
Abstract
Objective
To evaluate right iliac vein and left iliac vein compression in asymptomatic subjects, right-sided and left-sided iliofemoral deep vein thrombosis patients.
Methods
A retrospective analysis of records and computed tomography images was conducted in 200 asymptomatic subjects (male:female, 100:100). A prospective analysis was conducted in 79 consecutive deep vein thrombosis patients (left:right deep vein thrombosis, 47:32) who had undergone contrast-enhanced computed tomography examination. The minor diameter and percentage compression of the iliac vein were evaluated.
Results
In asymptomatic subjects, 13.5% had right iliac vein compression >50%, 2.0% had right iliac vein compression >70%, mean compression was 23.48%; 45.0% had left iliac vein compression >50% and 17.0% had left iliac vein compression >70%, mean compression was 47.58%. Right iliac vein sandwiched between the right external iliac artery and the right internal iliac artery was the most common compression pattern (59.26%). Males had higher right iliac vein compression than the females (male:female, 26.29%:20.68%, P < 0.001). Mean percentage compression of the right iliac vein was higher in right deep vein thrombosis patients than in left deep vein thrombosis patients (right:left deep vein thrombosis, 48.54%:22.29%, P < 0.001).
Conclusion
Similar to left iliac vein compression, right iliac vein compression was a frequent imaging finding in CT and represented a normal anatomic pattern. Right deep vein thrombosis patients had more serious right iliac vein compression than left deep vein thrombosis patients, and further research is required on the association of right iliac vein compression with right iliofemoral deep vein thrombosis.
Keywords
Introduction
Iliac vein compression syndrome (IVCS), also known as May–Thurner syndrome or Cockett syndrome, refers to the compression of left iliac vein (LIV) by the right iliac artery against the fifth lumbar vertebrae with iliofemoral deep vein thrombosis (DVT) or signs of venous hypertension in the left lower extremity such as swelling and varicose veins.1–6 In a asymptomatic population, many subjects were found to have compression of LIV in computed tomography (CT) examination without DVT or symptoms of venous hypertension in the left leg.1,7–9 Chan et al. 7 and Carr et al. 8 found that the compression of LIV was a strong independent risk factor for left DVT. For this reason, left-sided iliofemoral DVT was more common than right-sided DVT, and women were more likely than men to have left DVT.1,5,7,10–13
Right-sided IVCS is quite rare. In clinic, we encountered a classic right-sided IVCS case with the right common iliac vein (RCIV) being compressed by the right external iliac artery (REIA) against sacrum, and signs of venous hypertension in the right lower extremity. So we considered whether a certain proportion of asymptomatic population had the right iliac vein (RIV) compression in CT examination, and right-sided iliofemoral DVT patients had obvious RIV compression. In this study, the right-sided IVCS case was exposed, a retrospective analysis in a asymptomatic population and a prospective analysis in right-sided or left-sided iliofemoral DVT patients were conducted to evaluate the compression of RIV and LIV by means of pelvic contrast-enhanced CT examination.
Methods
Study population
The study was conducted at an academic hospital, approved by the institutional review board, and informed consent was obtained from all patients.
A 66-year-old male patient with symptomatic varicosis and pigmentation on the right leg for 25 years was sent to our vascular center. Venous ultrasound Doppler did not show signs of thrombosis. Direct venography revealed severe stenosis of the RIV. To clarify the external compression of RIV, the pelvic contrast-enhanced CT examination was performed.
A retrospective study of medical records and helical abdominal contrast-enhanced CT scans was conducted in 200 subjects with CT imaging for reasons unrelated to DVT between the ages of 18 and 85 years. These subjects were randomly chosen until the first 200 cases were found who met the exclusion criteria. They were selected from consecutively referred patients from 1 January 2013 to 31 December 2014. Patients were excluded if they had a previous history of DVT, the compression of iliac vessels by abnormal arteries such as an aneurysm or other tissue such as tumor tissue evaluated with CT imaging of the pelvis.
Between 1 January 2013 and 31 December 2014, a prospective analysis was conducted in 86 consecutive patients with a first time proximal iliofemoral acute (1–14 days) or subacute (15–28 days) lower extremity DVT that was diagnosed by means of compression ultrasonography or venography combined with D-dimer testing. They did not have bilateral DVT, a previous history of DVT, previous lower-extremity vascular surgical or endovascular vascular procedures. These patients accepted pelvic contrast-enhanced CT studies with contrast material. Patients were excluded if they had the compression of iliac vessels by tumor tissues or other pathological tissues evaluated with CT imaging. At last, 47 patients with left DVT and 32 patients with right DVT remained. Seven patients dropped out of this study, because five patients had the compression of iliac vessels by tumor tissues and two patients had the compression of the iliac vein by the cyst after hysterectomy.
Data collection
CT scans were performed on 64 row multidetectors (General Electric Medical Systems, Milwaukee, WI). Axial CT of 5 mm thickness or less was reviewed. Images were acquired 120–180s after intravenous administration of a 100–120 mL bolus of non-ionic contrast medium. The minor diameter of the iliac vein at the point of maximal compression and percentage compression was assessed in CT cross-sectional images. The degree of iliac vein compression (percentage compressiona) (please see the Table footnotes for a full explanation) was calculated as the minor diameter of the iliac vein at the site of maximal compression divided by the minor diameter of the distal uncompressed iliac vein. As an alternative measurement of degree of iliac vein compression (percentage compressionb), we also calculated as the minor diameter of the iliac vein at the site of maximal compression divided by the minor diameter of the contralateral uncompressed iliac vein at the same level. Measurements were performed independently by two radiologists who were blinded to the subject's clinical presentation.
Statistical analysis
Data were expressed as mean values with their range for continuous variables and percentages for categorical variables. One-sample Kolmogorov–Smirnov test was used to test whether continuous variables fit the normal distribution. Statistical significance was tested by using t tests for normally distributed variables, non-parametric Kolmogorov–Smirnov Z tests for non-normally distributed variables, and Chi-squared tests for categorical variables. A P value < 0.05 was considered to indicate statistical significance. Statistical analysis was carried out using SPSS version 13.0 (SPSS Inc., Chicago, IL, USA).
Results
A right-sided IVCS case
Direct venography revealed the severe compression of RIV with many large collateral veins (Figure 1(a, b)). Pelvic CT confirmed the compression of RIV. RCIV was compressed by REIA against sacrum (Figure 1(c)).
Imaging findings in a patient with right-sided iliac vein compression syndrome. (a), (b) Venography image showing compression of RCIV with many large collateral veins; (c) sequential computed tomography scans showing RCIV was compressed by REIA against the sacrum.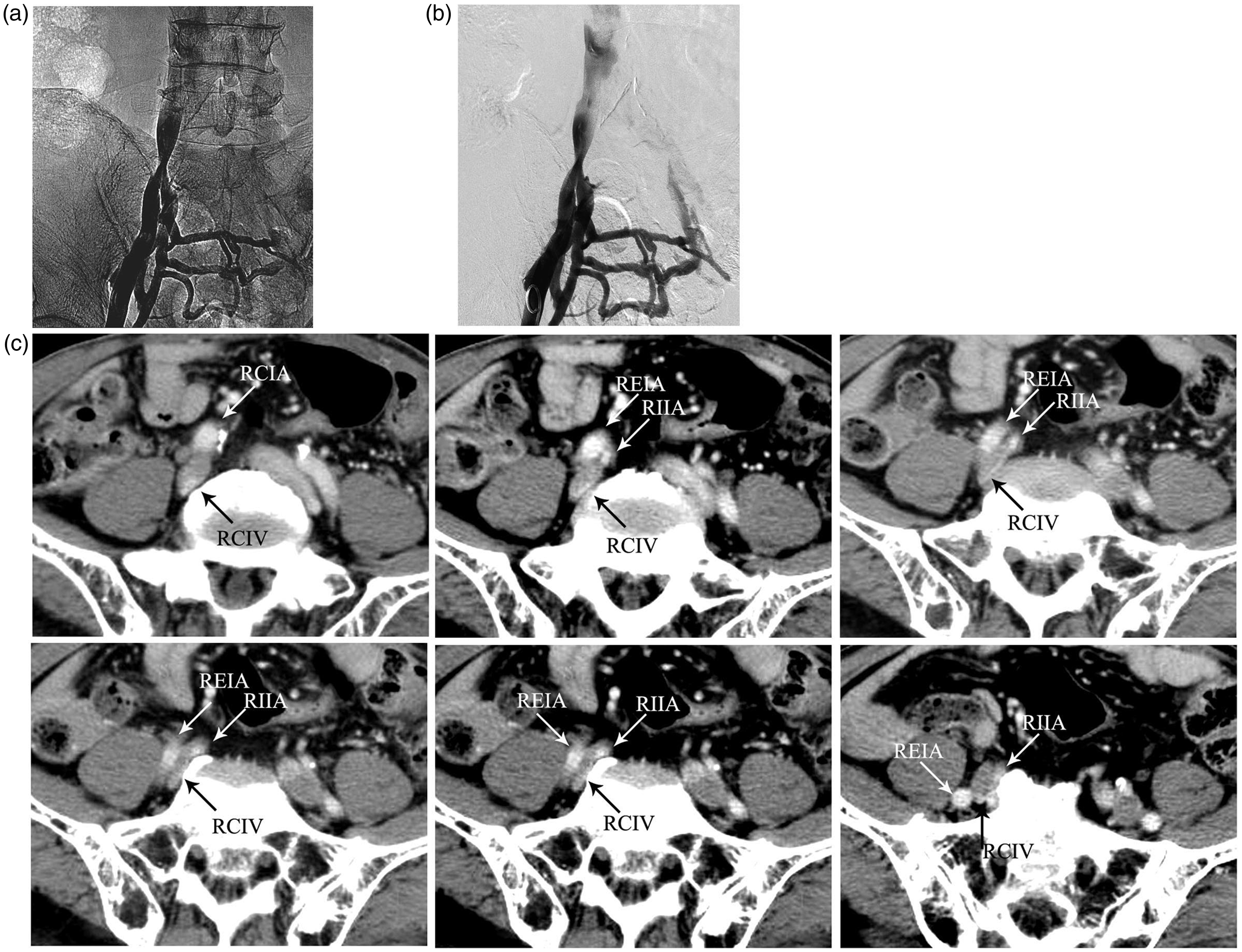
Compression of iliac veins in asymptomatic population
Demographics and iliac vein compression of asymptomatic population.
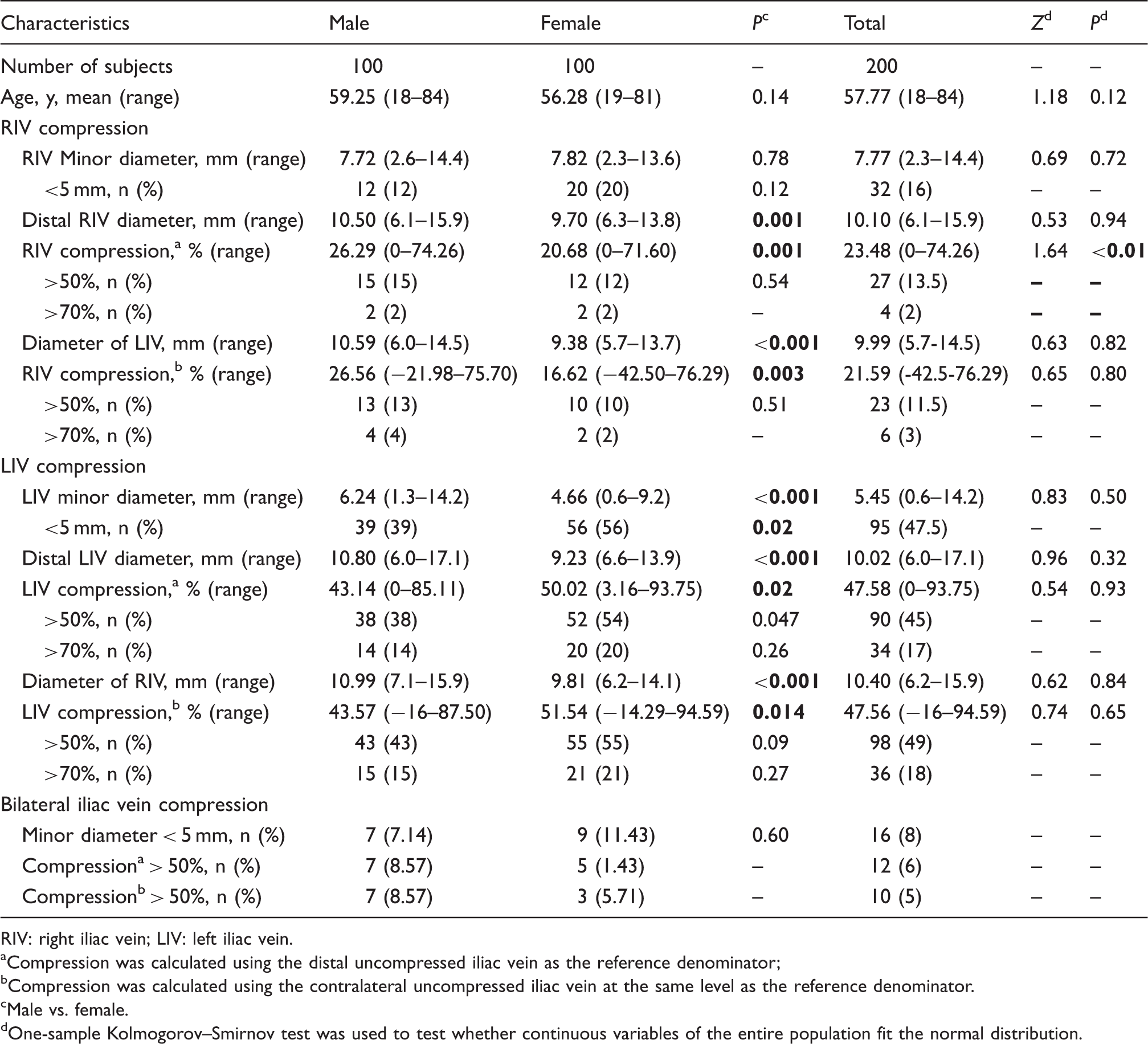
RIV: right iliac vein; LIV: left iliac vein.
Compression was calculated using the distal uncompressed iliac vein as the reference denominator;
Compression was calculated using the contralateral uncompressed iliac vein at the same level as the reference denominator.
Male vs. female.
One-sample Kolmogorov–Smirnov test was used to test whether continuous variables of the entire population fit the normal distribution.
In a total asymptomatic population, the frequency of subjects (n = 27, 13.5%) with RIV compression > 50% was lesser than that of subjects (n = 90, 45.0%) with LIV compression > 50% (P < 0.001), the frequency of subjects (n = 4, 2.0%) with RIV compression > 70% was also lesser than that of subjects (n=34, 17.0%) with LIV compression > 70% (P < 0.001), the ratio of the number of subjects with LIV compression >50% to the number of subjects with RIV compression >50% was 3.33:1 (LIV compression:RIV compression, 90:27, 45.0%:13.5%). Mean compression of RIV (23.48%, 0–74.26%) was lower than that of LIV (47.58%, 0–93.75%, P < 0.001). It seemed that the incidence and percentage compression of the iliac vein were lower in RIV than in LIV.
Males had higher RIV compression than the females (male:female, 26.29%:20.68%, P < 0.001). On the contrary, females had higher LIV compression than the males (female:male, 50.02%:43.14%, P = 0.02). And the number of subjects with LIV compression >50% in females was higher than that in males (female:male, 52:38, P = 0.047).
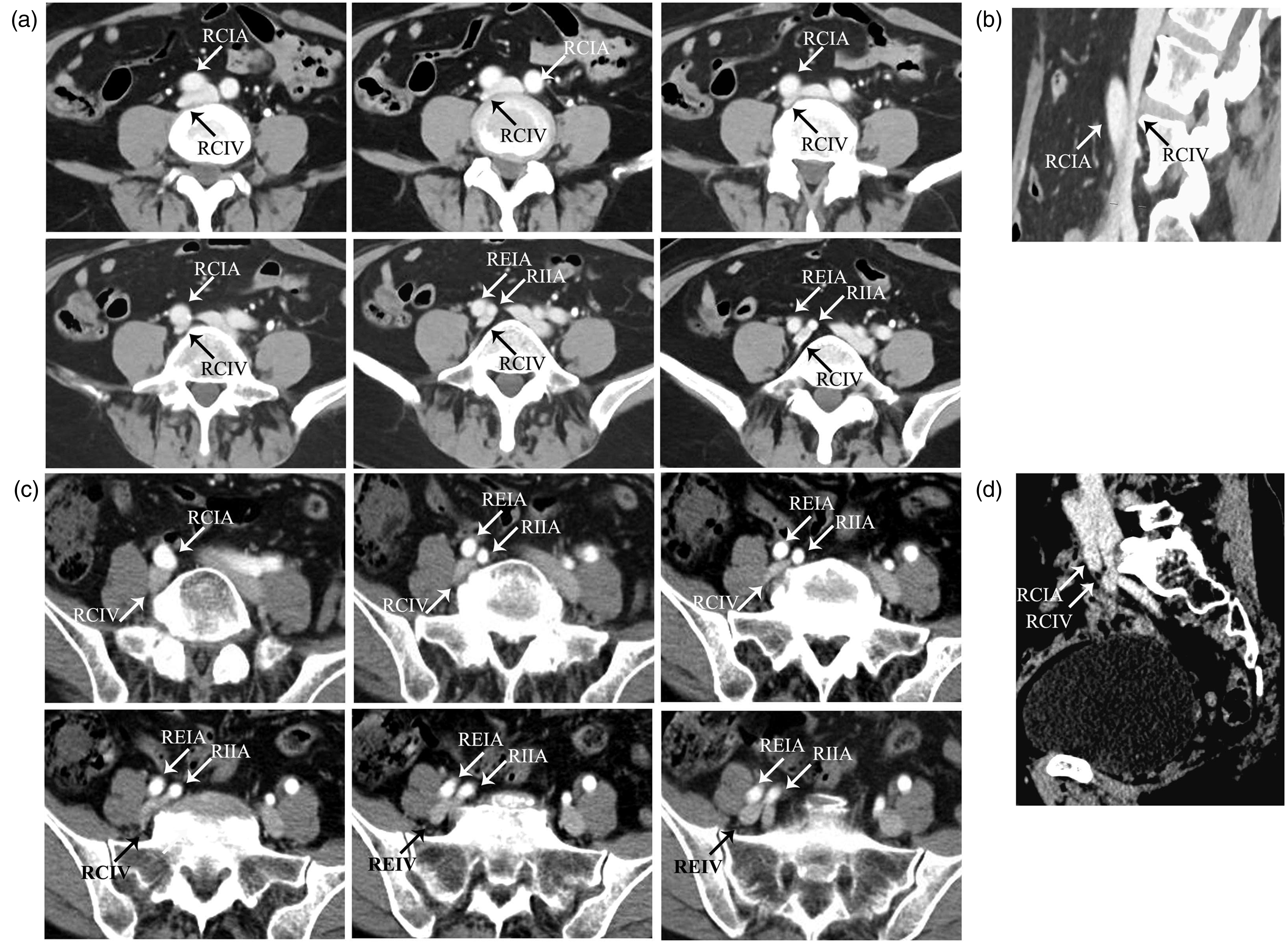
In subjects with RIV compression >50%, three anatomical RIV compression patterns were found: (1) RIV was sandwiched between REIA and right internal iliac artery (RIIA) (Figure 2); (2) RIV was compressed by RIA (including right common iliac artery (RCIA) and REIA) against sacrum (Figure 3); (3) RIV was compressed by RIA (including RCIA, REIA and RIIA) against psoas major muscle (Figure 4). The most common compression pattern was the first one (16/27, 59.26%).
Imaging findings in two subjects without deep vein thrombosis having the compression of RIV. In the first subject, sequential CT scans (a), a venography image (b) and a multiplanar line-of-flow CT scan reconstruction image (c) showed the compression of REIV which was sandwiched between REIA and RIIA. In the second subject, sequential CT scans (d) and a multiplanar line-of-flow CT scan reconstruction image (e) showed compression of REIV which was sandwiched between REIA and RIIA. Imaging findings in two subjects without deep vein thrombosis having the compression of RIV. In the first subject, sequential CT scans (a) and a multiplanar line-of-flow CT scan reconstruction image (b) showed the compression of RCIV which was compressed by RCIA against sacrum. In the second subject, sequential CT scans (c) and a multiplanar line-of-flow CT scan reconstruction image (d) showed the compression of RCIV which was compressed by REIA against sacrum.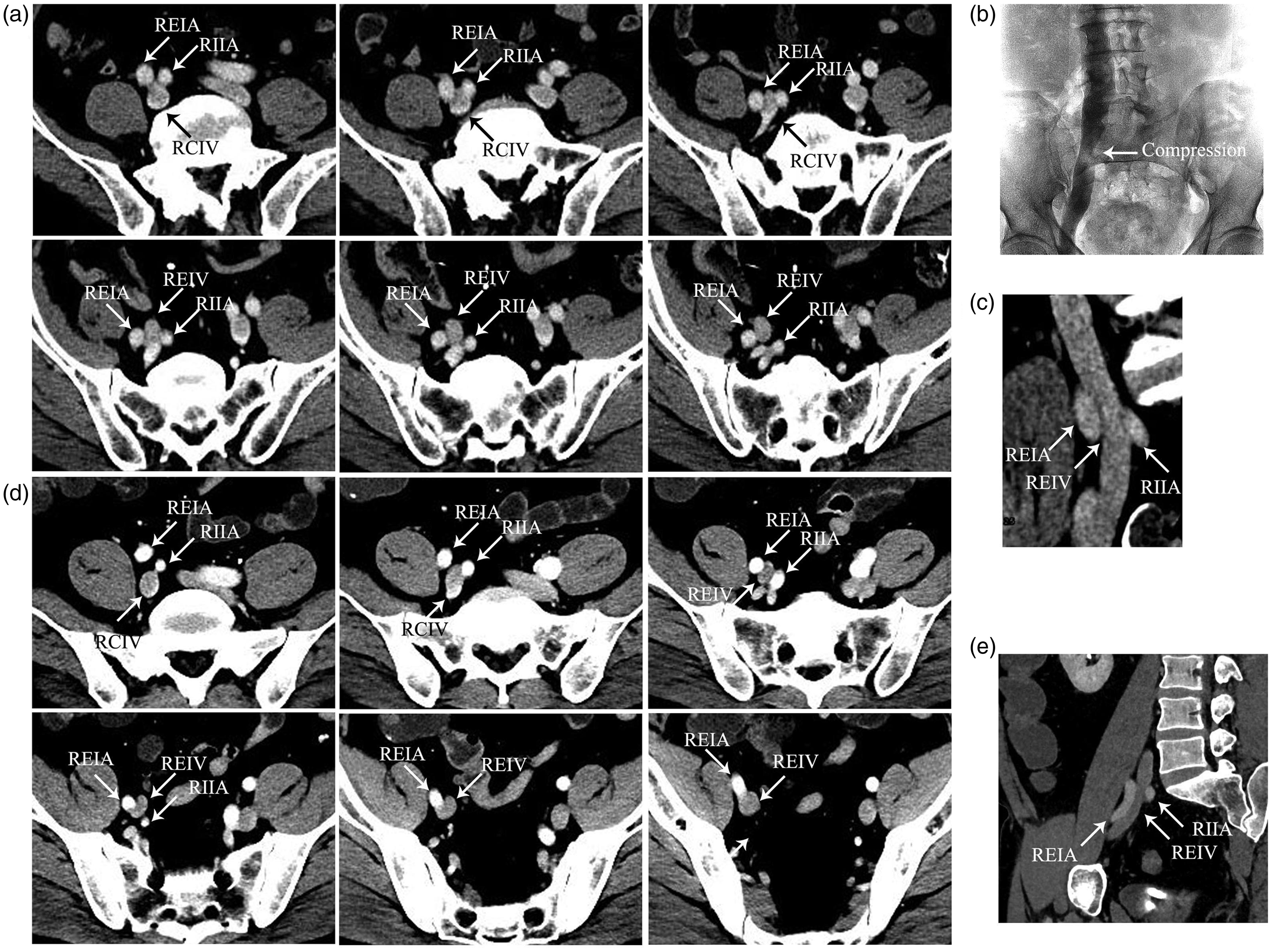
Compression of iliac veins in DVT patients
Demographics, risk factors and iliac vein compression of DVT patients.
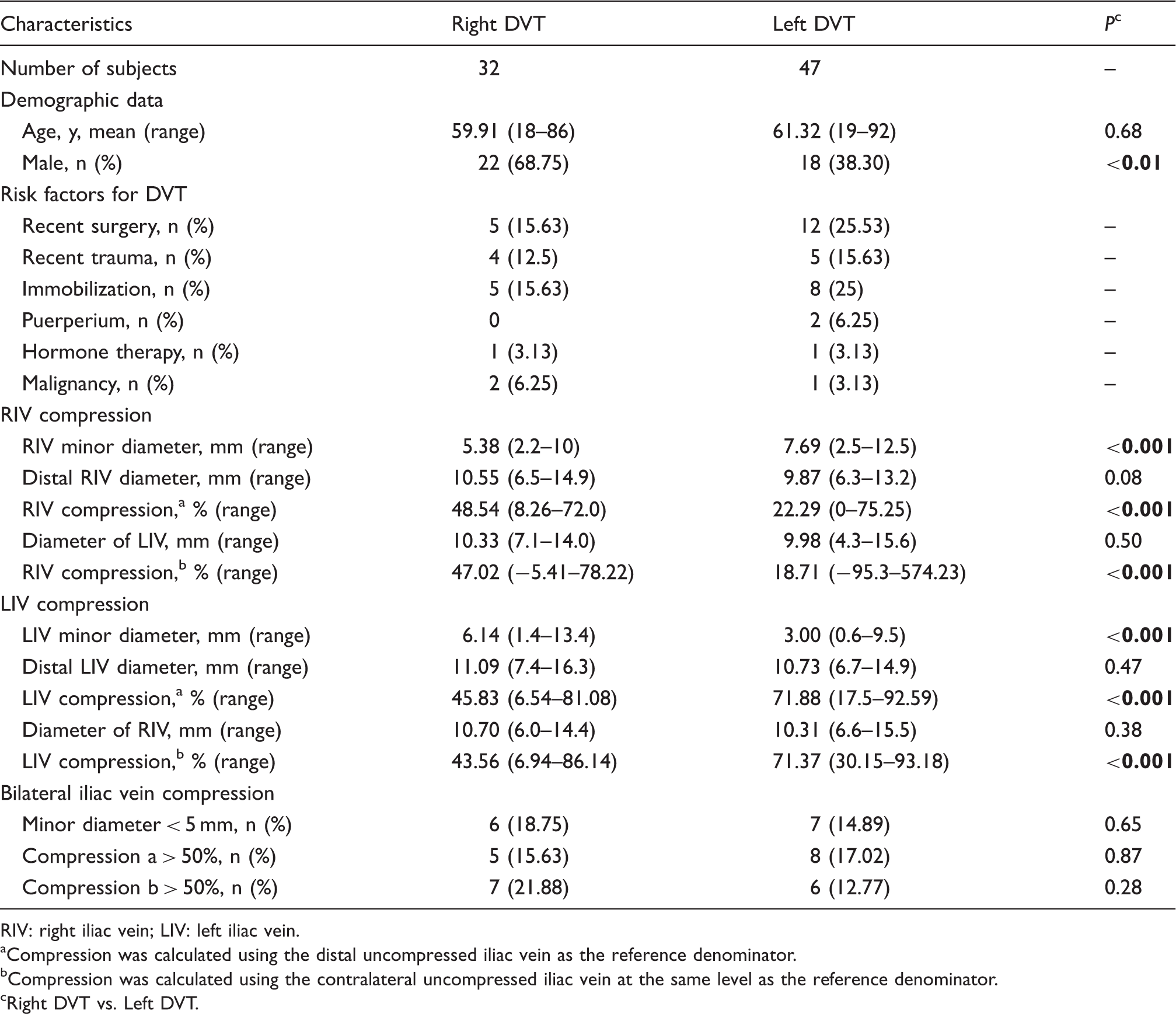
RIV: right iliac vein; LIV: left iliac vein.
Compression was calculated using the distal uncompressed iliac vein as the reference denominator.
Compression was calculated using the contralateral uncompressed iliac vein at the same level as the reference denominator.
Right DVT vs. Left DVT.
Mean minor diameter of RIV was significantly smaller in right-sided DVT patients than in left-sided DVT patients (right DVT:left DVT, 5.38 mm:7.69 mm, P < 0.001), and mean percentage compression was higher in right DVT patients than in left DVT patients (right DVT:left DVT, 48.54%:22.29%, P < 0.001). It seemed that right DVT patients had more excessive RIV compression than left DVT patients.
Similarly, mean minor diameter of LIV was significantly smaller in left DVT patients than in right DVT patients (left DVT:right DVT, 3.00 mm:6.14 mm, P < 0.001), and mean percentage compression was higher in left DVT patients than in right DVT patients (left DVT:right DVT, 71.88%:45.83%, P < 0.001). It seemed that left DVT patients had more excessive LIV compression than right DVT patients.
In right DVT patients, three anatomical RIV compression patterns mentioned above in asymptomatic population were found (Figure 5). Similarly, the most common RIV compression pattern was that RIV sandwiched between REIA and RIIA (14/32, 43.75%).
Sequential computed tomography scans showing that RIV was compressed by RCIA against psoas major muscle in two subjects without deep vein thrombosis. In three right-sided iliofemoral deep vein thrombosis patients, sequential computed tomography scans showed the compression of RIV and filling defect of iliac venous thrombus. (a) RIV was sandwiched between REIA and right internal iliac artery. (b) RIV was compressed by the REIA against the sacrum. (c) RIV was compressed by RCIA and RIIA against psoas major muscle.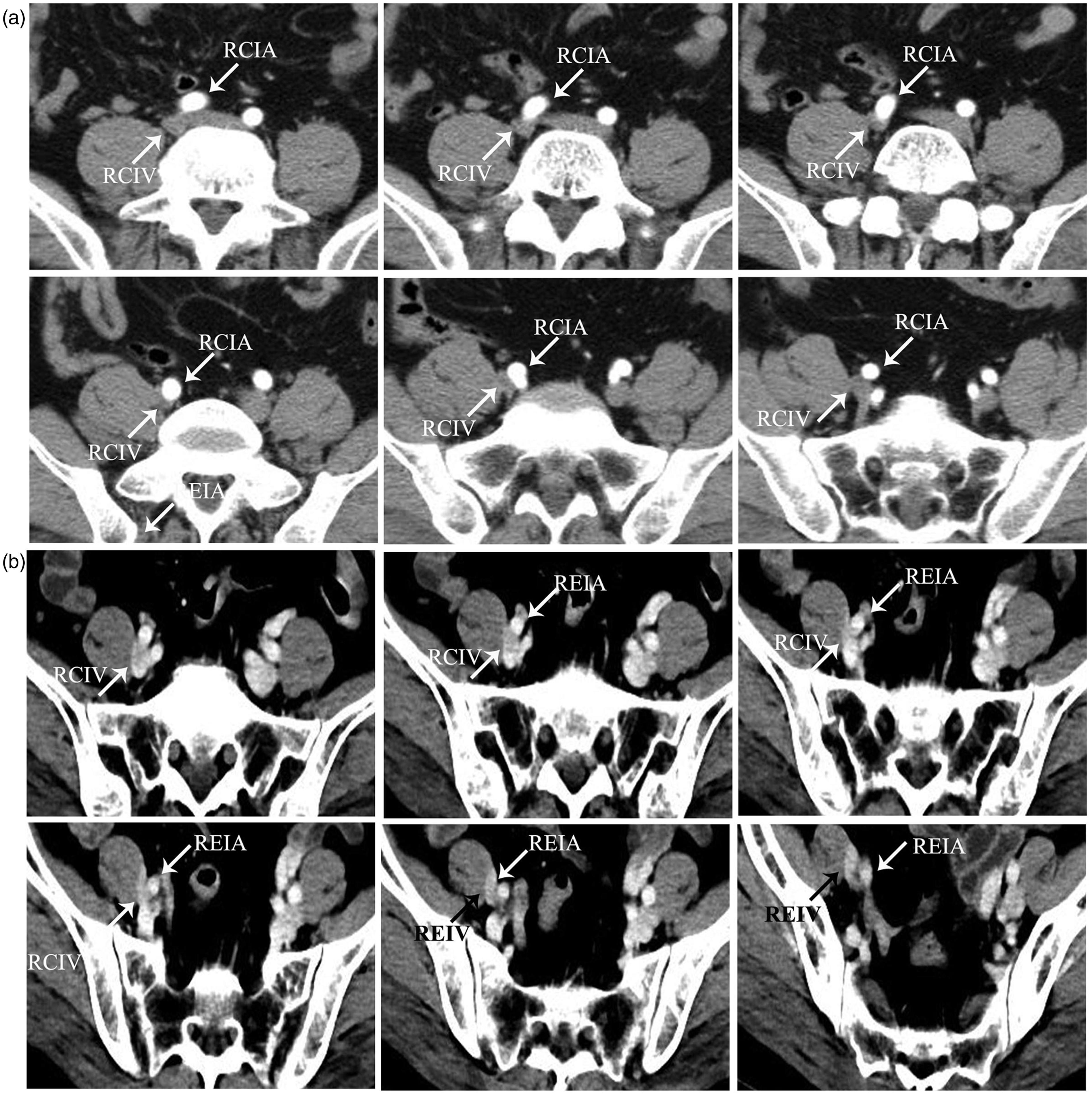

Discussion
IVCS, also known as May–Thurner syndrome or Cockett syndrome, refers to symptomatic extrinsic compression of LIV, caused by right iliac artery against the fifth lumbar vertebrae, with DVT or signs of venous hypertension in the left lower extremity.1–6 Because of this anatomical relationship, many people were found to have compression of LIV in CT examination without DVT or symptoms of venous hypertension in the left leg.1,7–9 But LIV compression in CT examination is not equal to IVCS.3,4 The diagnosis of IVCS must include three factors: firstly, the compression of LIV by RIA; secondly, the presence of tortuous venous collaterals crossing the pelvis to join contralateral veins in venography; thirdly, with DVT or signs of venous hypertension in the left lower extremity such as varicose veins or edema of lower extremity. Right-sided IVCS was rarely reported. Fretz and Binkert 14 reported a case of an atypical compression of the inferior vena cava by the RCIA secondary to a high aortic bifurcation with extensive collateral network. Abboud et al. 15 and Burke et al., 16 respectively, described one case of the RCIV compression by the LCIA with a left-sided inferior vena cava. These three right-sided IVCS cases all had vessel variation. Molloy et al. 17 reported a right-sided IVCS with the compression of the RCIV by RIIA, but the venography and CT data were not obtained. In our study, a classic right-sided IVCS case was reported without any vessel variation. In this case, RCIV was compressed by REIA against the sacrum, and the patient had the venous hypertension signs and the presence of venous collaterals in venography.
The formation of IVCS was considered as the formation of venous spurs (fibrous vascular lesions) in the intimal layer of the vein by the chronic extrinsic compression and pulsing force from the overlying artery. 18 Recently, two studies found that mean compression of LCIV in IVCS with DVT was 68% 19 and 74%, 1 respectively. Maybe only in severe LIV compression patients, the LIV compression in CT examination could develop into IVCS. In this study, 2.0% of subjects had greater than 70% compression of RIV and the highest percentage compression of RIV was no more than 75%. But 17% of subjects had greater than 70% compression of LIV. Severe compression happened more often in LIV than in RIV. It helped explain why right-sided IVCS was rarer than left-sided IVCS.
In asymptomatic subjects, Oguzkurt et al. 19 found mean compression of LCIV was 28% (n = 34), and Kibbe et al. 9 found mean compression of LCIV was 35.5% (n = 50). But Chan et al. 7 found mean compression was 56% (n = 35), and Carr et al. 8 found mean compression was 52% (n = 21). In this study, mean compression was 47.58%. So it was considered that LIV compression represented a normal anatomic pattern that has thus far been thought of as a pathologic condition. In this study, it was found that 27 (13.5%) subjects had greater than 50% compression of RIV in asymptomatic subjects and the mean compression was 23.48%. Similarly, RIV compression also might represent a normal anatomic pattern.
In LIV compression subjects, because of the special anatomical relationship between iliac vessels with lumbar (or sacrum), LIV could be compressed by RCIA, LCIA or LIIA.3,4,6,20 In this study, it was found that RIA (including RCIA and REIA) overlies RIV (including RCIV and REIV) before sacrum or psoas major muscle. RIV could be sandwiched between REIA and RIIA, or be compressed by RIA against sacrum or psoas major muscle. Raju and Neglen 21 also found that compression of RIV by the right iliac arteries with intravascular ultrasound scanning. RIV sandwiched between REIA and RIIA was the most common RIV compression pattern and accounted for 59.26%.
In this study, it was found that the mean percentage compression of LIV was higher in left DVT patients than in right DVT patients. This could be because the compression of LIV was a strong independent risk factor for left iliofemoral DVT.7,8 This anatomically narrowed vasculature can impede blood flow and reduce venous velocity. 18 With the presence of other prothrombotic risk factors, the patients with LIV compression were more likely to get left DVT. In this study, it was also found that the mean percentage compression of RIV was higher in right DVT patients than in left DVT patients. It was speculated whether RIV compression was an independent risk factor for right-sided iliofemoral DVT. And it required further studies.
In a previous study, it was found that left DVT was more common than right DVT. Chen et al. 12 found that the ratio of left-to-right-sided DVT was 3.68:1 (582:158). Ouriel et al. 13 found that the ratio of left-to-right-sided DVT was 1.32:1 overall and 2.4:1 for iliac DVT. In this study, the ratio of subjects with LIV compression >50% to the subjects with LIV compression >50% was 3.33 (LIV compression:RIV compression, 90:27, 45.0%:13.5%). If accounting for the iliac vein compression as an independent risk factor for lower extremity DVT, this difference incidence between LIV compression and RIV compression might explain why lower extremity DVT occurred more commonly in the left leg than in the right leg.
In previous studies, it was found that women accounted for the majority of IVCS and left DVT, while men accounted for the majority of right DVT.5,7,10–12,22,23 In females, the increase in lumbar lordosis that develops during maturation of the female pelvis pushes the lower lumbar vertebra forward, increasing compression of LCIV. This lordosis is even further increased in pregnancy.24,25 Thus, compression of LCIV predisposed left-sided DVT during postpartum and pregnancy period.5,10,11 In this study, males had higher RIV compression than the females. On the contrary, females had higher LIV compression than the males, and the number of subjects with LIV compression >50% in females was higher than that in males. All of these might lead to the gender differences in the incidence of right-sided and left-sided DVT.
This study had several important limitations. First, the data in the first analysis were subjected to all the limitations of a retrospective analysis. Second, CT in the transverse plane was used to assess the extent of iliac vein minor diameter. Ideally, three-dimensional imaging with vessel reconstruction would provide more accurate information with respect to the degree of compression, compared with two-dimensional diameter measurements. Third, the lack of an established reference standard measurement of iliac vein compression prevents us from fully evaluating pelvic CT as a method of diagnosing iliac vein compression.
In conclusion, similar to LIV compression, RIV compression was a frequent imaging finding in CT and a normal anatomic pattern. RIV sandwiched between REIA and RIIA was the most common compression pattern. The incidence and percentage compression of the iliac vein were lower in RIV than in LIV. Males had higher RIV compression than the females. Right DVT patients had more excessive RIV compression than left DVT patients. Further researches were needed to study whether RIV compression was an independent risk factor for right-sided iliofemoral DVT.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.