage of the optic nerve (II) and oculomotor nerve (III). In superior sagittal sinus thrombosis, spastic paresis of the lower limbs, visual field defects and coma may occur. In transverse sinus thrombosis, the typical symptom is pain behind the auricle. Cerebral cortex sinus and vein thrombosis may produce aphasia, limb paresis or convulsions due to a local brain oedema caused by impaired blood drainage. 5
Radiological diagnostics
CVST usually affects the superior sagittal sinus and the transverse sinus and is less frequent in the deep vein system.4,5
CT without contrast agents is the most frequent examination performed in emergencies for patients with non-specific neurological symptoms. However, CT with contrast media, possibly complemented with CT angiography, is a more sensitive method.
In CT imaging without contrast agents, CVST may be visible in approximately 25% of cases. 4 The radiological symptom is a hyperdense thrombus in a sinus or a vein (Figure 1). The high density is characteristic of the clot for the first week, which later becomes iso- or hypodense. 9 A less frequent complication of thrombosis is subarachnoid bleeding, which may be the first symptom of the disease. 10 In severe cases, intracerebral bleeding occurs, which is diagnosed, along with cerebral oedema, in approximately 40% of patients with CVST. Secondary venous hypertension and ischaemia may generate symptoms, such as oedema, low density of the cerebral tissue or a mass effect, that cause a narrowing of the ventricular system or cerebral sulci or fissures. Because they are normally narrow in young patients in whom thrombosis is more frequent, these fluid spaces pose an additional obstacle to diagnosis for this age group.4,5,9
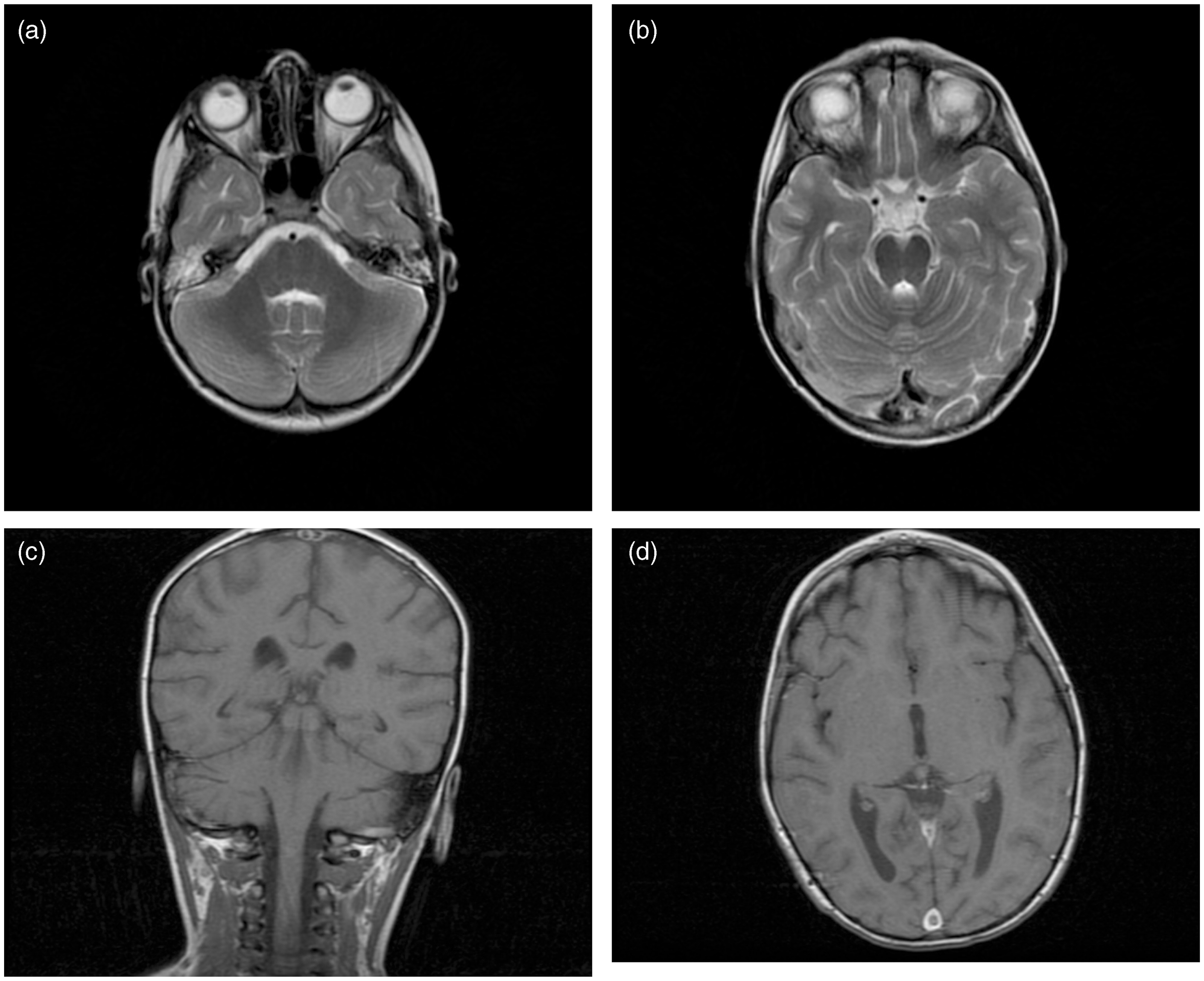
Transverse CT following the administration of a contrast agent may reveal the empty delta sign, that is, a clot in the venous sinus surrounded by blood with the contrast agent (usually displaying a triangular form in cross-section). Lesions of this type may be invisible in the first stage of the disease, but they usually persist for a dozen weeks or longer. 5 Increased hyperaemia of dura mater, falx and tentoriums may be detected by contrast imaging and is manifested by the pronounced intensification of these structures. The cord sign is the counterpart of the empty delta sign in smaller cerebral venous vessels with greater tortuosity. 11
In one-third of the cases examined by CT or contrast CT imaging, thrombosis cannot be diagnosed. CT angiography enables the direct detection of flow disorders in venous sinuses in the form of a defect in the contrast agent filling.
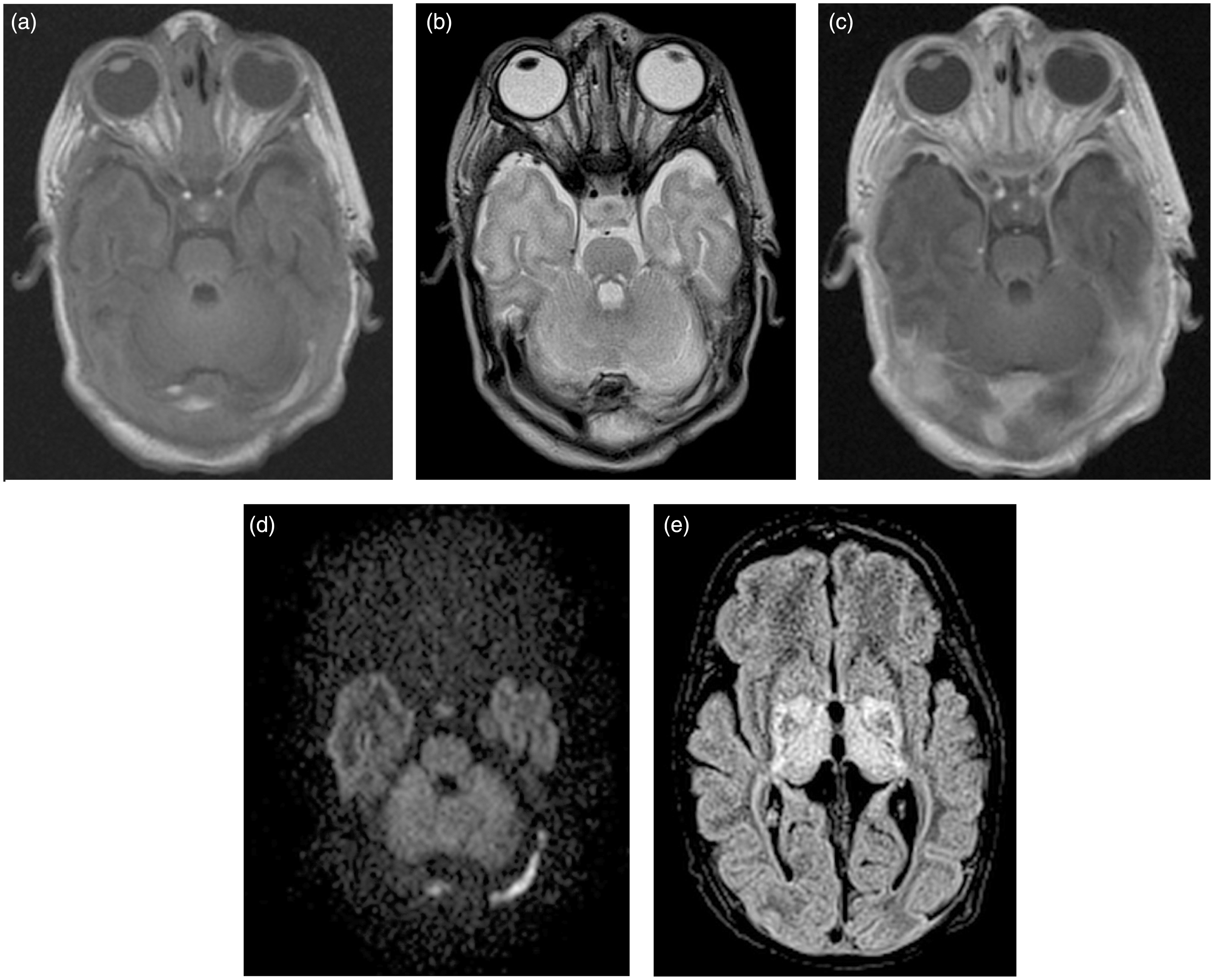
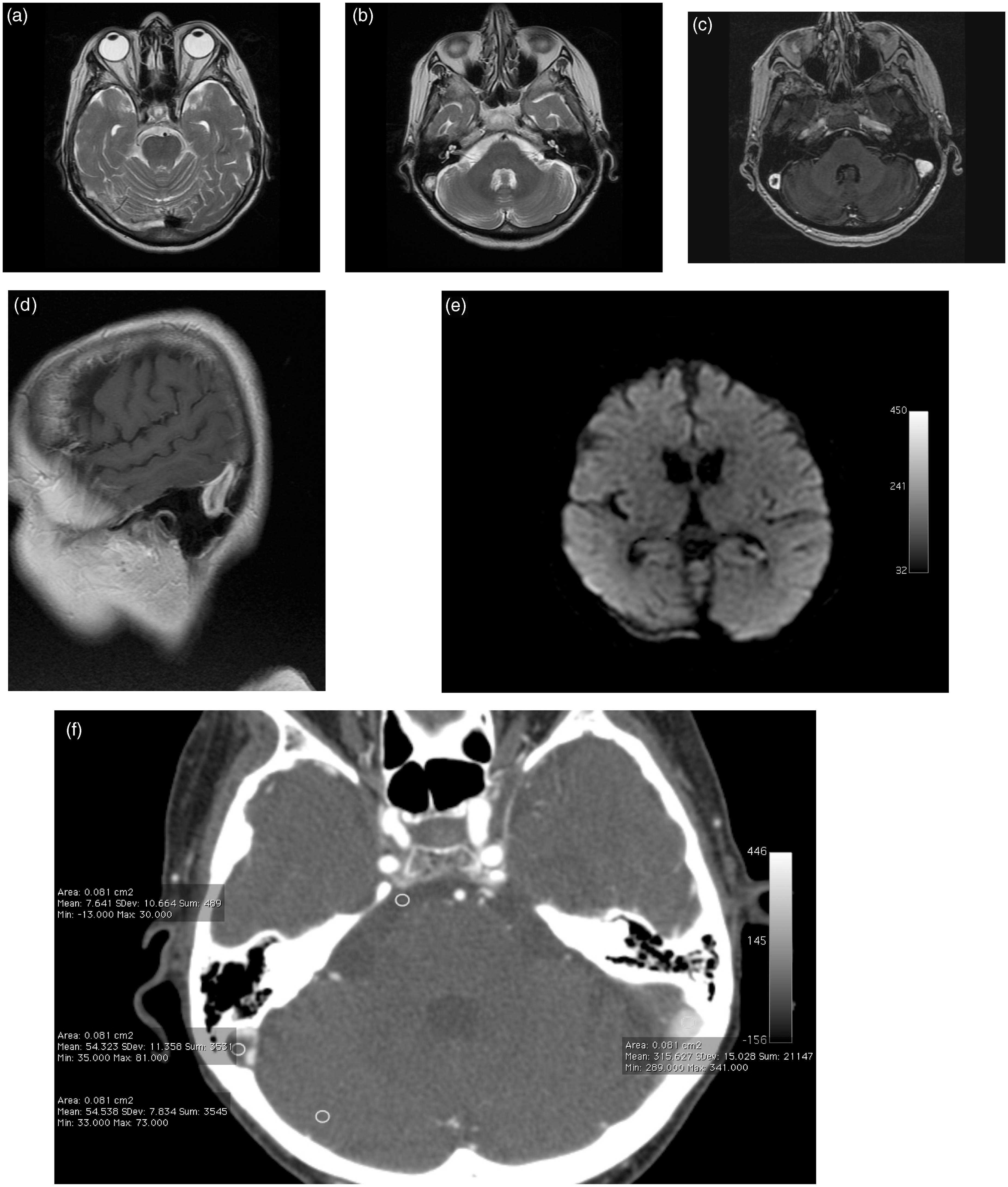
MRI exposes the thrombus in a more sensitive and more specific way. A lack of flow void in blood vessels, typically visible in T1- and T2-weighted images, is a clear indication of decreased blood flow velocity. In extensive thrombosis, a sinus may display an abnormal signal in a long section; similarly, this type of change may be visible in smaller cortical veins. The signal intensity depends on the duration of the clot. For clot visualisation, FLAIR/T2 and T1 imaging is used. Blood metabolites will be revealed in more detail in T2*/gradient echo sequences as more hypointense areas. In the DWI technique, a high signal is often visible in a projection of the sinus with the clot (Figures 2–5). Similar to CT, MRI enables the detection of possible collateral circulation and cerebral changes due to ischaemia and oedema, which are best visible in DWI and FLAIR sequences.4,5
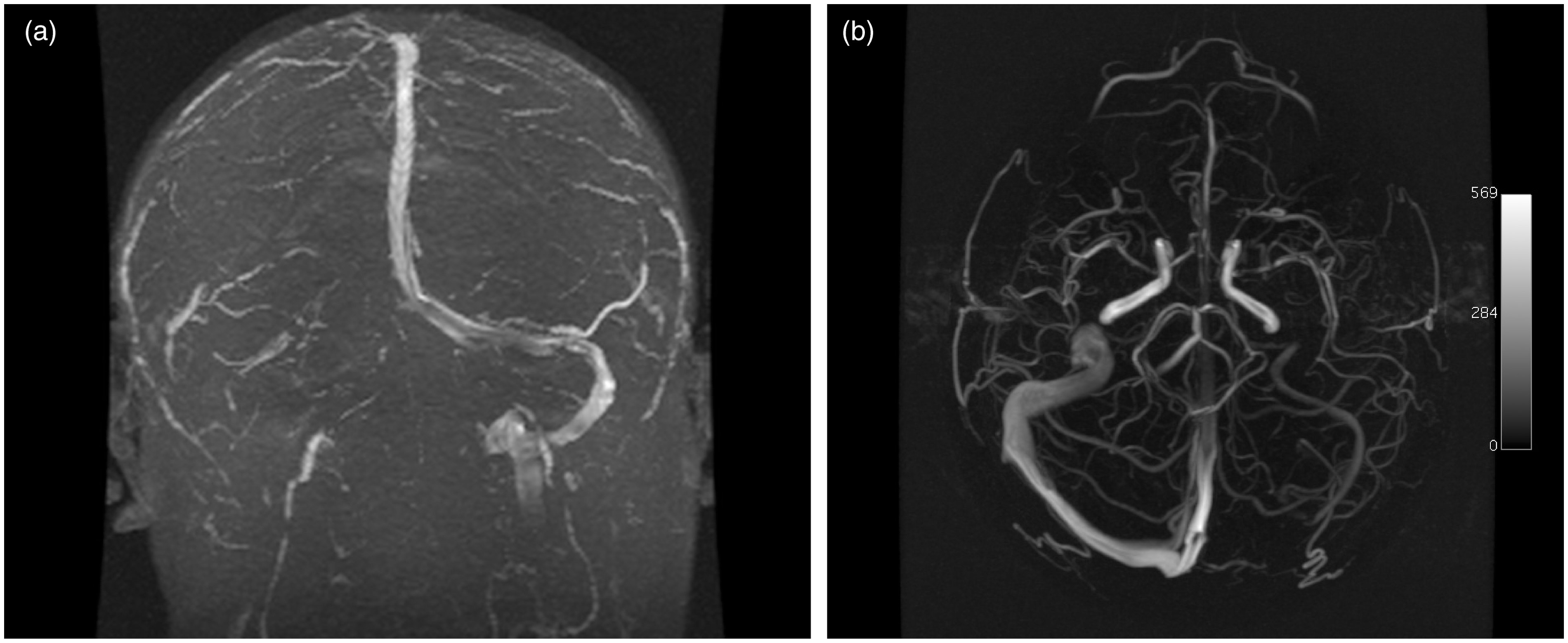
Similar to CT angiography, MRI angiography (usually the TOF method) enables the visualisation of a loss of flow in large venous vessels. The disadvantages of the method are artefacts, disturbances and a lack of signal when the blood flow is too slow or the vessel is too small in diameter (a false positive results in patients with suspected thrombosis; Figure 6). Artefacts of this type are significant due to the frequent tortuosity of venous vessels or to phase blood flow resulting from pressure fluctuations transferred to the venous system while breathing. A subacute, hyperintense clot may produce a high signal in TOF imaging, leading to a false-negative image. For verification purposes, in T1-weighted images, the clot signal will also be abnormally high.4,5,9 In contrast, in T2-weighted images, a hypointense clot may imitate a typical flow void in a vessel. A chronic, organised clot may exhibit a pathologically enhanced signal in T1-weighted contrast images similar to a normally filling contrasted sinus.4,5
MRI angiography with a contrast agent may be performed to visualise the vessels more clearly. However, in non-collaborating patients whose condition is severe, CT angiography will offer higher accuracy due to its greater acquisition speed.
Reactive enhancement of the leptomeninx and cerebral cortex is often evident in both CT and MRI images due to secondary lesions caused by the disruption of the blood-brain barrier.4,5,11
Imaging protocol
The preliminary examination is performed by contrast CT, possibly supplemented with CT angiography. When no conclusion has been obtained, MRI may be used supplemented with MRI angiography and the additional sequences T2*, DWI and T1 +C. If the examinations do not provide a decisive answer, DSA angiography is indicated so that targeted treatment may be introduced.3,11,12 In addition, ultrasound transfontanellar Doppler imaging may be helpful in paediatric cases. 5
Differential diagnosis
A less typical normal image: slightly hyperdense veins in CT imaging without contrast agents (usually in newborns, in whom unmyelinated brain has low density and physiological polycythaemia is frequent). Congenital hypoplasia/aplasia of the transverse sinus. Distinct arachnoid granulations in the sinuses. Acute subdural haematoma as a possible complication or cause of CVST. Brain tumour (with contrast enhancement in the area of venous infarction).
12
Cerebral stroke with a secondary haemorrhagic transformation.
Summary
Because CVST is a rare disease with relatively few specific clinical and radiological symptoms, diagnostic imaging in CVST patients is difficult. A correct radiological diagnosis would greatly contribute to the therapeutic efficacy.
Important
A normal brain image does not exclude thrombosis.
CT imaging for diagnosing CVST should be performed with the administration of a contrast agent.
In newborns, normal, relatively bright sinuses appear similar to thrombosis in CT imaging without a contrast agent.
Contrast agent clinical data are essential for diagnosis in the case of prolonged thrombosis, where contrast enhancement may occur, thus producing an image resembling that of a normal sinus filled with blood.
Thrombotic changes in the transverse sinus on the left side (a) with bilateral secondary lesions of the thalami (b) in CT imaging without a contrast agent. Transverse sinus on the left side and sinus confluence thrombosis (a) T1, (b) T2, (c) T1+C, (d) DWI. Secondary ischaemic changes in the basal ganglia: (e) FLAIR. Otitis media, more visible on the right side, with a complication in the form of transverse/sigmoid sinus thrombosis on the right side: (a) T1, (b) T2, (c) T1. Evolution of changes in follow-up T1 imaging with a transfer into the superior sagittal sinus (the empty delta sign): (d) T1+C. Thrombosis in the transverse sinus on the left side: (a) T1, (b) T2. MRI performed after the treatment: (c) T1, (d) T2. Thrombosis of the transverse sinus, sigmoid sinus and internal jugular vein on the right side: (a, b) T2, (c, d) T1+C, (e) DWI. Follow-up examination 6 months later (permanent lesions): (f) angio-CT transverse scan. Hypoplasia of the transverse sinus, sigmoid sinus and internal jugular vein on the right side: (a) 2D TOF and on the left side: (b) InHance.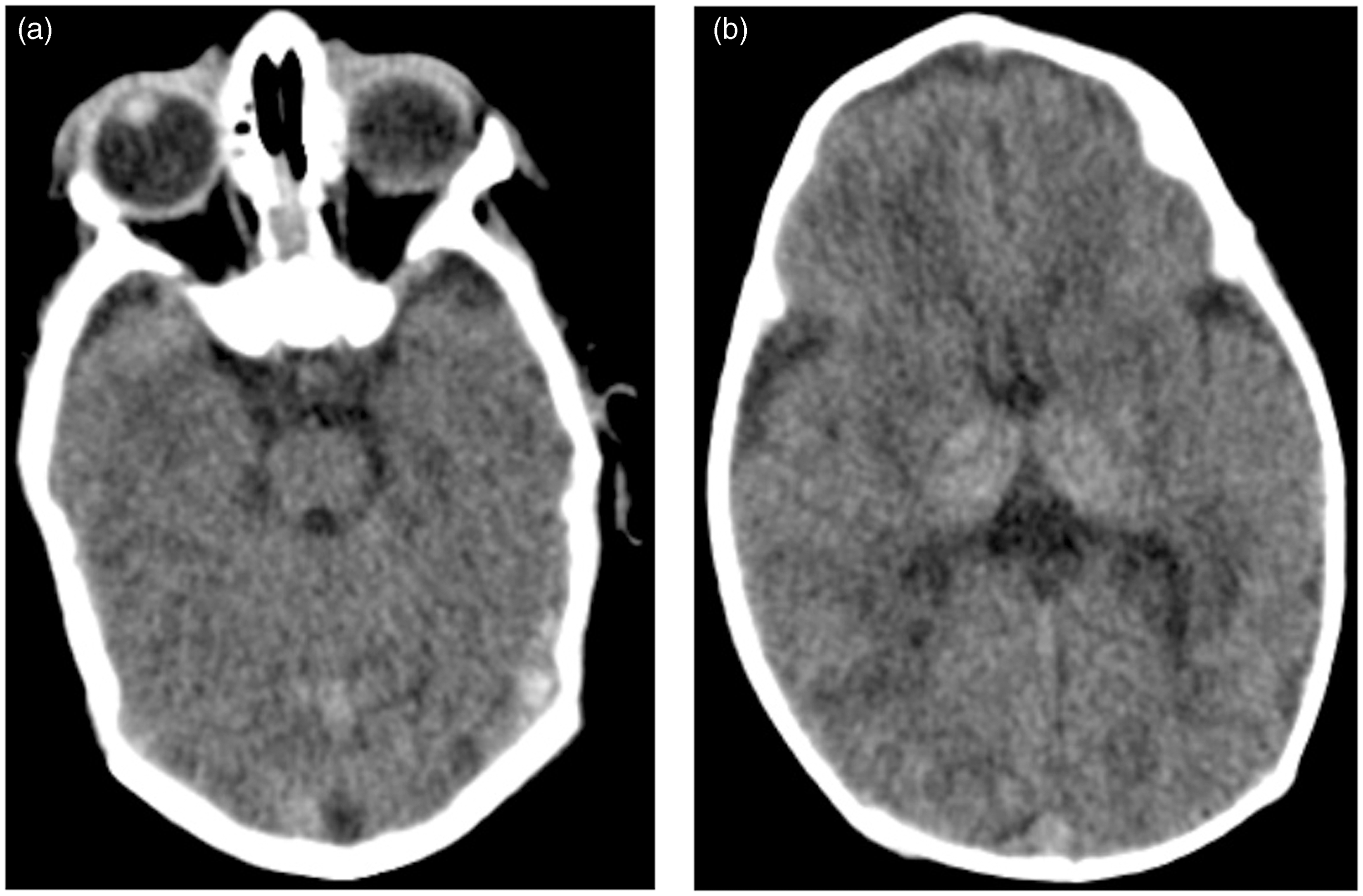

Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.